THE
EFFECT OF ALPHA-BLOCKER TREATMENT ON BLADDER HYPOXIA INDUCIBLE FACTOR-1
ALPHA REGULATION DURING LOWER URINARY TRACT OBSTRUCTION
(
Download pdf )
doi: 10.1590/S1677-55382010000100013
GEORGE KORITSIADIS, STAVROS I. TYRITZIS, GEORGE KOUTALELLIS, ANDREAS C. LAZARIS, KONSTANTINOS STRAVODIMOS
Department of Urology (GK, SIT, GK, KS) and Pathology (ACL), Athens University Medical School, LAIKO Hospital, Athens, Greece
ABSTRACT
Aims:
To determine whether a1-blocker treatment, in chronic bladder outlet obstruction
(BOO), influences bladder tissue ischemia.
Materials and Methods: This prospective
study included 60 patients with BOO, of which 40 were under α1-blocker
medication and 20 without treatment. Patients underwent transurethral
resection of the prostate (TURP) or suprapubic prostatectomy (SPP). Ten
patients with non-muscle invasive bladder cancer underwent transurethral
resection of the bladder tumor and served as the control group. Tissue
specimens were immunohistochemically stained for hypoxia inducible factor-1a
(HIF-1α).
Results: Bladder tissue from obstructed
subjects showed high immunoreactivity to HIF-1α. The specimens from the
control group, showed no or weak, mainly cytoplasmic immunoreactivity
to HIF-1α. Patients under α -blocker treatment did not differ in the number
of HIF-1α positive cells compared to subjects with no treatment (median
number 86.8 [20-150] and 88.6 [0-175], respectively) (p > 0.05). The
lowest bladder pressure at which HIF-1α was up regulated, was detected
at detrusor pressure Qmax (PdetQmax) = 60 cm H2O.
Conclusions: Treatment with α-blockers in
obstructed patients considered as non-responders, does not result in HIF-1α
down regulation, thus bladder continues to be under chronic stress.
Key
words: bladder; bladder outlet obstruction; hypoxia inducible
factor-1; ischemia; alpha-blockers
Int Braz J Urol. 2010; 36: 86-94
INTRODUCTION
First line
treatment in patients with bladder outlet obstruction (BOO) is alpha1-adrenoreceptor
antagonists (1). However, their contribution is limited mostly in alleviating
benign prostatic hyperplasia (BPH) symptoms rather than influencing disease
progression, which is manifested as acute urinary retention or the need
for invasive therapy (2).
There is evidence based on non-obstructed experimental models, that during
the emptying phase, bladder pressure increases while oxygen wall tension
decreases and returns to premicturition levels, shortly after voiding
is completed. In the obstructed animal model however, the pressure generated
is much higher and the bladder wall remains ischemic for several minutes
even after micturition has ended (3). In BOO, blood flow to the bladder
is inversely related to filling, leading to severe hypoxia and consequent
further damage to the detrusor (4).
Tissue hypoxia can be evaluated by measuring the levels of hypoxia inducible
factor-1α (HIF-1α). HIF-1α is a multipotent protein activated in cells
when they are under low oxygen tension, and functions as cellular regulator
of oxygen. Its multipotency is demonstrated by its crucial role in angiogenesis
through vascular endothelial growth factor (VEGF) up-regulation and the
regulation of cellular metabolism in diseases such as stroke, heart attack
and cancer, which generate a hypoxic microenvironment (5). The close association
of hypoxia and HIF-1α has been established in previous reports (6,7),
and this association provides the rationale of using this protein as a
credible hypoxia marker. Yet, there is evidence of HIF-1α induction by
non-hypoxic stimuli such as several growth factors, coagulation factors,
vasoactive peptides, cytokines, metal ions or even mechanical stress (8).
However, the pathway of their effect is based on reactive oxygen species
production, which somehow counterintuitive is up-regulated by hypoxia
(9,10). Thus, independently of the type of stimulus, it seems that hypoxia
is strongly related to HIF-1α synthesis.
