MANAGEMENT
OF LITHIASIS IN PELVIC KIDNEY THROUGH LAPAROSCOPY-GUIDED PERCUTANEOUS
TRANSPERITONEAL NEPHROLITHOTRIPSY
(
Download pdf )
ALESSE R. DOS SANTOS, DELSON C. B. ROCHA FILHO, LUIS C. F. TAJRA
Center for Advanced Treatment of Urologic Diseases, Santa Maria Hospital (Urocenter), Teresina, Piauí, Brazil
ABSTRACT
We report the case of a patient with pain and an abdominal palpable mass whose tests showed a left pelvic kidney with a 1.5-cm stone in the renal pelvis. We describe the successful management through videolaparoscopy-guided percutaneous transperitoneal nephrolithotripsy, stressing that this method is a therapeutic option in such cases.
Key
words: kidney; pelvic region; lithiasis; percutaneous nephrostomy;
lithotripsy; laparoscopy
Int Braz J Urol. 2004; 30: 32-4
INTRODUCTION
The
treatment of renal lithiasis has undergone a great advance with the advent
of extracorporeal lithotripsy and endourology. The presence of anatomical
anomalies, such as the pelvic kidney, imposes limitations to such therapeutic
procedures (1).
We describe a case of lithiasis in a pelvic
kidney that was successfully treated through videolaparoscopy-guided percutaneous
transperitoneal nephrolithotripsy.
CASE REPORT
Male,
35 year old patient, with abdominal pain for several months and palpable
abdominal mass. Abdominal ultrasonography evidenced left pelvic kidney
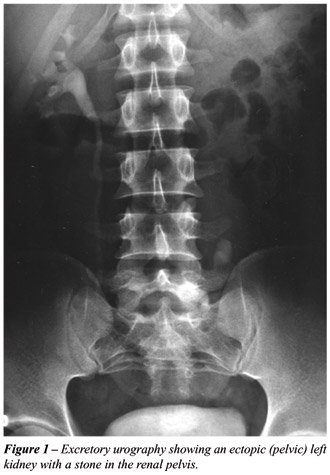
with a 1.5-cm stone in renal pelvis. Excretory urography demonstrated
a functional left pelvic kidney with a delay in excretion of 15 minutes
(Figure-1). The patient underwent transperitoneal videolaparoscopy, with
optics in the right paraumbilical region, after transcystoscopic insertion
of an ureteral catheter. A 5-mm auxiliary trocar was placed in the left
paraumbilical region in order to displace the intestine until the kidney
had been identified. Next, a videolaparoscopy-guided renal puncture and
fluoroscopy with retrograde pyelography were performed, and then followed
by the insertion of a guide wire, dilation of the tract until the insertion
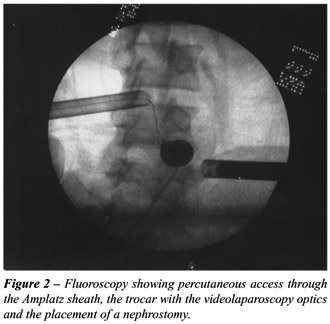
of an Amplatz sheath. A nephroscopy was performed, with identification
of renal stone that was fragmented and removed with ultrasonic lithotriptor,
and the kidney was drained through nephrostomy with a Foley catheter (Figure-2).
The surgical time was 90 minutes. The nephrostomy was removed in the fifth
post-operative day with subsequent discharge from the hospital.
COMMENTS
The
pelvic kidney is the most common form of renal ectopy. Its incidence is
estimated from 1 in 2,200 to 1 in 3,000 in casuistry from necropsies.
The association with lithiasis is small when there is no impairment of
urinary drainage (2).
The renal lithiasis in pelvic kidney can
be managed by means of open surgery, extracorporeal lithotripsy or percutaneous
nephrolithotripsy. Open surgery presents higher morbidity, is less esthetic
due to the incision, and causes more pain post-operatively. Extracorporeal
lithotripsy presents only 54% of success in such cases (2). Percutaneous
surgery has also been proposed, but it is not conducted in a conventional
way (3). It must be performed by anterior abdominal approach because the
pelvic bone structures hinder the posterior access. Additionally, there
is the need for renal puncture and dilation of the tract under direct
viewing with the aid of videolaparoscopy. Thus, the puncture needle is
oriented under direct viewing avoiding any damage to abdominal organs
or major vessels (3). At the end, a nephrostomy is placed, which must
be removed later, decreasing the potential of extravasation of urine to
the peritoneal cavity (3).
In the case reported, the videolaparoscopy
combined with fluoroscopy and retrograde pyelography allowed a good percutaneous
access to the renal stone, which was totally removed without surgical
intercurrences and with no complications. This procedure can be proposed
to patients who have stones in pelvic kidney by a team experienced in
urologic laparoscopy and endourology.
REFERENCES
- Matlaga BR, Assimos DG: The role of open stone surgery in 2002. Int Braz J Urol. 2002; 28: 87-92.
- Paterson RF, Lifshitz DA, Kuo RL, Siqueira Jr TM, Lingeman JE: Shock wave lithotripsy monotherapy for renal calculi. Int Braz J Urol. 2002; 28: 291-301.
- Holman E, Tóth C: Laparoscopically assisted percutaneous transperitoneal nephrolithotomy in pelvic dystopic kidneys: experience in 15 successful cases. J Laparoendosc Adv Surg Tech A. 1998; 8: 431-5.
______________________
Received: August 15, 2003
Accepted after revision: October 15, 2003
_______________________
Correspondence address:
Dr. Luis Carlos Feitosa Tajra
Hospital Santa Maria
Rua Governador Artur de Vasconcelos, 616
Centro / Sul, Teresina, PI, 64001-450, Brazil
Fax: + 55 86 223-1935
E-mail: lcftajra@uol.com.br
EDITORIAL COMMENT
The
best treatment for stones in pelvic ectopic kidney has not been clearly
established yet. Videolaparoscopy, in the case described above, enabled
percutaneous surgery avoiding the risk of damage to the intestine that
could be on the percutaneous tract.
The following question can be made: why
not to continue with the laparoscopic method, performing a pyelolithotomy
(laparoscopic), avoiding the association of procedures (percutaneous and
laparoscopic)?
Those who have already performed a laparoscopic
pyelolithotomy in a pelvic kidney know that it is usually a difficult
and prolonged surgery for some reasons: 1) There is no standardization
about the sites for placement of trocars and not always the optics and
the working instruments are properly positioned; 2) Depending on the side
and the ectopic location of the kidney, the displacement and mobilization
of the colon can be necessary; 3) Smaller working space compared to the
upper portion of the abdomen; 4) The peripyelitis, frequent in such cases,
can represent the greatest difficulty of all.
The renal pelvis is covered by a thick layer
of inflammated fat tissue where the surgeon becomes uncertain about where
to incise and is afraid to damage any vessel from the renal pedicle. The
open surgery for the stone provides guidance on the incision of the fat
tissue and the renal pelvis. The inflammatory reaction makes this perception
difficult during laparoscopic surgery (palpation), as well as the exposition
of the renal pelvis (inspection).
Therefore, even for those who are familiar
with laparoscopic surgery, the association proposed in this wok is an
appealing alternative to open surgery.
Dr.
Anuar Ibrahim Mitre
Division of Urology
University of São Paulo
São Paulo, SP, Brazil