PROGNOSTIC
VALUE OF THE PERCENTAGE OF POSITIVE FRAGMENTS IN BIOPSIES FROM PATIENTS
WITH LOCALIZED PROSTATE CANCER
(
Download pdf )
ALBERTO A. ANTUNES, MARCOS F. DALL’OGLIO, ALEXANDRE C. SANT’ANNA, MARIO PARANHOS, KATIA R. M. LEITE, MIGUEL SROUGI
Division of Urology, Paulista School of Medicine, Federal University of Sao Paulo, UNIFESP, Sao Paulo, SP, Brazil
ABSTRACT
Objective:
To assess the prognostic value of the percentage of positive fragments
(PPF) in biopsies from patients with localized prostate cancer (PCa) undergoing
radical prostatectomy.
Materials and Methods: During the period
from March 1991 to November 2000, 440 patients were selected. Cases receiving
neoadjuvant or adjuvant hormone therapy, or adjuvant radiotherapy, were
excluded, as were cases presenting Gleason scores higher than 6 at biopsy.
PPF was defined as the total number of fragments divided by the total
number of biopsy fragments times 100. This variable was initially divided
into categories from 0 to 25%, 25.1% to 50%, 50.1 to 75% and 75% to 100%.
During the postoperative period, patients were assessed every 2 months
for 1 year, then every 6 months for 5 years, and then yearly. Biochemical
recurrence was defined as serum PSA higher than or equal to 0.4 ng/mL.
Median follow-up was 60 months.
Results: One hundred and nine (24.8%) of
the 440 patients under study had biochemical recurrence. In the univariate
analysis, PPF significantly influenced disease-free survival (log-rank,
p < 0.001), and patients with PPF between 75 and 100% presented a risk
of a biochemical recurrence of the disease 3 times higher than patients
with PPF between 0 and 25% (p < 0.001). After the Cox regression analysis,
both serum PSA (p = 0.001) and PPF (p < 0.001) showed to be independent
predictive factors for disease-free survival following surgery.
Conclusion: PPF measurement in biopsy is
a simple and practical method, which should be routinely used as a predictive
factor for biochemical recurrence in patients with PCa presenting Gleason
scores between 2 and 6.
Key
words: prostatic neoplasms; biopsy; needle; neoplasm staging
Int Braz J Urol. 2005; 31: 34-41
INTRODUCTION
Currently,
50% of patients with localized prostate cancer (PCa) are treated with
radical prostatectomy (1); however, the finding of organ-confined cancer
in the surgical specimen does not guarantee postoperative biochemical
control of the disease. Thus, approximately 30% of patients undergoing
radical prostatectomy will present an increase in prostate specific antigen
(PSA) on long term (2).
Currently, the biopsy’s histological
grade along with the PSA and clinical staging (American Joint Committee
on Cancer - AJCC, 1992) are the most frequently used pre-operative prognostic
variables for identifying patients with a higher risk of presenting organ-confined
disease in the surgical specimen (3).
More recently, studies have demonstrated
that greater detailing of pathological data obtained from prostate biopsy,
in addition to merely identifying cancer and assessing its histological
grade, can improve diagnostic accuracy in these patients. Thus, the percentage
of fragments with cancer (PPF) has been widely used as a predictive factor
for tumor volume, extracapsular extension, invasion of seminal vesicle,
lymph nodal involvement and percentage of fragments with Gleason score
4 and 5 (4-8).
PPF has been used as well to predict postoperative
risk of biochemical recurrence (9-14). Presti et al. (9) defined that
Gleason score for biopsy and PPF are the most important predictive factors
for postoperative biochemical recurrence. D’Amico et al. (10) divided
patients into risk groups based on classic parameters (PSA, Gleason score
and clinical staging), and during a 4-year follow-up, observed that, among
patients from the low risk group, 25% and 10% had biochemical recurrence
when the PPF was higher or lower than 50% respectively.
However, most studies assessing the prognostic
value of PPF have limitations. All of them involve at least 2 centers
and, thus, surgical procedures and pathological analyses were performed
by a heterogeneous group of professionals. Moreover, they have a limited
follow-up with a median of 38.5 months (maximum 46 months), and finally,
they do not show an agreement concerning the ideal cut-off points that
should be considered when analyzing the PPF (11-14).
