CONSTIPATION
AND LUTS - HOW DO THEY AFFECT EACH OTHER?
(
Download pdf
)
Review Article
Vol. 37 (1):
16-28, January - February, 2011
doi: 10.1590/S1677-55382011000100003
MARCIO A. AVERBECK, HELMUT MADERSBACHER
Department of Urology (MAA), Mae de Deus Center Hospital, Porto Alegre, Brazil and Department of Neurology (HM), Medical University Innsbruck, Innsbruck, Austria
ABSTRACT
Context:
Urinary bladder and rectum share a common embryological origin. Their
autonomic and somatic innervations have close similarities. Moreover,
the close proximity of these two organ systems could suggest that dysfunction
in one may influence, also mechanically, the function of the other. Therefore,
it is not surprising that defecation problems and lower urinary tract
symptoms (LUTS) occur together, as reported in the literature.
Objective: To study the relationship between
constipation and LUTS focusing on what is evidence-based.
Evidence acquisition: We searched the Medical
Literature Analysis and Retrieval System Online (MEDLINE) database in
February 2010 to retrieve English language studies (from 1997 to 2009)
and the 2005, 2006 and 2007 abstract volumes of the European Association
of Urology (EAU), American Urological Association (AUA) and International
Continence Society (ICS).
Evidence synthesis: We present the findings
according to the studied population in four groups: (a) children, (b)
middle-aged women, (c) elderly and (d) neuropathic patients. Most published
studies that correlated rectal and bladder dysfunction were carried out
in children or in young women. On the other hand, there are few studies
regarding the association between constipation and LUTS in the elderly
and in neuropathic patients.
Conclusions: Several studies in children
documented that constipation is linked to urinary tract problems, including
infections, enuresis, vesicoureteral reflux and upper renal tract dilatation.
The underlying pathophysiology of these findings has not yet been clearly
defined. Studies in middle-aged women also support a high prevalence of
constipation among patients suffering from urinary tract dysfunction.
Furthermore, an association between constipation and urinary incontinence,
as well as between constipation and pelvic organ prolapse, has been suggested.
The only prospective study in constipated elderly with concomitant LUTS
demonstrates that the medical relief of constipation also significantly
improves LUTS. Finally, the available data on neuropathic patients suggest
that stool impaction in the rectum may mechanically impede bladder emptying.
However, most of the studies only include a small number of patients,
are not prospective and are uncontrolled. Therefore, there is a need for
large-scale, controlled studies to further improve evidence and to provide
a valid recommendation for all groups, especially for the elderly and
neuropathic patients.
Key words:
constipation; defecation; urinary tract; urinary tract diseases; urinary
incontinence
Int Braz J Urol. 2011; 37: 16-28
INTRODUCTION
The
urinary bladder and the rectum have a common embryological origin in the
cloaca. The motor nerve supply of each is provided by the parasympathetic
outflow arising from S2-S4. The same is true for the external (striated)
anal and for the external (striated) urethral sphincter; both are innervated
by the pudendal nerve, arising from the Onuf’s nucleous in S2-S4.
In healthy individuals bladder and rectum function are “in harmony”
(1). However, constipation and lower urinary tract symptoms (LUTS) can
occur concomitantly in children, women, the elderly, as well as in neuropathic
patients.
Autonomic reflex interaction between the urinary bladder and the distal
part of the gastrointestinal tract has been investigated in animal models
and humans (2). It has been demonstrated that anal stimulation abolishes
a prevailing detrusor contraction. On the other hand, distension of the
urinary bladder in man produces an increase in internal anal sphincter
pressure. This response is abolished by blockade of the thoracolumbar
sympathetic outflow by epidural anaesthesia, indicating a spinal reflex
arc (2).
The coincidence of defecation problems and
LUTS reported in the literature may have several different aetiologies:
(a) it may be that rectum and bladder are affected by the same neuropathology;
(b) that dysfunction in one system may impede the neighbouring organs
and structures mechanically, e.g. stool impaction from severe constipation
may impede voiding; or (c) severe straining due to constipation may induce
changes in the pelvic floor musculature, resulting in pelvic organ prolapse
(POP) and urinary incontinence.
