LAPAROSCOPIC
UPPER-POLE NEPHROURETERECTOMY IN INFANTS
(
Download pdf )
MARCIO L. MIRANDA, ANTONIO G. OLIVEIRA-FILHO, PATRICIA T. CARVALHO, ELAINE UNGERSBOCK, HUGO OLIMPIO, JOAQUIM M. BUSTORFF-SILVA
Division of Genitourinary Surgery, Pediatric Surgery Unit, State University of Campinas, Unicamp, Campinas, Sao Paulo, Brazil
ABSTRACT
Objective:
Report the results of laparoscopic upper-pole nephroureterectomy in infants.
Materials and Methods: Six consecutive infants
underwent 7 laparoscopic upper-pole nephroureterectomy. Pre and postoperative
evaluation included renal sonography, voiding cystourethrogram and renal
scintigraphy. All infants showed upper-pole exclusion. Surgery was performed
through a transperitoneal approach with full flank position in all infants.
Three or 4 ports were used according to the necessity of retracting the
liver. The distal ureter was ligated close to the bladder whenever reflux
was present and the dysplastic upper-pole was divided with the help of
an electrocautery. Data regarding operative time, postoperative use of
analgesics, time to resume oral feeding, hospital stay and tubular function
were collected and analyzed.
Results: All procedures were concluded as
planned. Mean operative time was 135 min. One patient underwent staged
bilateral upper-pole nephrectomy. There were no complications and the
postoperative hospital stay was 48 hours in 5 procedures and 24 hours
in 2 procedures. Pain medication was required only in the first day. Renal
tubular function showed improvement in half of the cases.
Conclusion: Laparoscopic partial nephrectomy
is a safe and feasible procedure in infants. Due to the magnification
provided by the lenses, a better vision of the structures is achieved,
facilitating selective dissection of vascular upper-pole, renal parenchyma
and distal ureter. This approach is less damaging to the lower pole, and
is associated to low morbidity and a short hospital stay.
Key
words: laparoscopy; infants; nephrectomy
Int Braz J Urol. 2007; 33: 87-93
INTRODUCTION
In pediatric practice, the use of minimally invasive surgery is on the rise due to its innumerous advantages over open surgery (1-3). Nephrectomy, which was one of the first laparoscopic procedures performed in children, has gained significant acceptance, especially due to the minimal morbidity, shorter hospital stay and improved cosmesis (1,2,4,5). Since the first report by Jordan and Winslow in 1993, the laparoscopic approach has become the procedure of choice for heminephrectomy (6,7). The retroperitoneal approach was proposed by GILL et al. in 1994 (8), but its use was restricted in infants due to the high incidence of peritoneal perforation (9). The purpose of this study is to report the results of a consecutive series of laparoscopic upper-pole nephroureterectomy procedures, with special emphasis in the function of the remaining kidney.
MATERIALS AND METHODS
Seven
upper-pole nephroureterectomies were performed in six infants between
January 2002 and January 2005. Clinical data were obtained by chart review.
Age at operation ranged from 5 to 20 months (median: 9.5 months). In the
case of a boy with bilateral duplex system, a second procedure was done
5 months after the first surgery. All infants (except one with recurrent
urinary tract infection) had a prenatal diagnosis of pyeloureteral duplex
system. This diagnosis was confirmed by ultrasonography, voiding cystourethrogram
and scintigraphy after birth. The 99mTc-DMSA scintigraphy revealed
duplicity of the renal unit with upper pole exclusion in all cases. Cystogram
showed ureterocele in 1 case and one child had vesicoureteral reflux in
both units.