The objective of this study is to assess
the prognostic value of PPF for biochemical recurrence in patients with
low-grade PCa undergoing radical prostatectomy.
MATERIALS AND METHODS
From
March 1991 to November 2000, we selected 440 patients with localized prostate
cancer undergoing radical prostatectomy at our institution. When selecting
this group, those cases receiving neoadjuvant or adjuvant hormone therapy
(14 patients), and adjuvant radiotherapy (1 patient) were excluded, as
were cases presenting Gleason score higher than 6 at biopsy; thus, the
inclusion criterion was a Gleason score < 6 at biopsy. All surgical
procedures were performed by the same surgeon and pathology analyses by
the same pathologist.
During staging, all patients underwent anamnesis
and physical examination, dosing alkaline phosphatase, total and prostatic
acid phosphatase, serum PSA, pelvic computerized tomography and bone scintigraphy,
aiming to rule out any signs of extraprostatic disease. Diagnoses were
made through transrectal biopsy of the prostate motivated by increases
in serum PSA or changes in the digital rectal examination. Postoperatively,
patients were assessed every 2 months for 1 year, then every 6 months
for 5 years, and then yearly. During each assessment, patients underwent
digital rectal examination of the prostate cavity and analysis of serum
PSA. Imaging studies were repeated every year. Biochemical progression
was defined as a serum PSA higher or equal to 0.4 ng/mL, a cut-off value
also instituted by other authors (15). Median follow-up was 60 months
(2 – 130.5 m). Only four patients (0.9%) were lost during follow-up.
The patients’ mean age was 62.5 ± 7.4 years, ranging from
40 to 79 years.
Clinical staging was defined according to
the AJCC classification, 1992 (16), and histological grade according to
the Gleason score (17). Serum PSA was divided into categories from 0 to
4 ng/mL, 4.1 to 10 ng/mL, 10.1 to 20 ng/mL and higher than 20 ng/mL. The
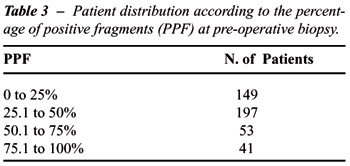
PPF was defined as the total number of fragments with cancer divided by
the total number of fragments in biopsy times 100. This variable was divided
into categories from 0 to 25%, 25.1% to 50%, 50.1 to 75% and 75% to 100%.
The patient distribution according to clinical
staging is listed on Table-1. Tables-2, 3 and 4 stratify patients according
to pre-operative PSA, PPF and the pathological stage of the surgical specimen
respectively.
A survival analysis approach was used for
the statistical analysis considering a biochemical recurrence of the disease
as the event of interest. This was defined by a PSA value higher or equal
to 0.4 ng/mL. For disease-free survival curves, the Kaplan-Meier method
and the log-rank test were used for comparing the curves of percentage
of affected fragments. On the multivariate analysis, a Cox proportional-hazards
regression model was adjusted. The assumption of proportional risks in
the adopted model was checked by construction log-minus-log graphs, which
did not indicate violation of the proportional hazard assumption. P values
p < 0.05 were considered statistically significant.
RESULTS
During
a median follow-up period of 60 months (2 – 130.5 m), 109 (24.8%)
of the 440 patients under study presented biochemical recurrence. Figure-1
shows the mean disease-free survival time estimated at 97 months with
95% confidence interval. We can observe that at 116 months, the likelihood
of a patient being disease-free was approximately 50.7%.
The number of biopsied fragments ranged
from 2 to 19, with means and medians of 7.01 and 6.0 fragments respectively,
with 40.6% of fragments affected by cancer.
On the univariate analysis, Table-5 shows
the patient distribution according to the cut-off points for PPF and the
probability of biochemical recurrence. We can observe that more than one
half of patients presenting PPF > 75% had biochemical recurrence. Figure-2
shows the disease-free survival curves in relation to PPF according to
predefined cut-off points. We observe that PPF significantly influenced
disease-free survival (log-rank, p < 0.001).