Most studies that correlated rectal and
bladder dysfunction were carried out in children or in middle-aged women,
but there is only one prospective cohort study, to our knowledge, regarding
constipation and LUTS in the elderly (1). One of the difficulties to conduct
clinical studies, including bowel dysfunction is the subjective aspect
associated with the definition of constipation (3). Some studies used
self-applied questionnaires where the patients could define themselves
as constipated or not. Only recently, has chronic functional constipation
been clearly defined (4).
The aim of this review was to study the
relationship between constipation and LUTS, focusing on what is evidence-based
and what can be recommended so far from the diagnostic and therapeutic
point of view.
EVIDENCE ACQUISITION
- SEARCH STRATEGY
A
literature search was performed in the Medical Literature Analysis and
Retrieval System Online (MEDLINE) database in February 2010 to retrieve
English language studies (from 1997 to 2009) on the association between
constipation and LUTS.
For retrieving the references in MEDLINE
we used the following medical subject heading terms: “constipation”
(major subject descriptor) and “defecation”, “urinary
tract”, “urinary tract diseases”, “urinary tract
infections”, “urinary incontinence” or “urinary
retention” (subject descriptors). Furthermore, we searched the abstract
volumes of the annual meetings of 2007, 2008 and 2009 of the European
Association of Urology the American Urological Association and the International
Continence Society meetings.
DEFINITION OF CONSTIPATION
Constipation is an end-point defined by a constellation of symptoms, including infrequent passage of stool, faeces that are either large, hard or in small pieces, abdominal pain, palpable stool in the abdomen, stool in the rectal vault or faecal soiling. Functional constipation (FC) is considered a symptom-based disorder that is characterized by both decreased frequency and hard consistency of stools, as well as symptoms relating to difficult evacuation (5). Table-1 presents the Rome III criteria for chronic functional constipation in adults and in children (4). Other terms and definitions have been used by some authors. Obstructive defecation was defined as difficulty in passing stool, hard stool, straining for more than 15 min., or incomplete evacuation, occurring at least weekly (6). Anal incontinence was defined as involuntary leakage of solid or liquid faeces or gas (7). Finally, dysfunctional elimination syndrome (DES) has been defined as any pattern of voiding or stooling that varies from the developmental norm (8).
EVIDENCE SYNTHESIS ACCORDING
TO THE STUDIED POPULATION
The studies on Constipation and LUTS will be presented and discussed, as well as the levels of evidence (LoE) and grades of recommendation (GR). The publications were organized according to the studied population in four groups: Children, Middle-Aged Women, Elderly, Neuropathic Patients. We were able to retrieve altogether 8 case-reports, 5 review studies, 3 case-control studies, 3 case-series, 6 cross-sectional studies, 5 cohort studies and 1 non-controlled clinical study. Table-2 lists the review articles on constipation and LUTS published so far. Table-3 and Table-4 lists the published studies on children and middle-aged women, respectively, and Table-5 shows the studies, only case-reports, in neuropathic patients.
CONSTIPATION AND LUTS
IN CHILDREN
Constipation
is responsible for 3% of visits to a paediatrician and 25% of consultations
with a gastroenterologist. Children diagnosed with constipation frequently
have a poor appetite and have been shown to have a lower calorie and fibre
intake, lower body mass index and more frequent anorexia than non-constipated
children (9). Some children voluntarily suppress the urge to defecate
and they refuse toileting, although a strong need to defecate is present.
Withholding behaviour over time can cause DES (8). This behaviour may
be due to an impairment of learning subsequent to distress, trauma, disruption
of routine, inattention or cognition difficulties and is often associated
with the memory or expectation of pain at defecation. Also the presence
of an anal fissure or an anal streptococcal infection may induce this
behaviour (9). Environmental factors regarding toilets, lack of privacy,
risk of bullying, limited access, lack of essential products for good
hygiene and dirty bathrooms can all contribute in encouraging a child
to withhold urine and stool while at school.
There are 12 studies addressing the relationship
between constipation and LUTS on children (10-21). Table-3 summarizes
these studies, as well as, the LoE and GR, number of patients included
in each study and their mean age. The important findings will be discussed
in detail.