To our knowledge, there are no reported studies on the effect of α1-blockers
in bladder metabolism and tissue hypoxia in patients with BOO and chronic
obstructed bladders, respectively. We made the hypothesis that since a1-blockers
used in BOO do not alleviate dramatically obstructive parameters, they
would not impact on bladder tissue hypoxia. The aim of the present study
was to examine tissue distribution of HIF-1a in patients with BOO under
α1-blocker medication, using urodynamic parameters and tissue immunohistochemical
staining.
MATERIALS AND METHODS
Patient Baseline Characteristics
This prospective,
non-blinded study took place from September 2004 to December 2006, including
60 patients with lower urinary tract symptoms (LUTS) suggestive of BOO
secondary to BPH (study group), who all provided informed consent. Ten
patients with non-muscle invasive bladder cancer scheduled for transurethral
resection (TUR-BT), without BOO or LUTS served as control group. Detrusor
tissue was retrieved from normal appearing urothelium distant from the
bladder cancer and the absence of cancer was verified microscopically.
Patients in the study group underwent detailed medical history, physical
examination and urinalysis with laboratory blood tests. LUTS were classified
according to International Prostate Symptom Score (IPSS). Maximum flow
rate (Qmax), post void residual volume (PVR), serum PSA and prostate volume
(Vpr) were determined. Indications for surgery were IPSS > 20, flow
rate less than 15 mL/sec and a history of acute urinary retention. In
the 20 patients with BOO without receiving treatment, we performed urodynamic
evaluation prior to surgery. The lowest detrusor pressure at max flow
(PdetQmax), maximum detrusor pressure (Pdetmax) and detrusor closure pressure
(PdetCL) were recorded.
The study group was further divided in those patients who were under tamsulosin
0.4 mg (40 patients) and those who were not (20 patients). The two subgroups
were well balanced regarding age, IPSS, Vpr and other comorbid conditions,
(diabetes, hypertension, smoking, high cholesterol). Exclusion criteria
in the study cohort comprised recurrent urinary tract infection, bladder
lithiasis, low hematocrit level, and previous surgery to the bladder or
the prostate. Exclusion criteria in the control group included IPSS >
7, recurrent urinary tract infections, high volume disease, suspicion
of in situ carcinoma, and previous TUR-BT.
Tissue Procurement and
Immunohistochemistry
Bladder
tissue was easily retrieved in patients who underwent suprapubic prostatectomy
whilst, in patients who underwent a TURP, a cold cup biopsy was done in
order to avoid thermal damage to the specimens. Tissue was always retrieved
from the dome of the bladder. Tissue samples were fixed in buffered formalin.
Paraffin-embedded sections were stained with standard hematoxylin and
eosin. The primary antibody used for immunohistochemistry was anti-HIF-1α
(Chemicon Inc., Tenecula, CA format: Purified immunoglobulin, clone: Chemicon
MAB 5382 - antibody specificity: HIF-1α, immunogen: fusion protein from
amino acids 432-528 of human HIF-1α, isotope: IgG2b) and was applied at
a dilution of 1:200.
Antigen retrieval was performed by heating the slides with citrate-buffered
solution in microwave oven for 5 minutes in two cycles. Envision (Dako,
Denmark) was used as secondary antibody. Finally, diaminobenzidine was
applied as chromogen and the slides were slightly counterstained with
hematoxylin. In substitute negative controls, the primary antibody was
omitted and replaced by phosphate-buffered saline.
Two pathologists unaware of the clinical data performed the assessment
of staining. Where results were equivocal, the slides were jointly re-examined
for a final consensus. A minimum of twenty randomly selected, high-power
fields through the whole section was examined and not quantitative histology
software was used.
The assessment of HIF-1a was based on a previously described method (11).
HIF-1a immunoreactivity was expressed in nucleus and cytoplasm of stromal
cells. The assessment of staining was carried out according to the number
of positive cells and staining distribution. Specimens were grouped into
high and low HIF-1α reactivity using a cut off point of 80 reactive cells/slide,
which represents the lowest 95% CI value.