After Cox regression analysis to control
for pre-operative serum PSA, we observed that both serum PSA and PPF were
independent predictive factors for disease-free survival in the post-operative
period (Table-6).
COMMENTS
This
study demonstrated that the PPF at biopsy could influence postoperative
biochemical recurrence in patients with Gleason scores between 2 and 6
undergoing definitive treatment by radical prostatectomy. Thus, patients
who have 0 to 25% and more than 75% of fragments affected present 15%
and 54% of biochemical recurrences respectively. Additionally, in the
multivariate analysis controlling for pre-operative serum PSA, the PPF
at biopsy was the strongest predictive factor for determining biochemical
recurrence, adding prognostic information in the group of patients under
study.
Pathological data obtained from prostate
biopsies have been poorly explored. In clinical practice, we can observe
that information obtained only through pre-operative analysis of serum
PSA, the biopsy’s Gleason scores and clinical staging are often
insufficient to predict the pathological staging of the surgical specimen
and the disease-free survival in patients undergoing definitive treatment
by radical prostatectomy (3).
In this context, several studies have demonstrated
that PPF provides additional information for the post-operative pathological
findings and clinical features of patients undergoing radical prostatectomy.
One analysis of 104 patients with a mean age of 61 found a significant
association between the number of affected fragments by prostate lob on
the sextant biopsy and an extracapsular extension of PCa. Thus, extracapsular
extension occurred in 9%, 12%, 32% and 40% of the sides presenting zero,
1, 2 and 3 of 3 fragments affected respectively (5). Other authors observed
that the probability of metastases in pelvic lymph nodes was 5% and 30%
when 3 and 6 fragments were affected respectively. They also observed
a higher incidence of Gleason scores 4 and 5 with the increased number
of affected fragments. As for logistic regression analysis, this was the
best predictive factor for lymph nodal status (6). Finally, Gancarczyk
et al. (8), in studies about the prognostic value of PPF at biopsy for
determining the post-operative pathological staging in 1510 patients from
the Center for Prostate Disease Research through uni- and multivariate
analysis, divided the PPF into 3 categories: less than 30%, from 30 to
59% and equal to or higher than 60%. The authors observed that the PPF
combined with the pre-operative serum PSA and Gleason scores at biopsy
were the most important predictive factors for the pathological staging
of the surgical specimen. Based on these findings, they included the PPF
in a probability nomogram for predicting post-operative pathological findings
in such patients.
PPF has also been used for predicting the
post-operative biochemical progression in patients undergoing radical
prostatectomy. A retrospective study of 1094 patients from 4 institutions
in the SEARCH database who were treated by radical prostatectomy defined
that the PPF was an independent prognostic variable for determining post-operative
pathological findings and biochemical recurrences. The study used 3 cut-off
points for PPF – less than 34%, 34 to 50% and more than 50% –
and when the study population was divided into risk groups based on the
classic parameters (serum PSA, Gleason scores at biopsy and clinical staging),
PPF provided additional prognostic information for patients with low and
moderate risk, but did not add any information for the high-risk group
(12).
Subsequently, this same group compared the
ability of predicting biochemical recurrence in the PPF of the entire
gland with the PPF of the lobe that was most affected by PCa (13). With
a mean follow-up of 27 months, this multivariate analysis showed that
the PPF of the dominant side was the strongest predictive factor for post-operative
biochemical recurrence. Thus, it would be worse for a patient to have
80% positive fragments in one lobe and 0% in the other, than to have 40%
positive fragments in each lobe.
More recently, Lotan et al. (14), found
a strong association between PPF and the tumor stage, histological differentiation,
biochemical progression, distant metastases and overall survival. After
assessing 630 patients with mean age of 60.4 years and mean pre-operative
PSA of 8.1 ng/mL who were followed for 21.2 months after radical prostatectomy,
13% of the patients presented disease progression. Patients with a PPF
higher than 25% had their disease-free survival estimated at 70% versus
90% when the PPF was lower or equal to 25%. PPF was associated with biochemical
recurrence on the pre- and post-operative multivariate analysis.