Loening-Baucke (10) published a cohort study evaluating the frequency
of urinary incontinence and urinary tract infection in constipated children
and the effect of successful treatment of constipation on urologic symptoms:
234 chronic constipated and encopretic children were evaluated before
and at least 12 months after the treatment for constipation (mean follow-up
= 15 months), which was successful in 52% of the children. In this group,
relief of constipation resulted in disappearance of daytime urinary incontinence
in 89% and night-time urinary incontinence in 63% of patients, and disappearance
of recurrent urinary tract infections in all patients who had no anatomic
abnormality of the urinary tract. This study showed that with treatment
of the constipation, most children became clean and dry and recurrence
of urinary tract infections was prevented (LoE 1B / GR B).
McGrath et al. (11) performed a prospective
cross-sectional study of children with enuresis at presentation to a continence
service. Data relating to the child’s bowel habits, pattern of enuresis
and other history items were obtained from parental questionnaires and
paediatrician’s assessments. Of the 277 participants aged 4.8-17.5
years (median 8.6 years), 100 (36.1%) were identified as constipated by
the clinician, compared with only 39 (14.1%) from parental reporting (Kappa
= 0.155; P = 0.003). Constipation was high among children with enuresis,
but was often not recognized by parents (LoE 2 / GR B).
Kajiwara et al. (15) retrospectively studied
the differences between monosymptomatic and non-monosymptomatic enuresis
on the basis of LUTS and constipation. Eighty-eight patients (9.8 ±
3.1 years old) were enrolled, 67 with monosymptomatic and 21 with non-monosymptomatic
enuresis. Besides a history of urinary tract infections, mechanical obstructions
and vesicoureteral reflux, constipation was also strongly associated with
non-monosymptomatic enuresis compared to monosymptomatic enuresis (LoE
2 / GR C).
Bael et al. (12) studied the efficacy of treating urinary incontinence
(UI) in children with concomitant functional fecal incontinence (FFI)
or FC. After treatment of UI, FFI dropped from 32% to 21% (P = 0.035);
for FC, the number of evaluated children was too small. Although the studied
population was rather small, the outcome supports a mutual relationship
between LUTS and bowel dysfunction (LoE 2 / GR B).
Koff et al. (13) performed a prospective
cohort study to evaluate the prevalence of DES in children with vesicoureteral
reflux and to determine whether functional bladder and/or bowel disorders
influence the natural history or treatment of children with primary vesicoureteral
reflux. One hundred and forty-three children with primary vesicoureteral
reflux, that stopped spontaneously or was surgically corrected, were included.
Unsuccessful surgical outcomes involving persistent, recurrent and contralateral
reflux occurred only in children with DES. The authors concluded that
dysfunctional elimination syndromes are common and are often unrecognized
in children with primary reflux. These syndromes are associated with delayed
reflux resolution and an increased rate of breakthrough urinary tract
infection, which leads more frequently to reimplantation surgery (LoE
2 / GR B).
Loening-Baucke (14) evaluated the prevalence
rates for constipation, as well as of faecal and urinary incontinence
in children attending primary care clinics in the United States. 482 children
(7-17 years of age) were included in the study. The prevalence rate for
constipation was 22.6% and was similar in boys and girls. The prevalence
rate for faecal incontinence (> or = 1/week) was 4.4%. Faecal incontinence
was associated with constipation in 95% of the patients. The prevalence
rate for urinary incontinence was 10.5%; 3.3% for daytime only, 1.8% for
day- and night-time and 5.4% for night-time urinary incontinence. Faecal
and urinary incontinence were significantly more commonly observed in
children with constipation than in children without constipation. Children
with constipation had higher prevalence rates not only for faecal but
also for urinary incontinence than children without constipation (LoE
2 / GR C).
De Paepe et al. (16) analysed the results
after treating young children with LUTS and constipation, using a noninvasive
training programme. Therapy consisted of keeping a voiding and drinking
chart, instructions on proper toilet posture, daily rules for application
at home, and if possible relaxation biofeedback of the pelvic-floor muscles.
