LAPAROSCOPIC
SURGERY FOR RENAL STONES: IS IT INDICATED IN THE MODERN ENDOUROLOGY ERA?
(
Download pdf )
ANDREI NADU, OSCAR SCHATLOFF, ROY MORAG, JACOB RAMON, HARRY WINKLER
Department of Urology, The Chaim Sheba Medical Center, Tel Hashomer, Israel and The Sackler School of Medicine, Tel Aviv University, Israel
ABSTRACT
Purpose:
To report the outcomes of laparoscopic surgery combined with endourological
assistance for the treatment of renal stones in patients with associated
anomalies of the urinary tract. To discuss the role of laparoscopy in
kidney stone disease.
Materials and Methods: Thirteen patients
with renal stones and concomitant urinary anomalies underwent laparoscopic
stone surgery combined with ancillary endourological assistance as needed.
Their data were analyzed retrospectively including stone burden, associated
malformations, perioperative complications and outcomes.
Results: Encountered anomalies included
ureteropelvic junction obstruction, horseshoe kidney, ectopic pelvic kidney,
fussed-crossed ectopic kidney, and double collecting system. Treatment
included laparoscopic pyeloplasty, pyelolithotomy, and nephrolithotomy
combined with flexible nephroscopy and stone retrieval. Intraoperative
complications were lost stones in the abdomen diagnosed in two patients
during follow up. Mean number of stones removed was 12 (range 3 to 214).
Stone free status was 77% (10/13) and 100% after one ancillary treatment
in the remaining patients. One patient had a postoperative urinary leak
managed conservatively. Laparoscopic pyeloplasty was successful in all
patients according to clinical and dynamic renal scan parameters.
Conclusions: In carefully selected patients,
laparoscopic and endourological techniques can be successfully combined
in a one procedure solution that deals with complex stone disease and
repairs underlying urinary anomalies.
Key
words: kidney; laparoscopy; nephrolithiasis; genitourinary abnormalities
Int Braz J Urol. 2009; 35: 9-18
INTRODUCTION
Endourological
techniques have revolutionized the treatment of urinary stones to the
point they have rendered open stone surgery anachronistic (1). Procedures
like open ureterolithotomy, open nephrolithotomy, or open pyelolithotomy
have become anecdotal. However, patients with large stone burdens and
associated renal malformations are prone to require multiple endourological
procedures in order to have their stones retrieved and anomalies repaired.
Thus in these selected patients, open stone surgery can certainly be considered
reasonable (2). In centers with established experience in advanced reconstructive
laparoscopy, this can be a feasible option if the goals of stone clearance
and correction of malformations could be achieved in a single procedure.
Incorporating laparoscopic techniques confer these patients surgical efficacy
combined with the advantages of minimally invasive surgery.
In the present paper, we describe our experience
and evaluate the outcomes of laparoscopic surgery in combination with
endourological procedures involving a variety of cases of renal stones
in the setting of underlying urinary tract malformations.
MATERIALS AND METHODS
The
data of twenty-nine patients who underwent laparoscopic procedures for
kidney stones between January 2004 and May 2007 were retrospectively analyzed.
Retrieved data included indications for intervention, stone burden, associated
malformations, perioperative complications and outcomes in terms of functional
results and stone free status. Fifteen patients underwent laparoscopic
nephrectomy due to non functioning kidneys and were not included in the
present study. One patient underwent laparoscopic pyelolithotomy without
harboring underlying malformations and thus was also excluded. The remaining
thirteen patients underwent laparoscopic stone removal and reconstructive
procedures combined with ancillary endourological assistance as needed.