However, despite all these results, the
most accurate method for quantifying tumor volume in the prostate biopsy
is still grounds for debate. Some studies have shown that more detailed
analyses of prostate biopsies, such as the total percentage of cancerous
tissue or a higher percentage of cancer in one affected fragment, are
the most adequate methods for measuring tumor volume in prostate biopsies
(18,19). In the series from Freedland et al. (18), the percentage of cancerous
tissue at biopsy was a stronger predictive factor for post-operative biochemical
recurrence than PSA and Gleason scores at biopsy. It was also predictive
of the involvement of seminal vesicle and extraprostatic disease. On the
other hand, the measurement of tumor volume through these methods is more
laborious and not all pathologists provide this information. The PPF measurement
as performed in this study seems to be easier and more practical. Additionally,
there is research showing that PPF was a stronger predictive factor for
biochemical recurrence than the total percentage of tissue affected by
carcinoma at biopsy, and the latter did not add any prognostic information
to the former in patients from the intermediary-risk group (20,21). In
fact, the best method for estimating tumor volume through biopsy still
has to be established by controlled studies comparing these methods.
A limiting factor in series presented so
far is the short follow-up period. With the present study, prognostic
data highlighted in the worldwide literature were ratified, with a median
follow-up of 5 years, adding at least 14 months to the follow-up period
in the longer series. Additionally, new cut-off points were defined for
PPF that were shown to present statistical significance, which, therefore,
can be employed in clinical practice. Since the categories of 25.1% to
50%, and 50.1% to 75% had similar disease-free survival curves (Figure-2)
and did not present statistical difference when compared to the category
from 0 to 25% (Table-5, p > 0.122), in practical terms the cut-off
points could be divided into lower than 25%, 25.1% to 75% and higher than
75%. Finally, the authors emphasize that the PPF measurement at biopsy
is a simple and practical method that should be routinely used as a predictive
factor for biochemical recurrence in patients with PCa who have Gleason
scores from 2 to 6.
_________________________________________
Adriana Sanudo performed the statistical analysis
REFERENCES
- Cooperberg MR, Broering JM, Litwin MS, Lubeck DP, Mehta SS, Henning JM, et al.: The contemporary management of prostate cancer in the United States: lessons from the cancer of the prostate strategic urologic research endeavor (CapSURE), a national disease registry. J Urol. 2004; 171: 1393-401.
- Hull GW, Rabbani F, Abbas F, Wheeler TM, Kattan MW, Scardino PT: Cancer control with radical prostatectomy alone in 1,000 consecutive patients. J Urol. 2002; 167: 528-34.
- Partin AW, Kattan MW, Subong EN, Walsh PC, Wojno KJ, Oesterling JE, et al.: Combination of prostate-specific antigen, clinical stage, and Gleason scores to predict pathological stage of localized prostate cancer. A multi-institutional update. JAMA. 1997; 277: 1445-51. Erratum in: JAMA. 1997; 278: 118.
- Furuya Y, Fuse H, Nagakawa O, Masai M: Preoperative parameters to predict tumor volume in Japanese patients with nonpalpable prostate cancer. Int J Clin Oncol. 2002; 7: 109-13.
- Borirakchanyavat S, Bhargava V, Shinohara K, Toke A, Carroll PR, Presti JC Jr.: Systematic sextant biopsies in the prediction of extracapsular extension at radical prostatectomy. Urology. 1997; 50: 373-8.
- Conrad S, Graefen M, Pichlmeier U, Henke RP, Hammerer PG, Huland H: Systematic sextant biopsies improve preoperative prediction of pelvic lymph node metastases in patients with clinically localized prostatic carcinoma. J Urol. 1998; 159: 2023-9.
- Ravery V, Schmid HP, Toublanc M, Boccon-Gibod L: Is the percentage of cancer in biopsy cores predictive of extracapsular disease in T1-T2 prostate carcinoma? Cancer. 1996; 78: 1079-84.
- Gancarczyk KJ, Wu H, McLeod DG, Kane C, Kusuda L, Lance R, et al.: Using the percentage of biopsy cores positive for cancer, pretreatment PSA, and highest biopsy Gleason sum to predict pathologic stage after radical prostatectomy: the Center for Prostate Disease Research nomograms. Urology. 2003; 61: 589-95.