Twenty children were treated and 13 had a good result (became dry during
the day and night, and encopresis resolved). This study shows that pelvic-floor
muscle- and toilet training can improve both LUTS and constipation, but
the studied population was very small and there was no control group (LoE
2 / GR C).
CONSTIPATION AND LUTS IN MIDDLE-AGED WOMEN
Constipation may affect 12 to 32% of middle-aged women (6,7). Women with constipation are more likely than men to seek medical attention or use medication for this condition. There are 5 studies examining the prevalence of constipation and its association with LUTS and/or POP in middle-age women (6,7,22-24). These studies are summarized in Table-4.
Varma et al. (6) analysed data from a randomly
selected cohort of 2,109 women, 40-69 years old, to describe the prevalence
of obstructive defecation and identify associated risk factors. Obstructive
defecation that occurred at least weekly was reported by 12.3% of women.
Significant independent risk factors included vaginal or laparoscopic
hysterectomy [odds ratio (OR) = 2.01; 95% confidence interval (CI) = 1.15-3.54],
using three or more medications [1.81 (1.36-2.42)], symptomatic pelvic
organ prolapse [2.34 (1.47-3.71)], urinary incontinence surgery [2.52
(1.29-4.90)], and other pelvic surgery [1.35 (1.03-1.78)]. Women who had
undergone laparoscopic/vaginal hysterectomies or surgery for pelvic organ
prolapse or for urinary incontinence had a nearly two times higher risk
for obstructive defecation (LoE 2 / GR B).
Ewings et al. (22) performed a cohort study
assessing risk factors for developing urinary incontinence following childbirth.
A total of 723 women were recruited from the study. At 6 months post-partum,
45% of women reported some incontinence problems. Chronic constipation
was the second strongest predictor for post-partum incontinence (OR =
1.86; 95% CI = 1.03-3.34), along with a pre-existing incontinence problem
[4.49 (3.09-6.53)] and episiotomy in at least one delivery [1.96 (1.25-3.07)]
(LoE 2 / GR C).
Soligo et al. (7) analysed the prevalence
and patterns of constipation in women with urinary symptoms and/or genital
prolapse. Seven hundred and eighty-six consecutive urogynaecological patients
participated in a questionnaire and structured clinical assessment. Thirty-two
percent of women were constipated. A genital prolapse of grade 2 or more
occurred in 44% of women. A posterior colpocele was more frequent in constipated
women (35% vs. 19%; p < 0.0001), resulting in a risk factor for constipation
(OR = 2.31; 95% CI = 1.63-3.27). By contrast, higher degrees of anterior
colpocele appeared to protect against constipation [0.80 (0.66-0.96)].
Constipation correlated exclusively with posterior aspects of the pelvic
floor support (LoE 2 / GR C).
Spence-Jones et al. (24) performed a case-control
study to investigate the aetiological importance of constipation in patients
with uterovaginal prolapse and urinary stress incontinence. Twenty-three
women with uterovaginal prolapse (mean age 57 years), 23 women with urinary
stress incontinence (mean age 52 years) and 27 control women (mean age
52 years) were included. All three groups were comparable in terms of
parity, age and birth weight of children. However, constipation as a young
adult prior to the development of urogynaecological symptoms was significantly
more common in women with uterovaginal prolapse (61% vs. 4%; P < 0.001)
and women with urinary stress incontinence (30% vs. 4%; P < 0.05),
compared to controls. At the time of consultation, 95% of the women with
uterovaginal prolapse were constipated, compared with only 11% of control
women. Constipation, in addition to obstetric history, appears to be an
important factor in the pathogenesis of uterovaginal prolapse and stress
urinary incontinence (LoE 3 / GR C).
Ng et al. (23) evaluated the prevalence
of anorectal dysfunction among women with LUTS. All 320 women who attended
the urogynaecological outpatient clinic for urodynamic evaluation were
requested to complete a structured questionnaire. Forty-nine (15.9%) women
reported having anal incontinence. Constipation was reported by 100 (31.5%)
of the women. A multiple logistic regression analysis revealed that the
main risk factor associated with anal incontinence and constipation was
the presence of uterovaginal prolapse (OR = 5.02; 95% CI = 2.19-11.5 for
anal incontinence; OR = 1.78; 95% CI = 1.03-3.09 for constipation) (LoE
3 / GR C).