Statistics
Data were analyzed through descriptive statistics and for statistical reasons the categorical nature of HIF-1a staining was used. Chi-square test was used to test statistical significance in categorical variables and odds ratios to quantify the strength of association. Differences of categories were evaluated with Kruskall-Wallis and analysis of variance when appropriate, Mann-Whitney-U and Student’s-t-test were used to estimate differences among groups.
RESULTS
The examined baseline parameters of the patients are listed in Table-1. Differences between patients under α1-blocker medication (n = 40) and without medication (n = 20) in terms of age, IPSS, Vpr, PVR, and Qmax were not statistically significant. The risk, however, to present at least one episode of acute urinary retention, was 3-fold more probable in patients who never used α1-blockers (p = 0.044) OR = 3.439 (95 % CI 1.05-11.06). Subjects under α-blocker treatment were obstructed for a shorter period [mean 3.82 ± 4.11 vs. 6.14 ± 4.33 years (p = 0.019)], which reflects the time receiving medication.
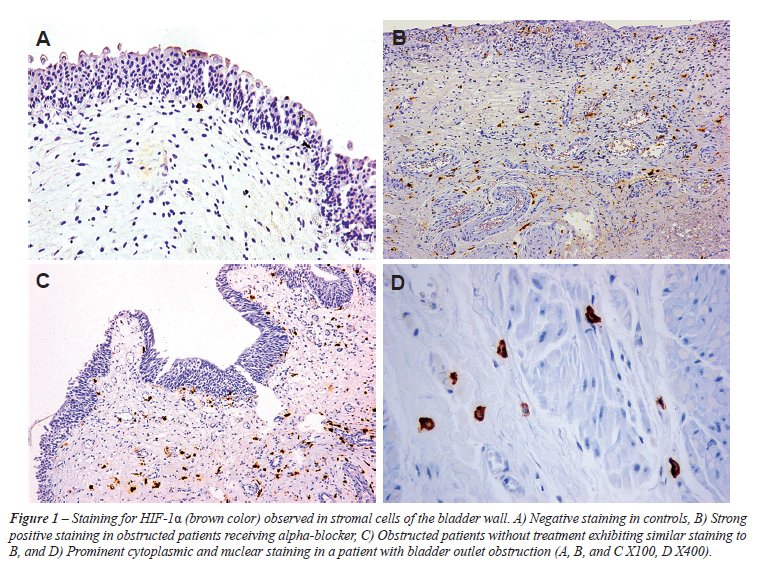
Bladder tissue from obstructed subjects
showed high immunoreactivity to HIF-1α (mean number of total positive
cells 88 ± 48.1), which was diffusely distributed among positive
cells and was mainly nuclear and only weakly cytoplasmic (Figure-1). The
specimens from the control group, showed no or weak, mainly cytoplasmic
immunoreactivity to HIF-1α (< 0-2 ± 0.0) (Figure-1).
Cells expressing HIF-1α, both from obstructed and control group
patients (in control group when present) were stromal cells located in
different proportions between muscle bundles and submucosa, while the
urothelium and the detrusor muscle did not show any kind of immunoreactivity.
The difference among study cohort and control group was significant (p
< 0.001).
The
two groups did not differ in the number of HIF-1α positive cells,
(mean number 88.6 ± 49.6 in those under medication, 86.8 ±
45.8 in the later) (p = 0.78). Stromal cells exhibited strong positive
staining for HIF-1α, in both its nuclear and cytoplasmic components.
Twenty patients underwent urodynamic evaluation;
the characteristics are summarized in Table-2. Nine patients were characterized
as low immunoreactivity and 11 as high reactivity according to HIF-1α
positive cells. The 2 groups did not differ regarding age, IPSS, Vpr,
PSA, PVR and Qmax. No difference was detected among urodynamic parameters
between the two groups, while the lowest bladder pressure at which HIF-1a
was up-regulated was detected at PdetQmax = 60 cm H2O, which corresponded
at high HIF-1α protein expression (PdetQmax 101.1 ± 29.1
range 60-130 cm H2O) (Table-2).