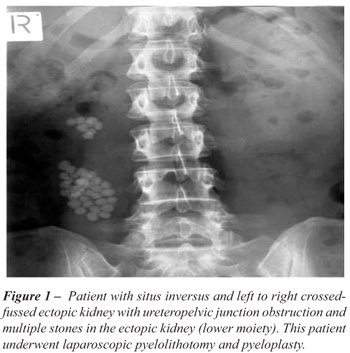
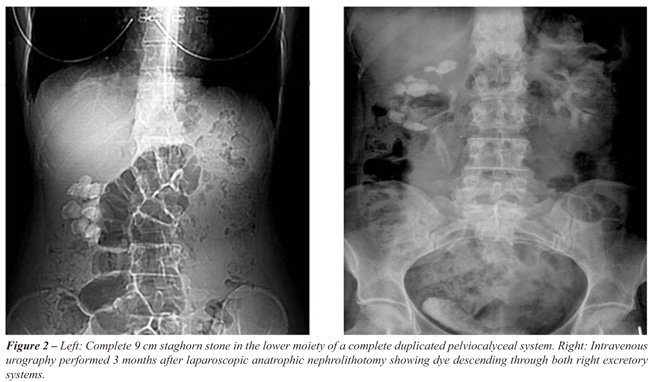
Preoperative stone scenario and associated anomalies are detailed in Table-1
and Figures-1 to 3. All cases were discussed with the endourology unit
and considered unlikely that stones and underlying anomalies could be
efficiently addressed with a single endourological procedure. Three patients
had previous unsuccessful endourological procedures, with inability to
gain percutaneous access and significant residual stones after nephroscopy
among main causes of failure.

Patients underwent preoperative anatomical
and functional evaluation with non contrast CT scan and either intravenous
pyelography or diuretic renal scans in cases of suspected ureteropelvic
junction (UPJ) obstruction. Postoperative assessment consisted of x-rays,
ultrasound, and/or CT as appropriate. A diuretic renal scan was performed
in patients who underwent concomitant pyeloplasty.
Surgical procedures and their technique
are summarized below. Combinations were used to deal with specific patient
necessities.
SURGICAL TECHNIQUE
Laparoscopic
Pyeloplasty and Pyelolithotomy / Flexible Nephroscopy
The operative room setting includes one
laparoscopic cart and one endourological cart to enable simultaneous laparoscopy
and nephroscopy. Using a four port transperitoneal approach, the ureter
is identified and followed cranially, the UPJ is exposed and the renal
pelvis dissected. The renal pelvis is opened above the UPJ, the ureter
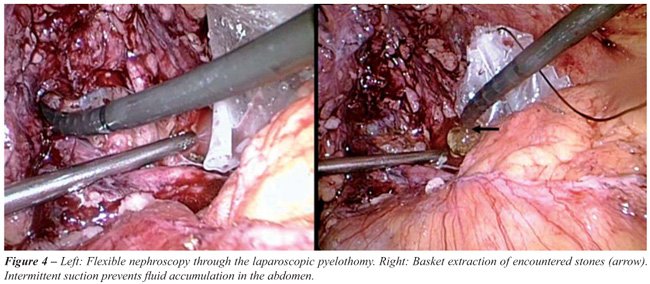
is spatulated on its lateral aspect and dismembered. Stones in the renal
pelvis are removed with an atraumatic grasper and placed in a laparoscopic
bag. A flexible cysto-nephroscope is passed through one of the 10 mm ports
and guided laparoscopically through the opening in the renal pelvis. The
kidney is systematically inspected and calyceal stones removed with a
basket or fragmented with Holmium:YAG laser lithotripsy. A double J stent
is introduced in an antegrade fashion, the renal pelvis is reduced as
needed, and ureteropelvic anastomosis is performed with two (one posterior
and one anterior) 4/0 polyglactin running sutures. A percutaneous drain
is placed and the bag with stones removed (Figure-4).
Laparoscopic
Nephrolithotomy
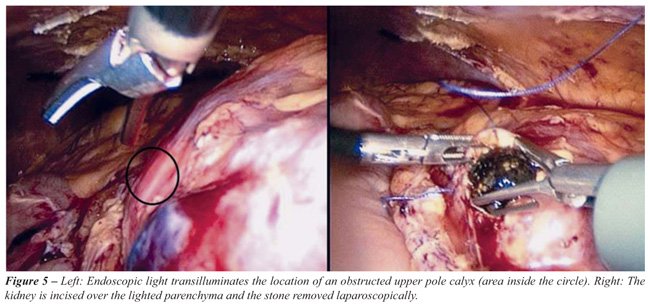
A “cut for the light” technique
was used when calyceal stones were associated with infundibular stricture,
obstructed hydrocalyx, or calyceal diverticulum. After widely incising
the renal pelvis, the flexible cysto-nephroscope is brought at the obstructed
calyx containing the stone and a small laparoscopic nephrotomy is made
in the kidney as indicated by the endoscopic light. The stone is removed
and the kidney sutured with one layer 2/0 polyglactin (Figure-5).