CONSTIPATION AND LUTS
IN THE ELDERLY
There is only one prospective cohort study, to our knowledge, evaluating the effect of alleviating constipation on LUTS in the elderly (1). Charach et al. studied fifty-two patients, aged 65-89 (mean 72 ± 13) years, with chronic constipation and LUTS, recruited from gastroenterology and urology clinics.(1) All patients were generally mobile, sensitive and continent. Before treatment of constipation was initiated, patients completed a questionnaire regarding their constipation pattern, LUTS, sexual function and mood. The follow-up was 4 months. Successful treatment of constipation increased the number of weekly defecations from 1.5 ± 0.9 to 4.7 ± 1.2 (P < 0.001); patients spent less time on the toilet (25 ± 2.1 versus 63 ± 1.9 min; P < 0.0001); fewer patients reported urgency (16 vs. 34; P < 0.001), frequency (25 vs. 47; P < 0.001) and burning sensation during urination (6 vs. 17; P < 0.05). At the same time, there was also an improvement in the scoring of urgency, frequency and burning sensation (from a baseline of 52 to 126, 131 and 95, respectively; P < 0.001). Urinary stream disturbances improved in 32 of the 52 patients (P < 0.001). Residual urine volume decreased from 85 ± 39.5 to 30 ± 22.56 mL (P < 0.001). There was also a significant decrease in the number of patients with bacteriuria events (5 vs. 17; P < 0.001), and an improvement in sexual activity and mood (P < 0.05). Treatment of constipation significantly improved LUTS, as well as, patient’s mood, sexual activity and quality of life (LoE 2, GR B).
CONSTIPATION AND LUTS IN THE NEUROPATHIC PATIENTS
Neuropathic
lower urinary tract dysfunction and neuropathic colorectal dysfunction,
as in patients with spinal cord lesions, share several similarities. The
affected nerves causing the dysfunction are similar and the pattern of
bowel and bladder dysfunction may change over the years (25). However,
there are only case-reports and review studies (26-30) addressing constipation
and LUTS in neuropathic patients. Table-5 provides the case-report studies
published so far.
Only recently, Pannek et al. (26) published
an interesting article reporting two cases with mechanical compression
of the urinary bladder by an over distended bowel. The first patient (63
year-old male), who had post-traumatic paraplegia sub Th 7 since 17 years,
was performing intermittent catheterization and was referred because of
recurrent urinary tract infections and urinary incontinence. He showed
a distended abdomen and palpable masses in the left lower quadrant. Digital
rectal examination revealed massive stool masses. Computed tomography
showed dilatation of the colon, completely filled with stool, compressing
the bladder and the left ureter, resulting in upper urinary tract dilatation.
The second patient (62 year-old male), with post-traumatic quadriplegia
sub C 7 since 42 years, had undergone sacral deafferentation and implantation
of a Brindley anterior root stimulator. He presented with urinary retention
since 3 days, due to malfunction of the Brindley device. Physical examination
revealed a minimally distended abdomen, but with palpable masses in the
left lower quadrant. On digital rectal examination, lumps of hard stool
were detected. Video-urodynamics demonstrated compression of the urinary
bladder against the symphysis, making voiding impossible despite sufficient
detrusor contractions. The patients were properly treated with evacuation
by colonic hydrotherapy. After successful treatment of constipation, upper
urinary tract dilatation resolved in the first patient, and in the second
patient, after re-establishing the function of the Brindley device, with
electrically driven defecation, stool impaction disappeared and electromicturition
was possible. This case report shows that massive stool impaction due
to neuropathic bowel dysfunction can mechanically impede bladder emptying.