- Presti JC Jr, Shinohara K, Bacchetti P, Tigrani V, Bhargava V: Positive fraction of systematic biopsies predicts risk of relapse after radical prostatectomy. Urology. 1998; 52: 1079-84.
- D’Amico AV, Whittington R, Malkowicz SB, Schultz D, Fondurulia J, Chen MH, et al.: Clinical utility of the percentage of positive prostate biopsies in defining biochemical outcome after radical prostatectomy for patients with clinically localized prostate cancer. J Clin Oncol. 2000; 18: 1164-72.
- Grossfeld GD, Latini DM, Lubeck DP, Broering JM, Li YP, Mehta SS, et al.: Predicting disease recurrence in intermediate and high-risk patients undergoing radical prostatectomy using percent positive biopsies: results from CaPSURE. Urology. 2002; 59: 560-5.
- Freedland SJ, Aronson WJ, Terris MK, Kane CJ, Amling CL, Dorey F, et al. and The SEARCH Database Study Group: The SEARCH Database Study Group. Percent of prostate needle biopsy cores with cancer is significant independent predictor of prostate specific antigen recurrence following radical prostatectomy: results from SEARCH database. J Urol. 2003; 169: 2136-41.
- Freedland SJ, Aronson WJ, Terris MK, Kane CJ, Amling CL, Dorey F, et al.: The percentage of prostate needle biopsy cores with carcinoma from the more involved side of the biopsy as a predictor of prostate specific antigen recurrence after radical prostatectomy: results from the Shared Equal Access Regional Cancer Hospital (SEARCH) database. Cancer. 2003; 98: 2344-50.
- Lotan Y, Shariat SF, Khoddami SM, Saboorian H, Koeneman KS, Cadeddu JA, et al.: The percent of biopsy cores positive for cancer is a predictor of advanced pathological stage and poor clinical outcomes in patients treated with radical prostatectomy. J Urol. 2004; 171: 2209-14.
- Ward JF, Blute ML, Slezak J, Bergstralh EJ, Zincke H: The long-term clinical impact of biochemical recurrence of prostate cancer 5 or more years after radical prostatectomy. J Urol. 2003; 170: 1872-6.
- Schroder FH, Hermanek P, Denis L, Fair WR, Gospodarowicz MK, Pavone-Macaluso M. The TNM classification of prostate cancer. Prostate Suppl. 1992; 4: 129-38.
- Gleason DF: Histologic Grading and Staging of Prostatic Carcinoma. In: Tannenbaum M (ed.): Urologic Pathology. Philadelphia, Lea & Feibeger. 1977; pp. 171-87.
- Freedland SJ, Csathy GS, Dorey F, Aronson WJ: Percent prostate needle biopsy tissue with cancer is more predictive of biochemical failure or adverse pathology after radical prostatectomy than prostate specific antigen or Gleason scores. J Urol. 2002; 167: 516-20.
- Leite KR, Srougi M, Bevilacqua RG, Dall’Oglio M, Andreoni C, Kauffmann JR, et al.: Quantification of tumor extension in prostate biopsies: importance in the identification of confined tumors. Int Braz J Urol. 2003; 29: 497-501.
- Linson PW, Lee AK, Doytchinova T, Chen MH, Weinstein MH, Richie JP, et al.: Percentage of core lengths involved with prostate cancer: does it add to the percentage of positive prostate biopsies in predicting postoperative prostate-specific antigen outcome for men with intermediate-risk prostate cancer? Urology. 2002; 59: 704-8.
- Sebo TJ, Bock BJ, Cheville JC, Lohse C, Wollan P, Zincke H: The percent of cores positive for cancer in prostate needle biopsy specimens is strongly predictive of tumor stage and volume at radical prostatectomy. J Urol. 2000; 163: 174-8.
__________________________
Received:
September 17, 2004
Accepted after revision: January 20, 2005
_______________________
Correspondence address:
Dr. Marcos F. Dall’Oglio
Rua Barata Ribeiro, 398 / 5o.
São Paulo, SP, 01308-000, Brazil
Fax: + 55 11 3159-3618
E-mail: marcosdallogliouro@terra.com.br