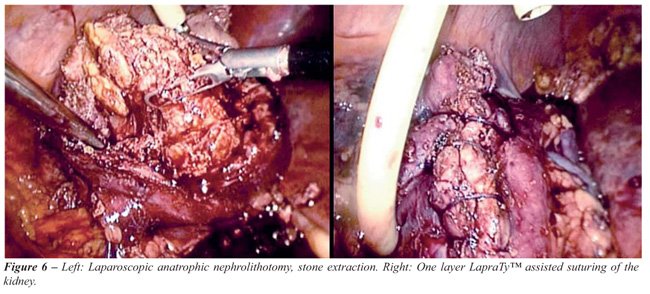
Laparoscopic
Anatrophic Nephrolithotomy
The kidney is dissected from the surrounding
fat, the vascular elements identified and clamped en bloc with a laparoscopic
Satinsky clamp. The renal parenchyma and collecting system are incised
longitudinally on the postero-lateral aspect of the kidney; the staghorn
stone is mobilized with graspers, removed and placed in an endobag. A
16 F Foley catheter is placed as a nephrostomy tube by making a small
incision in the kidney away from the nephrotomy line. The kidney is sutured
with a running 2/0 polyglactin single layer that includes renal capsule,
parenchyma, and collecting system in a “no-knot” technique
with the aid of Lapra-Ty clips (Ethicon-Johnsons & Johnsons), Figure-6.
RESULTS
Mean
age at surgery was 36 years (range 18-56), ASA score 2 (range 1-2), and
average number of stones removed was 12 (range 3 to 214). Laparoscopic
pyeloplasty combined with pyelolithotomy and flexible nephroscopy was
performed in ten patients, laparoscopic pyeloplasty with pyelolithotomy
and endoscopic-assisted nephrolithotomy was performed in two; and laparoscopic
anatrophic nephrolithotomy was performed in one patient (Table-2).
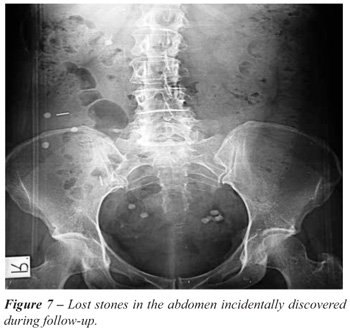
A double J stent and percutaneous drain
was left postoperatively in all patients. Additionally, a nephrostomy
drain using a 16 Fr Foley catheter was placed in two patients. All the
procedures were completed laparoscopically with no conversions to open
surgery. Intraoperative complications included two patients with lost
stones in the abdomen diagnosed during follow up (Figure-7) and variable
degrees of irrigation fluid accumulation secondary to nephroscopy in several
others. One patient had a postoperative urinary leak in the context of
an indwelling double J stent, which was not replaced at the time of surgery,
and most probably chronically obstructed. Leakage was discovered during
early postoperative period as urinary extravasation through the percutaneous
drain. Cystoscopic replacement of the double J stent effectively treated
the complication and the patient was discharged during the following days
without evidence of further leakage.
Stone free status was obtained in ten patients
(77%), and the remaining three were rendered stone free after one ancillary
procedure (shockwave lithotripsy - SWL) in two patients and retrograde
nephroscopy in another).
In all twelve patients with UPJ obstruction
the pyeloplasty was considered successful according to clinical (disappearance
of pain) and diuretic renal scan parameters. The mean washout half-life
time in the diuretic renal scan improved from 43 to 22 minutes.
