RE:
APPENDICEAL SUBSTITUTION FOLLOWING RIGHT PROXIMAL URETER INJURY
(
Download pdf )
To the Editor:
Use
of the appendix as a ureteral substitute was first described by Melnikoff
in 1912 (1). However, the technique has been used only in a handful of
patients since its introduction (2,3). We present the case of a 66 year-old
male who presented with abdominal pain three weeks after undergoing lysis
of small bowel adhesions, and was found to have an 8-10 cm defect of the
right proximal ureter upon undergoing retrograde pyelogram.
There are numerous techniques for the repair
of ureteral injuries. Primary end-to-end anastomosis, psoas hitch ureteral
reimplantation, and Boari flap were not feasible in this case due to the
length and location of the injury. Ileal interposition has been successfully
used to repair large defects, but requires a bowel anastomosis, which
we wished to avoid. Auto-transplantation of the kidney is technically
challenging and associated with unique morbidities. Appendiceal substitution
was chosen due to the amenable location of the injury and favorable operative
risks.
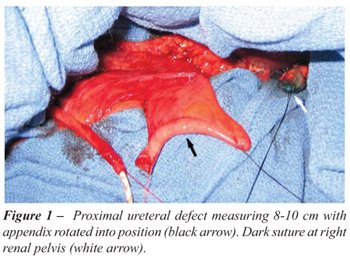
In the operating room, we injected methylene
blue through a previously placed nephrostomy tube in order to better delineate
the proximal margin of the injury. The appendix was then ligated at its
base and tip and detached from the cecum. Special attention was given
to preserving the appendicular arteries and mesoappendix (Figure-1). The
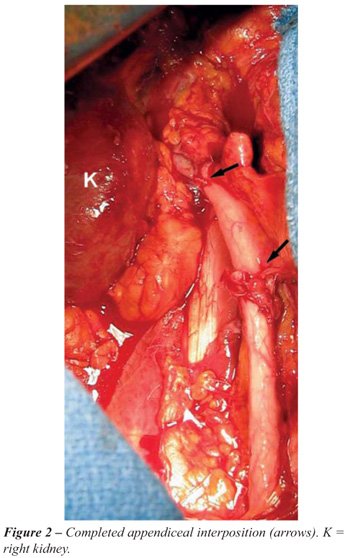
appendix was cannulated to accommodate a 14 French endopyelotomy stent.
Next, the appendix was rotated up to the level of the renal pelvis to
ensure a tension free anastomosis. It was then oriented in isoperistaltic
fashion with its distal tip abutting the renal pelvis. A spatulated uretero-appendiceal
anastomosis was performed on both ends of the graft (Figure-2). The
anastomosis was then tested for leakage by injecting methylene blue through
the indwelling nephrostomy tube.
The patient was discharged from the hospital
on postoperative day six and the stents were removed four weeks later.
Intravenous pyelogram at eight months postoperatively showed a patent
appendiceal graft with no evidence of stricture or hydronephrosis (Figure-3).

Long-term data in the small body of literature
devoted to this procedure demonstrates excellent autograft performance
and preserved renal function up to fifteen years postoperatively (2).
While traumatic injury is the most commonly reported indication for this
procedure, it has also been employed successfully in other settings such
as ureteral necrosis secondary to dermatomyositis. This technique has
also been proven effective in pediatric as well as adult populations (2).
The majority of case reports of appendiceal
interposition involve the right ureter due to the ipsilateral location
of the appendix. However, there is at least one description of a proximal
left ureteral repair by Zargar et al. 2004 (3). To accomplish the left-sided
reconstruction the author mobilized the appendix with the right colon
and distal ileum into the left ureteral fossa.
This case supports appendiceal substitution
as a reasonable option for patients with right-sided ureteral defects
not amenable to primary end-to-end anastomosis. Limiting factors for the
procedure include presence and length of appendix, impaired renal function,
and history of pelvic irradiation.
REFERENCES
- Melnikoff AE: Sur le replacement de l’uretere par anse isolée de l’intestin grêle. Rev Clin Urol. 1912; 1: 601-05.
- Richter F, Stock JA, Hanna MK: The appendix as right ureteral substitute in children. J Urol. 2000; 163: 1908-12.
- Zargar MA, Mirzazadeh M, Zargar K: The appendix, an acceptable substitute for all segments of both ureters: a report of two cases. Med J Islam Repub Iran. 2004; 18: 177-180.
Matt
S. Ashley, BA &
Dr. Siamak Daneshmand
Division of Urology & Renal Transplantation
Oregon Health & Science University
Portland, Oregon, USA
E-mail: daneshma@ohsu.edu