COMMENTS
In the present
study, HIF-1a expression was higher in subjects with BOO than controls,
demonstrating that obstructed bladder becomes hypoxic, as previously reported
(12). The authors suggested that bladder stromal cells were those to perceive
low oxygen tension, while the detrusor and the urothelium seems to be
more resistant.
Another important finding is that HIF-1α protein expression is the same
among patients under treatment with a1-blockers who are finally operated
and those without treatment, giving evidence that medication did not influence
tissue hypoxia in chronic BOO. The role of a1-blockers in bladder metabolism
and hypoxia has not been previously investigated, even though several
papers have been published regarding the role of this medication on bladder
function (1,2).
Study group and control group were well balanced regarding age, IPSS,
Vpr and other comorbid conditions, in an effort to avoid bias between
the two groups, on factors that could influence tissue hypoxia (diabetes,
hypertension, smoking, high cholesterol) (13). Chronic tissue ischemia
results in detrusor smooth muscle replacement with collagen, followed
by impaired contractility and overactivity with loss of bladder compliance
(14).
However, the same changes are observed in chronic BOO, with detrusor dysfunction
and tissue hypoxia being the result of high intravesical pressure, generated
to overcome the resistance to flow. Bladder blood flow decreases during
filling along with the rise of intravesical pressure. Before voiding,
intravesical pressure increases, while bladder neck relaxes and the resistance
to flow drops; a plateau phase is reached, where intraluminal pressure
remains constant to achieve complete emptying. In BOO, this phase is prolonged
and voiding may still be complete, at the cost, however, of tissue ischemia.
In experimental models with obstructed animals, during the voiding phase,
bladder wall blood flow decreases to the same extent as in the non-obstructed
animals. Nevertheless, since emptying is sustained, significant detrusor
hypoxia occurs and detrusor pressure becomes the main determinant of blood
flow (15).
Pinggera and colleagues measured blood perfusion in arteries in the bladder
neck and the prostate at different filing volumes using Doppler ultrasound,
while they assessed the influence of α1-blockers in the perfusion of the
same arteries during filling. They concluded that perfusion is reduced
in LUTS patients and increases to almost normal levels after α1-blocker
treatment, suggesting that treatment improved perfusion in the lower urinary
tract (16). However, in the aforementioned work, blood flow at the dome
and the posterior wall was not investigated, while perfusion was not measured
during bladder emptying. The vessels that authors measured for perfusion
were in the bladder neck and prostate and not those that travel in bladder
wall (17), the vessels in the trigone are arranged in a looser network
with more uniform and larger diameter (18). Therefore, there is no definite
conclusion that treatment with a-blockers improved perfusion in the hall
bladder.
In human bladders without obstruction, there is a 2-fold increase in bladder
blood flow associated with filling, compared to the empty state, as measured
with laser Doppler in the posterior wall (17). It seems that the posterior
wall and the dome of the bladder are more vulnerable to bladder pressure
(17,18). The investigators also found that bladder blood flow reaches
peak at detrusor pressure of 23 cm H2O. On the other hand, blood flow
is decreased to approximately 1.2 times the base line flow, in detrusor
pressure of 43 cm H2O, which is measured at maximum cystometric capacity.
However, despite the high pressure, it remains higher compared to the
empty state. Additionally, those with decreased bladder compliance had
lower perfusion at empty bladder, a smaller increase of blood flow with
filling, and a lower perfusion at maximum cystometric capacity. Nevertheless,
in this work it could not be addressed whether the causative factor for
the low compliance was ischemia or the exact opposite (17). As the authors
state, bladder perfusion still remains normal even at intraluminal pressure
of 43 cm H2O which corresponds to filling at the maximum cystometric capacity.
In obstructed patients, however complete voiding requires much higher
pressures.
Recently it has been described that HIF-1α expression was higher in patients
with retention. It is known that urodynamics performed shortly after an
episode of retention shows a decompensated bladder with intravesical pressures
not exceeding 20-30 cm H2O. After a period however of 11 to 50 days detrusor
regains its function and can generate intravesical pressures at maximum
flow even of 81.6 (35.2) cm H2O (17). It is common practice to wait at
least several weeks after an acute episode of urinary retention before
performing surgical treatment for BOO, since prostatectomy immediately
after such episode is associated with higher morbidity and mortality (19).