Warm ischemia time for laparoscopic anatrophic
nephrolithotomy was 43 minutes; the patient was rendered stone free and
renal function remained within preoperative values.
COMMENTS
Endourology
has revolutionized the treatment of urinary stones. Notwithstanding, underlying
anatomic anomalies, extremely large stone burdens or a combination of
them can significantly decrease the success rate of endourological procedures
(3,4). The surgical approach in these special cases should efficiently
address the large stone burden and associated malformations in a single
procedure. Although open surgery is an alternative, laparoscopic surgery
might be a feasible option additionally conferring the advantages of minimally
invasive surgery.
Micali et al. reported 17 patients who underwent
laparoscopic stone extraction, including 11 with renal calculi and 9 with
associated anomalies (UPJ obstruction) with stone size up to 6 cm; fifteen
patients were eventually rendered stone free and one patient had a postoperative
urinoma. These authors concluded that indications for laparoscopy included
stones associated with anatomical abnormalities requiring reconstruction
and calculi for which endourological procedures had failed (5). Ramakumar
et al. reported 90% three month stone-free rate in 19 patients who underwent
laparoscopic pyelolithotomy and pyeloplasty (6). Similar results were
recently reported by Srivastava et al. (7) and Stein et al. (8) with 75
and 80% stone-free rates respectively.
Nambirajan et al. reported their experience
with eighteen patients who underwent different laparoscopic procedures
with concomitant stone removal, including pyeloplasties, partial nephrectomies,
and calyceal ablations. Stone-free status was achieved in 93% of cases.
The authors concluded that laparoscopy is effective for complex renal
stones and that the need for open surgery should be rare in the future
(9). Meria et al. compared laparoscopic pyelolithotomy to percutaneous
nephrolithotomy (PNL) in 32 patients with pelvic stones without underlying
malformations. Stone free rates were not significantly different (88 vs.
82%). However, the laparoscopic group had higher operative time, urological
complications (12% urine leak), and conversion to open surgery was required
in two patients. They concluded that indications for each technique must
be determined although PNL remains the gold standard for large pelvic
stones (10). It is our belief and current practice that SWL, retrograde
and percutaneous techniques are the first approaches to treat kidney stones
due to their excellent results and minimal morbidity. The role of laparoscopy
is not to replace any of these options, but to compliment them in situations
where decreased success or increased morbidity is expected, specially
as regards large stone burdens coexisting with underlying malformations.
As showed in our series and as reported by other authors (11,12), laparoscopic
and endourological techniques can be successfully combined in the same
procedure to improve the stone free rate and simultaneously resolve synchronous
anomalies.
Tunc et al. published a study on 150 patients
with stones in anomalous kidneys treated with SWL, including 57 duplex,
45 horseshoes, 30 malrotated, 14 pelvic, and 4 crossed ectopic. The overall
stone-free rate was 68%, with the worst results obtained in crossed ectopic
kidneys with stone clearance of only 25% (13). Pure percutaneous approach
has also been reported in anomalous kidneys. Although highly effective
with an overall stone-free rate of 83%, the anterior displacement of the
collecting system together with an unpredictable vascular supply and interposition
of bowel between the kidney and the abdominal wall makes the procedure
technically demanding. Moreover, it requires a highly precise imaging
system (i.e. CT guided) to minimize risk of visceral damage during kidney
puncture and tract creation (14). Pure endoscopic management has also
been accomplished for anomalous kidneys. Weizer et al. reported a 75%
stone-free rate (15), meanwhile Braz et al. reported an 81% stone-free
rate at three months, however 62% required ancillary treatments (16).
Due to urinary stasis, these patients suffer from poor spontaneous stone
passage, with persistence or growth of residual fragments in 60% of cases.
Laparoscopic techniques seem especially
useful for stones located in anomalous kidneys. Our overall stone-free
rate was 77% (10/13), and reached a 100% after one ancillary treatment
(i.e. SWL or nephroscopy). Additionally, anomalies to be addressed (i.e.
UPJ obstruction) were successfully repaired with optimal functional outcome.