COMMENTS
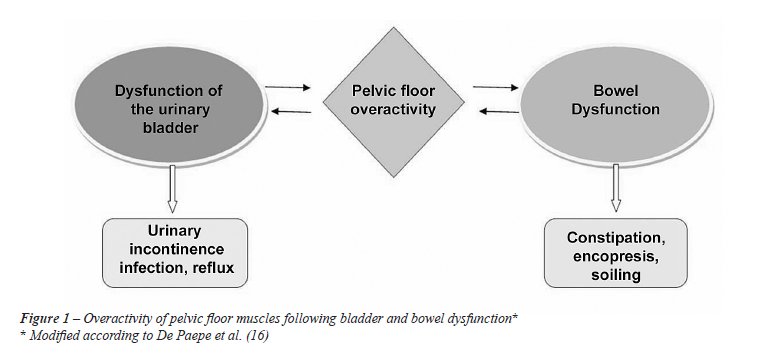
Much attention has been focused on the evaluation of colon, rectum and anus in children with chronic constipation with or without encopresis, but little thought has been given to a possible association to urinary tract symptoms, such as day- and night-time urinary incontinence, urinary tract infection, and urinary retention in these children (10), despite the well-known fact that the lower urinary tract and the lower bowel tract are interrelated structures (31). Anatomically bladder and rectum lay in close communication and share muscular structures of the pelvic floor. Nevertheless, it has been suggested that the distension of the rectum by stool impaction in constipated children presses on the bladder wall causing bladder outflow obstruction, as well as inducing detrusor overactivity (32). Urodynamic studies have reported detrusor overactivity in patients with functional constipation. Additionally, both, bladder overactivity and bowel dysfunction may lead to overactivity of the pelvic floor musculature, resulting in a high muscle tone, which again causes dysfunctional elimination of urine and faeces (Figure-1) (16). A comprehensive medical history along with physical examination must be done for every child either with LUTS and/or with chronic constipation and encopresis, bearing in mind the neighbouring organ systems. It has been shown that it is not enough only asking the parents about the bowel habits of the child, as constipation is frequently not recognized and reported by parents (11). Moreover, it is important to pay attention during the physical examination to findings suggesting stool impaction, such as abdominal masses and/or abdominal distension. Complementary ultrasound may provide additional information on filling condition of colon and rectum.
When a child presents with enuresis, it
is for various reasons important to differentiate between monosymptomatic
and non-monosymptomatic enuresis: it has been shown by Kajiwara et al.
that constipation is more often found in association with non-monosymptomatic
enuresis (15). Also in the setting of vesicoureteral reflux, it makes
sense to search for constipation, because this condition can cause delayed
reflux resolution and urinary tract infections. In this situation, successful
treatment of constipation could avoid breakthrough urinary tract infections,
which are often an indication for reimplantation surgery (13). In children
with constipation and concomitant LUTS, adequate treatment of constipation
also improves or abolishes LUTS. Loening-Baucke et al. performed a prospective
study in this context: disappearance of day- and night-time urinary incontinence,
only by treating constipation, occurred in 89% and 63% of patients, respectively.
Additionally, urinary tract infections disappeared in all patients who
had no anatomic abnormality of the urinary tract (10).
Constipation in women may significantly
impact overall quality of life (33). Bowel habits must be investigated,
especially in women with previous hysterectomy, pelvic organ prolapse
and urinary incontinence surgery, as it was shown that these conditions
are independent risk factors for constipation, probably due to an iatrogenic
lesion of the innervation (6,7,23). In contrast, constipation in young
women is a risk factor for future uterovaginal prolapse and urinary stress
incontinence (24). Constipation has frequently been described to increase
the risk for pelvic organ prolapse (34). Pregnant women should have their
bowel habits investigated, because there is good evidence that chronic
constipation is a risk factor for postpartum urinary incontinence (22).
When a pregnant woman presents with chronic constipation, one should treat
this condition in time as an attempt to prevent postpartum urinary incontinence.
In community-based surveys, faecal incontinence
(FI) is strongly associated with urinary incontinence and overactive bladder
in both men and woman. Among nursing home patients, the association between
urinary incontinence and FI is even stronger (35). It has also been shown
that constipation and urinary symptoms are very common and disturbing
in the elderly population (1). In the only prospective study addressing
this problem in the elderly, Charach et al. (1) have shown that the treatment
of constipation, at the same time, also improves or abolishes the urologic
symptoms as urgency, frequency and burning sensation can be significantly
improved after treatment of constipation. Besides, improvements in sexual
activity and mood have been reported. Thus, it is important to take into
consideration that treatment of chronic constipation in elderly patients,
by appropriate use of stool softeners, adequate fluid intake, exercise
and disimpaction if necessary, may also improve or even cure the urological
symptoms.