Acute detrusor decompensation on the other hand and post void residual
is a consequence of depletion of energetic reserves and HIF-1α is known
to participate in the cellular metabolism by inducing enzymes in the glycolitic
pathway (12). These results may explain why HIF-1α was found up-regulated
in patients with retention as in our cohort of patients.
In the present study, tissue specimens were obtained from the dome of
the bladder, since during filling the dome has the lowest perfusion. Therefore,
we hypothesized that hypoxia would be more pronounced at this location
(20). We also used urodynamics to identify the lowest bladder pressure
at which HIF-1α is up-regulated, although this was not possible. In our
patients, the lowest detrusor pressure to detect HIF-1α was at 60 cm H2O
and corresponded to a high protein expression. Furthermore, there was
no difference among urodynamic parameters between high and low reactivity
patients. The expression of HIF-1α gives evidence that above the normal
detrusor pressure for voiding (roughly 20-30 cm H2O) the bladder becomes
hypoxic.
The urodynamic effect of α1-blockers has been extensively explored in
earlier studies. It has been found that treatment with α1-blockers increased
average maximum flow rate to 2.9 mL/s (range 0.9-5.6 mL/s) and the PdetQmax
decreased to average 17.4 cm H2O (38.2-0.0 cm H2O) from a base line of
85.1 cm H2O (range 70-100.4 cm H2O) to 67.1 cm H2O (range 39.7-93 cm H2O),
but this interval is always above normal detrusor pressure, for non obstructed
voiding (17-21). Patients in these studies however, experienced marked
symptomatic improvement as assessed by IPSS, although still remaining
obstructed. This may explain why these medications do not influence disease
progression as defined by the need for invasive treatment and acute urinary
retention (2). Recently, Barendrecht and associates questioned the fact
that a1-blockers improve LUTS by reducing BOO. In this work, BOO index
improved only slightly compared to IPSS and maximum flow, so the investigators
stated that these medications function differently than relaxing prostate
smooth muscle (22).
Our study is not without drawbacks. Firstly, we used immunohistochemistry
to characterize bladders as hypoxic rather than quantify the levels of
HIF-1α. Immunohistochemical evaluation of tissue protein expression is
susceptible to intraobserver and interobserver variability, however, quantification
of the HIF-1α is not necessary for the evaluation of hypoxia, since we
used the categorical nature of HIF-1α protein expression in order to minimize,
as possible, the aforementioned limitations. Additionally, we used HIF-1α
as a marker of tissue hypoxia, despite the fact that it can also be induced
in non ischemic tissues. HIF-1α accumulates in myocytes as an early response
to mechanical stress in hearts with diastolic pressure increase, followed
by enhanced expression of VEGF genes. Similarly, in obstructed bladders,
HIF-1α may also be induced by mechanical stress. Even if this is the case
in BOO, treatment with α-blockers does not decrease bladder wall tension
to preobstructed levels giving a further stimulus to HIF-1α induction.
It would be interesting to verify if HIF-1α levels normalize after the
obstruction is relieved. We are also aware that urinary retention may
affect HIF-1α expression to those not receiving α1-blocker treatment (12).
CONCLUSIONS
Treatment with α-blockers in obstructed patients does not seem to result in HIF-1α down-regulation. It is likely that once obstruction has settled, medication does not change bladder metabolism, which continues to be under chronic stress. Further studies are needed to confirm the present results, and clarify the role of α1-antagonists on bladder homeostasis in chronic BOO.
ACKNOWLEDGMENTS
We would like to thank Douka Despina for her support to the study and Kemerli Maria for her assistance with the immunohistochemical analysis.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Lee E, Lee C: Clinical comparison of selective and non-selective alpha 1A-adrenoreceptor antagonists in benign prostatic hyperplasia: studies on tamsulosin in a fixed dose and terazosin in increasing doses. Br J Urol. 1997; 80: 606-11.