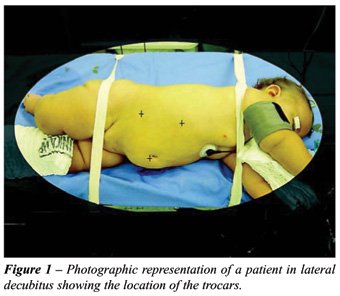
The procedure was done as described by Desgrandchamps
et al. 1999 (10). The transperitoneal approach was achieved with the patient
in the lateral decubitus position with the operative side up and the lumbar
region slightly flexed (Figure-1). The peritoneum was insufflated with
CO2 (pressure 12 mmHg). Three trocars were introduced (two 5 mm and one
10 mm). A fourth trocar (2 mm) was used in case a liver retraction was
needed (3 cases). After incising along the Toldt’s line, the colon
was retracted medially and the Gerota fascia was opened. Careful dissection
of the ureter of the upper pole avoiding mobilization of ureter of the
lower unit was done followed by the transposition of the duplicate ureter
over the renal vascular pedicle. The vascular supply of the upper-pole
was dissected and ligated with clips and the dysplastic parenchyma was
transected with electrocautery, avoiding damage to the lower half of the
kidney and to its vascular pedicle. No attempt was made to suture the
renal capsule over the open parenchymal surface. Finally, distal ureter
was either clipped close to the bladder if reflux was present, or emptied
and left opened whenever an ureterocele was present. The retroperitoneal
space was sutured and the incisions were infiltrated with bupivacain.
The operative time, need for analgesics, time to resume oral feeding and
length of hospital stay were assessed. Scintigraphic study to access the
tubular function was done usually six months after the surgery.
RESULTS
All
the procedures were completed laparoscopically with a mean operative time
of 135 minutes (range: 120 to 160 minutes). The estimated blood loss was
minimal and no major per-operative complications were observed. Five infants
were fed 4 hours after returning to their beds and the remaining in the
day following the surgery. The length of hospital stay was 48 hours for
5 infants and 24 hours for the other 2. Pain medication was required only
in the first postoperative day. The histopathological results indicated
the presence of renal dysplasia in 3 specimens and chronic pyelonephritis
in 4.
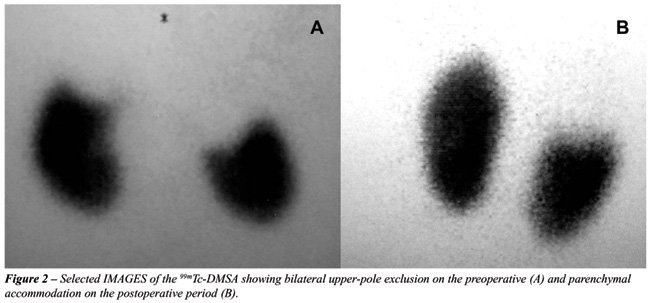
Mean follow-up was 18 months. 99mTc-DMSA
scintigraphy showed an improvement or maintenance of tubular function
in all infants (Figure-2).
COMMENTS
Because
the clinical diagnosis of duplex kidney is presumptive and renal dysplasia
of the upper pole may remain asymptomatic, prenatal or incidental sonographic
findings have contributed to early diagnosis (11). In this series, 6 out
of 7 infants had suspected prenatal diagnosis of duplex system and were
therefore referred early to the specialist.
Several surgical approaches to nephrectomy
of the upper pole have been described. The classic dorsal lumbotomy approach
ensures a great exposure but requires a large incision, intense renal
mobilization and is associated to the possibility of atrophy of the remaining
kidney (1,5,12). Jednak et al. (2000) described a rapid, safe and easy
technique of open heminephrectomy through supracostal approach, which
however had to incise parietal muscles and diaphragm to gain greater exposure
(13). With the advances and development of appropriated instruments for
children, improvement of the techniques with resulting lower rates of
morbidity, minimally invasive surgery is becoming common in the pediatric
surgery (1,3). An important contribution of video surgery in partial nephrectomy
is that the perfect view of the pedicle of both units and delimitation
after vascular clamping allows orderly sectioning of the parenchyma, avoiding
damage to the intact remaining unit (5,12). Some authors recommend the
use of a harmonic scalpel or argon beam coagulator to resect the parenchyma;
however, when the vascular delimitation is clear, this section does not
represent a problem (1,12). There is still some controversy regarding
the choice of either the transperitoneal or retroperitoneal approach.