Indeed, there are only a few case-reports
addressing the relationship between neuropathic bowel dysfunction and
neuropathic urinary tract dysfunction (26-30). It has been documented
that overdistended bowel can mechanically impede bladder emptying and
can cause upper urinary tract dilatation (26). This has to be considered,
especially at long term follow-up, when upper and/or lower urinary tract
unexpectedly deteriorates; in this situation it is mandatory to exclude
stool impaction by abdominal palpation and digital rectal examination,
as well as by a plain abdominal X-ray, ultrasound and/or computed tomography.
Colonic hydrotherapy is widely used for the treatment of this type of
constipation. In these patients, with successful management of constipation,
the urinary tract function can recover.
CONCLUSIONS
Studies in children have linked constipation to urinary tract problems, including infections, enuresis, vesicoureteral reflux and upper renal tract dilatation. As a consequence of this interaction between bladder and bowel dysfunction, also overactivity of pelvic floor muscles is likely to occur. It is important in children with LUTS also to assess their bowel habits by taking a targeted history and proper clinical examination, as constipation may not be recognized and, thus, may not be reported by the parents. Studies in middle-aged women support a high prevalence of constipation among patients suffering from lower urinary tract dysfunction. There is some evidence for an association between constipation and urinary incontinence, as well as between constipation and POP and vice-versa. The only prospective study regarding the elderly population clearly shows that the medical relief of constipation significantly improves concomitant LUTS, which, in turn, improves the patient’s mood, sexual activity and quality of life. Finally, the available data on neuropathic patients suggest that neuropathic bowel dysfunction with chronic constipation may mechanically cause urinary tract dysfunction. Chronic constipation and stool impaction may develop over many years, e.g. in spinal cord injured patients, and they are often subjectively unaware, of their condition which may be the reason for unexpected and otherwise unexplainable upper urinary tract deterioration and/or lower urinary tract dysfunction. In conclusion, despite the apparent relationship between constipation and LUTS, large scale, prospective, controlled studies are still needed, especially as regards the elderly and the neuropathic population.
ACKNOWLEDGEMENTS
We would like to thank Prof. Gisele Alsina Nader, from Federal University of Health Sciences of Porto Alegre – UFCSPA (Brazil), for her help in classifying the available studies on constipation and LUTS, according to the levels of evidence (LoE) and grades of recommendation (GR).
CONFLICT OF INTEREST
None declared.
REFERENCES
- Charach G, Greenstein A, Rabinovich P, Groskopf I, Weintraub M: Alleviating constipation in the elderly improves lower urinary tract symptoms. Gerontology. 2001; 47: 72-6.
- Buntzen S, Nordgren S, Delbro D, Hultén L: Anal and rectal motility responses to distension of the urinary bladder in man. Int J Colorectal Dis. 1995; 10: 148-51.
- Drossman DA: The functional gastrointestinal disorders and the Rome II process. Gut. 1999; (45 Suppl 2): II1-5.
- Bharucha AE, Wald A, Enck P, Rao S: Functional anorectal disorders. Gastroenterology. 2006; 130: 1510-8.
- American College of Gastroenterology Chronic Constipation Task Force (2005) An evidence-based approach to the management of chronic constipation in North America. Am J Gastroenterol. 2005; 100(Suppl 1): S1-S4.
- Varma MG, Hart SL, Brown JS, Creasman JM, Van Den Eeden SK, Thom DH: Obstructive defecation in middle-aged women. Dig Dis Sci. 2008; 53: 2702-9.
- Soligo M, Salvatore S, Emmanuel AV, De Ponti E, Zoccatelli M, Cortese M, et al.: Patterns of constipation in urogynecology: clinical importance and pathophysiologic insights. Am J Obstet Gynecol. 2006; 195: 50-5.
- Kistner M: Dysfunctional elimination behaviors and associated complications in school-age children. J Sch Nurs. 2009; 25: 108-16.