- McConnell JD, Roehrborn CG, Bautista OM, Andriole GL Jr, Dixon CM, Kusek JW, et al.: The long-term effect of doxazosin, finasteride, and combination therapy on the clinical progression of benign prostatic hyperplasia. N Engl J Med. 2003; 349: 2387-98.
- Greenland JE, Brading AF: Urinary bladder blood flow changes during the micturition cycle in a conscious pig model. J Urol. 1996; 156: 1858-61.
- Brading AF: Alterations in the physiological properties of urinary bladder smooth muscle caused by bladder emptying against an obstruction. Scand J Urol Nephrol Suppl. 1997; 184: 51-8.
- Salceda S, Caro J: Hypoxia-inducible factor 1alpha (HIF-1alpha) protein is rapidly degraded by the ubiquitin-proteasome system under normoxic conditions. Its stabilization by hypoxia depends on redox-induced changes. J Biol Chem. 1997; 272: 22642-7.
- Lee JW, Bae SH, Jeong JW, Kim SH, Kim KW: Hypoxia-inducible factor (HIF-1)alpha: its protein stability and biological functions. Exp Mol Med. 2004; 36: 1-12.
- Hoppeler H, Vogt M: Muscle tissue adaptations to hypoxia. J Exp Biol. 2001; 204: 3133-9.
- Kietzmann T, Görlach A: Reactive oxygen species in the control of hypoxia-inducible factor-mediated gene expression. Semin Cell Dev Biol. 2005; 16: 474-86.
- Chandel NS, Maltepe E, Goldwasser E, Mathieu CE, Simon MC, Schumacker PT: Mitochondrial reactive oxygen species trigger hypoxia-induced transcription. Proc Natl Acad Sci U S A. 1998; 95: 11715-20.
- Duranteau J, Chandel NS, Kulisz A, Shao Z, Schumacker PT: Intracellular signaling by reactive oxygen species during hypoxia in cardiomyocytes. J Biol Chem. 1998; 273: 11619-24.
- Birner P, Schindl M, Obermair A, Plank C, Breitenecker G, Oberhuber G: Overexpression of hypoxia-inducible factor 1alpha is a marker for an unfavorable prognosis in early-stage invasive cervical cancer. Cancer Res. 2000; 60: 4693-6.
- Koritsiadis G, Stravodimos K, Koutalellis G, Agrogiannis G, Koritsiadis S, Lazaris A, et al.: Immunohistochemical estimation of hypoxia in human obstructed bladder and correlation with clinical variables. BJU Int. 2008; 102: 328-32.
- Ponholzer A, Temml C, Wehrberger C, Marszalek M, Madersbacher S: The association between vascular risk factors and lower urinary tract symptoms in both sexes. Eur Urol. 2006; 50: 581-6.
- McVary KT: Erectile dysfunction and lower urinary tract symptoms secondary to BPH. Eur Urol. 2005; 47: 838-45.
- Greenland JE, Brading AF: The effect of bladder outflow obstruction on detrusor blood flow changes during the voiding cycle in conscious pigs. J Urol. 2001; 165: 245-8.
- Pinggera GM, Mitterberger M, Pallwein L, Schuster A, Herwig R, Frauscher F, et al.: alpha-Blockers improve chronic ischaemia of the lower urinary tract in patients with lower urinary tract symptoms. BJU Int. 2008; 101: 319-24.
- Kershen RT, Azadzoi KM, Siroky MB: Blood flow, pressure and compliance in the male human bladder. J Urol. 2002; 168: 121-5.
- Miodonski AJ, Litwin JA: Microvascular architecture of the human urinary bladder wall: a corrosion casting study. Anat Rec. 1999; 254: 375-81.
- Dubey D, Kumar A, Kapoor R, Srivastava A, Mandhani A: Acute urinary retention: defining the need and timing for pressure-flow studies. BJU Int. 2001; 88: 178-82.
- Batista JE, Wagner JR, Azadzoi KM, Krane RJ, Siroky MB: Direct measurement of blood flow in the human bladder. J Urol. 1996; 155: 630-3.