Supporters of the retroperitoneal approach believe that it provides exposure
of the posterior aspect of the kidney units, avoiding dissection of the
kidney pedicle, which can be preserved (5,14). This approach may be posterior
or lateral. Borzi et al. have compared these two approaches and concluded
that the posterior approach is preferable for nephrectomies that do not
need ureterectomy (9). The lateral approach, on the other hand, provides
better access for complete resection of the ureter.
The main inconvenience of the retroperitoneal
access is the higher incidence of peritoneal tears in infants, which prevent
the creation of an adequate retropneumoperitoneum. This is the most common
complication and also the main cause of conversion to open surgery (9,12).
In some cases, peritoneal microperforations and consequent ventilatory
changes may occur. On the contrary, besides avoiding theses complications,
the transperitoneal approach also offers an excellent approach to the
vascular bundle with minimum lower pole mobilization and minimal morbidity
when compared to retroperitoneal approach (2). Nevertheless, there is
no conclusive medical evidence that favors either the retro or transperitoneal
approach (3,15). Like others, we also use the retroperitoneal approach
for children over two years of age or to perform a total nephrectomy (14).
The subjectivity of evaluating postoperative
pain in children, made analysis of the data very difficult. Reduction
of postoperative pain is apparent but very hard to prove in many controlled
series (2).
Assessment of the postoperative tubular
function has not been stressed in the literature, most probably due to
the low incidence of the lesions in the remaining unit. Scintigraphic
evaluation is more qualitative than quantitative. In this series, half
of the cases presenting with preoperative ureterohydronephrosis and compression
of the lower pole, showed recover on postoperative scintigraphy. This
observation is probably due to parenchymal accommodation and not to an
actual improvement of tubular function. The 99mTc-DMSA analysis
of the tubular function was considered adequate for postoperative evaluation
since it demonstrated improved uptake of some renal units, justifying
the use of video assisted renal surgery in our service.
Most authors did not observe any difference
regarding the surgical duration of laparoscopic heminephrectomy and conventional
surgery (5,16). The increase in operative time reported by some is probably
related to the learning curve (3,12,16).
CONCLUSION
Minimally invasive approach should be considered when partial nephroureterectomy is indicated, whether through a transperitoneal or a retroperitoneal approach. Magnification makes selective upper-pole dissection safe and feasible, promotes sectioning of the distal ureter without additional incisions, minimizes surgical trauma in the lower pole with minimal morbidity, improving cosmetic results and reducing hospital stay.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Peters CA: Laparoscopic and robotic approach to genitourinary anomalies in children. Urol Clin North Am. 2004; 31: 595-605.
- Robinson BC, Snow BW, Cartwright PC, De Vries CR, Hamilton BD, Anderson JB: Comparison of laparoscopic versus open partial nephrectomy in a pediatric series. J Urol. 2003; 169: 638-40.
- Steyaert H, Valla JS: Minimally invasive urologic surgery in children: an overview of what can be done. Eur J Pediatr Surg. 2005; 15: 307-13.
- Koyle MA, Woo HH, Kavoussi LR: Laparoscopic nephrectomy in the first year of life. J Pediatr Surg. 1993; 28: 693-5.
- Valla JS, Breaud J, Carfagna L, Tursini S, Steyaert H: Treatment of ureterocele on duplex ureter: upper pole nephrectomy by retroperitoneoscopy in children based on a series of 24 cases. Eur Urol. 2003; 43: 426-9.
- Jordan GH, Winslow BH: Laparoendoscopic upper pole partial nephrectomy with ureterectomy. J Urol. 1993; 150: 940-3.
- Horowitz M, Shah SM, Ferzli G, Syad PI, Glassberg KI: Laparoscopic partial upper pole nephrectomy in infants and children. BJU Int. 2001; 87: 514-6.