There are several operative pitfalls that
need special consideration when combining laparoscopy with endourological
procedures. The operating room and the space around the operating table
become limited when the laparoscopic and endourological towers need to
be brought to work simultaneously. The laser cart and endourological instrumentation
table pose additional ergonomic problems. One serious limitation is the
difficulty to obtain fluoroscopic images during stone removal. Introduction
of a C arm becomes a challenge in the described set-up and even if possible
the images obtained in the insufflated abdomen of a patient in lateral
decubitus are far from informative. Deflating the abdomen may improve
the imaging but is unpractical and time consuming, and even after this,
images are of poor quality due to patient position and free fluid in the
abdomen, thus seriously limiting the ability to identify small residual
stones.
Irrigating fluid that flows freely into
the abdomen during the nephroscopy is of some concern and might be a limiting
factor. Although some of it can be suctioned, still large quantities of
fluid accumulate and occupy the space of the pneumoperitoneum. As fluid
accumulates between bowel loops it cannot be directly aspirated. We overcame
this difficulty by placing the patient in a “head down” position
for two minutes, allowing the fluid to accumulate under the diaphragm
where it becomes easily aspirated with the laparoscopic suction.
Identifying stones inside obstructed calyces
can become a real challenge. Intraoperative ultrasound can be useful in
these situations (9) however; it poses additional restrictions to the
already cumbersome operative scenario. We found a solution relying on
“cut for the light” technique, where the light of the endoscope
marks the stone containing calyx and the location for the parenchymal
incision. In the two cases performed, the light of the endoscope precisely
delineated the place for the nephrotomy (Figure-5).
Kaouk et al. created a porcine model to
address the feasibility of laparoscopic anatrophic nephrolithotomy (17),
Deger et al. reported the first case in humans (18), and recently Simforoosh
et al. (19) reported their series of five patients, with 3/5 being rendered
stone-free. Interestingly, no postoperative urinary extravasation occurred
albeit no internal stent was placed. We performed a laparoscopic anatrophic
nephrolithotomy in a young patient with a duplex system and a complete
staghorn of the lower moiety with optimal results and no perioperative
complications. The kidney was repaired with one running suture including
parenchyma and collecting system with no postoperative urinary extravasation.
An interesting aspect of laparoscopic pyelolithotomy
concerns stones lost in the abdomen. It is not infrequent during retrieval
of multiple small stones to have them fall out of the renal pelvis or
the endobag, and locating them in the abdomen is challenging and time
consuming. There is no report in the urological literature regarding this
issue; however there are well described complications of lost stones in
the abdomen after laparoscopic cholecystectomy. They include intraperitoneal
and abdominal wall abscess, fistula, and prolonged fever (20). Regarding
the infectious status of struvite staghorn stones, lost stones should
remain of concern. However, two patients in our series had lost stones
in the abdomen and after completing more than two years of follow-up,
they remain completely asymptomatic.
We are aware of the limitations of this
paper, which consist of a small, retrospective series of patients. However,
considering the limited data published up to date we believe our experience
contributes to the developing of this novel and poorly studied approach.
CONCLUSIONS
Although classical endourological procedures should remain as the gold standard for the great majority of renal stones, however patients with large stone burdens and underlying malformations might benefit from a combined laparoscopic and endourological one procedure solution that deals with complex stone disease and repairs associated anomalies.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Matlaga BR, Assimos DG: Changing indications of open stone surgery. Urology. 2002; 59: 490-3; discussion 493-4.
- Alivizatos G, Skolarikos A: Is there still a role for open surgery in the management of renal stones? Curr Opin Urol. 2006; 16: 106-11.
- Grasso M, Conlin M, Bagley D: Retrograde ureteropyeloscopic treatment of 2 cm. or greater upper urinary tract and minor Staghorn calculi. J Urol. 1998; 160: 346-51.
- Semerci B, Verit A, Nazli O, Ilbey O, Ozyurt C, Cikili N: The role of ESWL in the treatment of calculi with anomalous kidneys. Eur Urol. 1997; 31: 302-4.