- Kortmann BB, Floratos DL, Kiemeney LA, Wijkstra H, de la Rosette JJ: Urodynamic effects of alpha-adrenoceptor blockers: a review of clinical trials. Urology. 2003; 62: 1-9.
- Barendrecht MM, Abrams P, Schumacher H, de la Rosette JJ, Michel MC: Do alpha1-adrenoceptor antagonists improve lower urinary tract symptoms by reducing bladder outlet resistance? Neurourol Urodyn. 2008; 27: 226-30.
____________________
Accepted
after revision:
August 11, 2009
_____________________
Correspondence
address:
Dr. Stavros Tyritzis
LAIKO Hospital, Department of Urology
Athens University Medical School
17 Agiou Thoma str.
11527, Athens, Greece
Fax: + 0030 210 9327-744
E-mail: statyr@freemail.gr
EDITORIAL COMMENT
Benign prostatic
obstruction will induce bladder hypoxia, which could be detected by elevation
of bladder tissue HIF-1-a . The authors studies the effects of a-blocker
treatment on bladder HIF-1-a regulation during lower urinary tract obstruction
and concluded that a blocker has no effect on bladder tissue HIF-1-a expression.
It is an interesting study, but some bias from the current groups need
to be cleared.
As all of the biopsy patients are alpha-blocker non-responder, I would
contend that the responders may show lower HIF-1 a than the non-responder.
By means of laser Doppler flowmeter, Lin et al. demonstrated that the
obstructed bladders from rabbits with partial outlet obstruction had significantly
lower blood flow than the ischemic bladders (1). After 8 weeks partial
outlet obstruction, bladder from rabbits with supplement of L-arginine
showed significantly greater contractile function compared with the no-treatment
group (2). The study demonstrated that increasing blood flow by stimulating
nitric oxide synthase significantly protected the bladder from partial
bladder outlet obstruction dysfunctions. Therefore, the patients with
lower urinary tract obstruction might still be able to get partial recovery
of bladder flow, reverse of ischemia change, and improve bladder function
through some therapy.
REFERENCES
- Lin WY, Mannikarottu A, Li S, Juan YS, Schuler C, Javed Z, et al.: Correlation of in vivo bladder blood flow measurements with tissue hypoxia. World J Urol. 2009; 4. [Epub ahead of print]
- Lin WY, Levin RM, Chichester P, Leggett R, Juan YS, Johnson A, et al.: Effects of L-arginine and L-NAME on chronic partial bladder outlet obstruction in rabbit. Am J Physiol Regul Integr Comp Physiol. 2007; 293: R2390-9.
Dr. Yao-Chi
Chuang
Division of Urology
Chang Gung Memorial Hospital
Kaohsiung Medical Center
Kaohsiung, Taiwan
E-mail: chuang82@ms26.hinet.net
EDITORIAL COMMENT
This well
written paper offers new insight novel mechanism of action a-blocker treatment
my have on the obstructed bladder. This study lends further evidence that
a-blocker’s benefit in cases of bladder outlet obstruction (BOO)
may be more on the bladder than urethral outlet.
George and associates from Athens assessed whether a1-blocker treatment,
in chronic BOO, influences bladder tissue ischemia. They studied 60 patients
with BOO, 40 with and 20 without a1-blockers, respectively. At time of
transurethral or suprapubic prostatectomy, bladder biopsies were taken
for immunohistochemically stained for Hypoxia Inducible Factor-1a (HIF-1a).
Ten patients with non muscle invasive bladder cancer underwent transurethral
resection of the tumor served as control group.
This study found that HIF-1a expression was higher in patients with BOO
than controls, demonstrating that obstructed bladder becomes hypoxic.
Another important finding is that HIF-1a protein expression is the same
among patients under treatment with a1-blockers who are finally operated
and those without treatment. It is likely that once obstruction has settled,
medication does not change bladder metabolism, which continues to be under
chronic stress. Further studies are needed to clarify the role of a1-antagonists
on bladder homeostasis in chronic obstruction.
Dr.
Michael B. Chancellor
Neurourology Program
William Beaumont Hospital
Royal Oak, MI, 48073, USA
E-mail: chancellormb@gmail.com