- Gill IS, Delworth MG, Munch LC: Laparoscopic retroperitoneal partial nephrectomy. J Urol. 1994; 152: 1539-42.
- Borzi PA: A comparison of the lateral and posterior retroperitoneoscopic approach for complete and partial nephroureterectomy in children. BJU Int. 2001; 87: 517-20.
- Desgrandchamps F, Gossot D, Jabbour ME, Meria P, Teillac P, Le Duc A: A 3 trocar technique for transperitoneal laparoscopic nephrectomy. J Urol. 1999; 161: 1530-2.
- Hulbert WC, Rabinowitz R: Prenatal diagnosis of duplex system hydronephrosis: effect on renal salvage. Urology. 1998; 51: 23-6.
- El-Ghoneimi A, Farhat W, Bolduc S, Bagli D, McLorie G, Khoury A: Retroperitoneal laparoscopic vs open partial nephroureterectomy in children. BJU Int. 2003; 91: 532-5.
- Jednak R, Kryger JV, Barthold JS, Gonzalez R: A simplified technique of upper pole heminephrectomy for duplex kidney. J Urol. 2000; 164: 1326-8.
- Borzi PA, Yeung CK: Selective approach for transperitoneal and extraperitoneal endoscopic nephrectomy in children. J Urol. 2004; 171: 814-6.
- Guillonneau B, Ballanger P, Lugagne PM, Valla JS, Vallancien G: Laparoscopic versus lumboscopic nephrectomy. Eur Urol. 1996; 29: 288-91.
- Janetschek G, Seibold J, Radmayr C, Bartsch G: Laparoscopic heminephroureterectomy in pediatric patients. J Urol. 1997; 158: 1928-30.
____________________
Accepted
after revision:
June 31, 2006
_______________________
Correspondence address:
Dr. Marcio Lopes Miranda
R. Timburí 945
Campinas, SP, 13098-301, Brazil
E-mail: marciomiranda@terra.com.br
EDITORIAL COMMENT
The
authors performed upper pole nephrectomy by laparoscopy in children under
two years old and achieved good results. The authors are to be congratulated
for their efforts in light of the fact that few articles have been published
on this subject. However, I would like to comment on some of the thoughts
and conclusions made by the authors. First, despite its common usage,
the term “minimally invasive procedure” is not an accurate
manner to address the laparoscopic upper pole nephrectomy because except
for skin incision all the following steps are the same as the open surgery.
Because the laparoscopic surgery was performed intraperitonially, one
could actually consider it as more invasive, since the peritoneum is not
entered in the open procedure. Also, a 10 mm trocar is not a small instrument
for such a small child. I believe laparoscopic upper pole nephrectomy
is the procedure of choice in older children and has been performed on
our group at this age. Moreover, I do not agree with the authors’
statement that in small children a large incision is needed for open surgery.
The benefits of improved cosmesis and rapid recovery remain controversial
in younger children and infants, where smaller incisions and quicker recovery
tend to be the role in most open procedures (1). In our department we
perform in very young children, the technique described by Jednak et al.
and do not isolate the vascular pedicle, which minimizes the risk of vascular
damage, and lower pole ischemia (2,3). This procedure is fast, the patients
are discharged in 24 hours and there is no need for excessive pain medication
at this age.
The
authors commented that 5 children were discharged within 48 hours and
that pain medication was only necessary for 24 hours in all patients.
This raises the question, what were these 5 infants doing at the hospital
for 24 hours longer if there was no more pain?
The
authors reported that there was improvement in renal function on the operated
side. However, this is not possible since according to the authors, there
was no upper pole function before the operation and all upper pole tissue
was removed. There was no comment about the extent of this improvement,
but certainly this cannot be attributed to a better technique. A maximum
of 5% difference among two renal DMSA scans would be expected and this
is just an artifact and therefore I do not think that renal accommodation
is a good explanation.