- Micali S, Moore RG, Averch TD, Adams JB, Kavoussi LR: The role of laparoscopy in the treatment of renal and ureteral calculi. J Urol. 1997; 157: 463-6.
- Ramakumar S, Lancini V, Chan DY, Parsons JK, Kavoussi LR, Jarrett TW: Laparoscopic pyeloplasty with concomitant pyelolithotomy. J Urol. 2002; 167: 1378-80.
- Srivastava A, Singh P, Gupta M, Ansari MS, Mandhani A, Kapoor R, et al.: Laparoscopic pyeloplasty with concomitant pyelolithotomy--is it an effective mode of treatment? Urol Int. 2008; 80: 306-9.
- Stein RJ, Turna B, Nguyen MM, Aron M, Hafron JM, Gill IS, et al.: Laparoscopic pyeloplasty with concomitant pyelolithotomy: technique and outcomes. J Endourol. 2008; 22: 1251-5.
- Nambirajan T, Jeschke S, Albqami N, Abukora F, Leeb K, Janetschek G: Role of laparoscopy in management of renal stones: single-center experience and review of literature. J Endourol. 2005; 19: 353-9.
- Meria P, Milcent S, Desgrandchamps F, Mongiat-Artus P, Duclos JM, Teillac P: Management of pelvic stones larger than 20 mm: laparoscopic transperitoneal pyelolithotomy or percutaneous nephrolithotomy? Urol Int. 2005; 75: 322-6.
- Fariña Pérez LA, Cambronero Santos J, Meijide Rico F, Zungri Telo ER: Laparoscopic pyelolithotomy in a pelvic kidney. Actas Urol Esp. 2004; 28: 620-3.
- Whelan JP, Wiesenthal JD: Laparoscopic pyeloplasty with simultaneous pyelolithotomy using a flexible ureteroscope. Can J Urol. 2004; 11: 2207-9.
- Tunc L, Tokgoz H, Tan MO, Kupeli B, Karaoglan U, Bozkirli I: Stones in anomalous kidneys: results of treatment by shock wave lithotripsy in 150 patients. Int J Urol. 2004; 11: 831-6.
- Matlaga BR, Shah OD, Zagoria RJ, Dyer RB, Streem SB, Assimos DG: Computerized tomography guided access for percutaneous nephrostolithotomy. J Urol. 2003; 170: 45-7.
- Weizer AZ, Springhart WP, Ekeruo WO, Matlaga BR, Tan YH, Assimos DG, et al.: Ureteroscopic management of renal calculi in anomalous kidneys. Urology. 2005; 65: 265-9.
- Braz Y, Ramon J, Winkler H: Ureterorenoscopy and holmium laser lithotripsy for large renal stone burden: A reasonable alternative to percutaneous nephrolithotomy. Eur Urol. 2005; (Suppl 4): 264. (Abstract 1047).
- Kaouk JH, Gill IS, Desai MM, Banks KL, Raja SS, Skacel M, et al.: Laparoscopic anatrophic nephrolithotomy: feasibility study in a chronic porcine model. J Urol. 2003; 169: 691-6.
- Deger S, Tuellmann M, Schoenberger B, Winkelmann B, Peters R, Loening SA: Laparoscopic anatrophic nephrolithotomy. Scand J Urol Nephrol. 2004; 38: 263-5.
- Simforoosh N, Aminsharifi A, Tabibi A, Noor-Alizadeh A, Zand S, Radfar MH, et al.: Laparoscopic anatrophic nephrolithotomy for managing large staghorn calculi. BJU Int. 2008; 101: 1293-6.
- Memon MA, Deeik RK, Maffi TR, Fitzgibbons RJ Jr: The outcome of unretrieved gallstones in the peritoneal cavity during laparoscopic cholecystectomy. A prospective analysis. Surg Endosc. 1999; 13: 848-57.