Furthermore
because there is no control group, the authors cannot justify any advantage
of upper pole laparoscopy over open surgery. Prospective studies comparing
different surgical approaches are warranted.
REFERENCES
- Wallis MC, Khoury AE, Lorenzo AJ, Pippi-Salle JL, Bagli DJ, Farhat WA: Outcome analysis of retroperitoneal laparoscopic heminephrectomy in children. J Urol. 2006; 175: 2277-82.
- Jednak R, Kryger JV, Barthold JS, Gonzalez R: A simplified technique of upper pole heminephrectomy for duplex kidney. J Urol. 2000; 164: 1326-8.
- Barroso U Jr, Vinhaes AJ, Barros MS, Calado AA, Macedo A Jr, Srougi M: Simplified upper pole nephrectomy: initial experience. Int Braz J Urol. 2005; 31: 157-60.
Dr. Ubirajara Barroso Jr.
Section of Urology
Federal University of Bahia
Salvador, Bahia
E-mail: ubarroso@uol.com.br
EDITORIAL COMMENT
Partial
nephrectomy is an uncommon procedure in children. This study, therefore,
is a welcome opportunity to re-visit this problem. Indeed antenatal diagnosis
has uncovered many urologic anomalies, including ureteral duplications,
which are asymptomatic (6 cases in this series). Nevertheless, spontaneous
resolution seems unlikely for most ectopic ureters and ureteroceles (1).
So as in this series, in case of duplex system with minimal or non-functioning
upper pole, heminephrectomy is recommended for the affected upper pole
(2). A subtotal ureterectomy is usually sufficient, certainly when there
is no associated ureterocele. Once that established rest the type of approach.
The
gold standard approach still uses a classical flank incision. One of the
main problems of this type of operation is that it requires a complete
mobilization of the kidney and the vessels. However, vessels of babies
are prone to spasm. Failure of excretion of the lower pole therefore is
the main postoperative complication. Minimal invasive surgery will probably
decrease this complication due to better vision of the vessels (magnification)
and the fact that heminephrectomy will be done “in situ”.
The minimal invasive approach however may be transperitoneal or retroperitoneal
(3). The transperitoneal approach, as described in authors’ paper,
provides a wider exposition but requires colon mobilization and unnecessary
opening of the peritoneum. Complications are described (4). Patient’s
position may be lateral as in this series or more frequently supine with
a tilted table. The retroperitoneal access is more “natural”,
faster in experienced hands, but requires creation of a working space.
This way undoubtedly gives the best hilum’s exposition. Conversion
rate is higher, in part due to the learning curve and a thin peritoneum
in babies (3 and authors).
Postoperative
assessment of tubular function is a finding of importance in this paper.
The authors should be encouraged to report longer term-follow up and perhaps
to design a study in collaboration with their scintigraphists and nephrologists
in order to better understand this phenomenon.
REFERENCES
- Keating MA: Ureteral Duplication Anomalies: Ectopic Ureters and Ureteroceles. In: Docimo SG (ed.), Clinical Pediatric Urology. United Kingdom, Informa Healthcare. 2007, fifth edition, 593-648.
- Smith EL, Ritchie EL, Maizels M, Zaontz MR, Hsueh W, Kaplan WE, et al.: Surgery for duplex kidneys with ectopic ureters: ipsilateral ureteroureterostomy versus polar nephrectomy. J Urol. 1989; 142: 532-534.
- Lais A, Peters CA: Laparoscopic Management of Duplication Anomalies. In: Docimo SG (ed.), Clinical Pediatric Urology. United Kingdom, Informa Healthcare. 2007, fifth edition, 649-54.
- Parsons JK, Varkarakis I, Rha KH, Jarrett TW, Pinto PA, Kavoussi LR: Complications of abdominal urologic laparoscopy: longitudinal five-year analysis. Urology. 2004, 63: 27-32.
Dr. Henri Steyaert
Pediatric Surgery and Urology
Lenval Foundation for Children
Nice, France
E-mail: henri.steyaert@lenval.com