____________________
Accepted after revision:
October 24, 2008
_______________________
Correspondence address:
Dr. Oscar Schatloff
Department of Urology
The Chaim Sheba Medical Center
Tel Hashomer, 52621, Israel
Fax: + 972 3 535-1892
E-mail: oscar.schatloff@gmail.com
EDITORIAL COMMENT
Authors
present interesting series of patients with urinary stone disease managed
mainly by laparoscopic method. The presented cases have some kind of anomaly
necessitating laparoscopic approach rather than using routine endourological
procedures like percutaneous nephrostolithotomy or urethroscopic means.
Laparoscopy is gaining more popularity in
managing urinary stone disease (1-3). This is especially true when associated
anomalies like ureteropelvic junction obstruction, or fusion anomalies
exists (4).
Even though results of laparoscopic approach
in managing stone disease in the present series and other reported series
seems satisfactory (1-5), longer follow-up and more cases are necessary
to better elucidate the exact role of laparoscopy in today’s management
of stone disease.
REFERENCES
- Simforoosh N, Aminsharifi A, Tabibi A, Noor-Alizadeh A, Zand S, Radfar MH, et al.: Laparoscopic anatrophic nephrolithotomy for managing large staghorn calculi. BJU Int. 2008; 101: 1293-6.
- Basiri A, Simforoosh N, Ziaee A, Shayaninasab H, Moghaddam SM, Zare S: Retrograde, antegrade and laparoscopic approaches for the management of large, proximal stones: A randomized clinical trial. J Endourol. 2008; 22: 2677-80.
- Meria P, Milcent S, Desgrandchamps F, Mongiat-Artus P, Duclos JM, Teillac P: Management of pelvic stones larger than 20 mm: laparoscopic transperitoneal pyelolithotomy or percutaneous nephrolithotomy? Urol Int. 2005; 75: 322-6.
- Mosavi-Bahar SH, Amirzargar MA, Rahnavardi M, Moghaddam SM, Babbolhavaeji H, Amirhasani S: Percutaneous nephrolithotomy in patients with kidney malformations. J Endourol. 2007; 21: 520-4.
- Simforoosh N, Basiri A, Danesh AK, Ziaee SA, Sharifiaghdas F, Tabibi A, et al.: Laparoscopic management of ureteral calculi: a report of 123 cases. Urol J. 2007; 4: 138-41.
Dr.
Nasser Simforoosh
Shaheed Labbafinejad Hospital
Urology Nephrology Research Center
Shaheed Beheshti University of Medical Sciences
Tehran, Iran
E-mail: simforoosh@iurtc.org.ir
EDITORIAL COMMENT
Laparoscopy
is an established modality in management of renal stones in selected situations.
On most occasions, laparoscopy is nephron sparing - namely - pyelolithotomy
as compared with percutaneous nephrostolithotomy (PCNL).
The authors have successfully used laparoscopy
combined with endourological procedures in anomalous kidneys, mainly ureteropelvic
junction obstruction. This is a retrospective study. Larger and prospective
studies will help in developing concrete guidelines.
It is to be noted that a renal angiogram
or CT angiogram is a complimentary investigation in planning reconstructive
laparoscopic surgery in anomalous kidneys.
The authors have not done an infundibuloplasty
in cases of infundibular stenosis with calyceal diverticulum and; the
collecting system was not closed separately in patients with staghorn
calculus where an anatrophic pyelolithotomy was done. It would be interesting
to see the configuration of the collecting system using a CT scan during
follow-up.
In most centers, pyeloplasty is done with
interrupted sutures. The authors have used running sutures for the anterior
and posterior walls.
Meria et al. had shown similar results with
different modalities (PCNL and laparoscopy) in management of stone disease
in non-anomalous kidneys; however the complication rate in was higher
in laparoscopy compared to ESWL and PCNL. Hence, they concluded that ESWL
or PCNL should be the first option in non-anomalous kidneys.
Practical problems of C arm usage; ultrasound
usage and free flow of irrigating fluid into the peritoneal cavity with
laparoscopy are problems to be looked into.
Combining laparoscopy with PCNL and pure
endoscopy gives a better result in stone disease.
Dr.
Manickam Ramalingam
Department of Urology
K.G. Hospital and Post Graduate Institute
Coimbatore, India
E-mail: uroram@yahoo.com