- Chase JW, Homsy Y, Siggaard C, Sit F, Bower WF: Functional constipation in children. J Urol. 2004; 171: 2641-3.
- Loening-Baucke V: Urinary incontinence and urinary tract infection and their resolution with treatment of chronic constipation of childhood. Pediatrics. 1997; 100: 228-32.
- McGrath KH, Caldwell PH, Jones MP: The frequency of constipation in children with nocturnal enuresis: a comparison with parental reporting. J Paediatr Child Health. 2008; 44: 19-27.
- Bael AM, Benninga MA, Lax H, Bachmann H, Janhsen E, De Jong TP, et al.: Functional urinary and fecal incontinence in neurologically normal children: symptoms of one ‘functional elimination disorder’? BJU Int. 2007; 99: 407-12.
- Koff SA, Wagner TT, Jayanthi VR: The relationship among dysfunctional elimination syndromes, primary vesicoureteral reflux and urinary tract infections in children. J Urol. 1998; 160: 1019-22.
- Loening-Baucke V: Prevalence rates for constipation and faecal and urinary incontinence. Arch Dis Child. 2007; 92: 486-9.
- Kajiwara M, Kato M, Mutaguchi K, Usui T: Overactive bladder in children should be strictly differentiated from monosymptomatic nocturnal enuresis. Urol Int. 2008; 80: 57-61.
- De Paepe H, Renson C, Van Laecke E, Raes A, Vande Walle J, Hoebeke P: Pelvic-floor therapy and toilet training in young children with dysfunctional voiding and obstipation. BJU Int. 2000; 85: 889-93.
- Robson WL, Leung AK, Van Howe R: Primary and secondary nocturnal enuresis: similarities in presentation. Pediatrics. 2005; 115: 956-9.
- Kasirga E, Akil I, Yilmaz O, Polat M, Gözmen S, Egemen A: Evaluation of voiding dysfunctions in children with chronic functional constipation. Turk J Pediatr. 2006; 48: 340-3.
- Erickson BA, Austin JC, Cooper CS, Boyt MA: Polyethylene glycol 3350 for constipation in children with dysfunctional elimination. J Urol. 2003; 170: 1518-20.
- Lucanto C, Bauer SB, Hyman PE, Flores AF, Di Lorenzo C: Function of hollow viscera in children with constipation and voiding difficulties. Dig Dis Sci. 2000; 45: 1274-80.
- Chrzan R, Klijn AJ, Vijverberg MA, Sikkel F, de Jong TP: Colonic washout enemas for persistent constipation in children with recurrent urinary tract infections based on dysfunctional voiding. Urology. 2008; 71: 607-10.
- Ewings P, Spencer S, Marsh H, O’Sullivan M: Obstetric risk factors for urinary incontinence and preventative pelvic floor exercises: cohort study and nested randomized controlled trial. J Obstet Gynaecol. 2005; 25: 558-64. Erratum in: J Obstet Gynaecol. 2005; 25: 834-5.
- Ng SC, Chen YC, Lin LY, Chen GD: Anorectal dysfunction in women with urinary incontinence or lower urinary tract symptoms. Int J Gynaecol Obstet. 2002; 77: 139-45.
- Spence-Jones C, Kamm MA, Henry MM, Hudson CN: Bowel dysfunction: a pathogenic factor in uterovaginal prolapse and urinary stress incontinence. Br J Obstet Gynaecol. 1994; 101: 147-52.
- Faaborg PM, Christensen P, Finnerup N, Laurberg S, Krogh K: The pattern of colorectal dysfunction changes with time since spinal cord injury. Spinal Cord. 2008; 46: 234-8.
- Pannek J, Göcking K, Bersch U: ‘Neurogenic’ urinary tract dysfunction: don’t overlook the bowel!. Spinal Cord. 2009; 47: 93-4.
- Karatzoglou P, Karagiannidis A, Kountouras J, Christofiridis CV, Karavalaki M, Zavos C, et al.: Von Recklinghausen’s disease associated with malignant peripheral nerve sheath thmor presenting with constipation and urinary retention: a case report and review of the literature. Anticancer Res. 2008; 28: 3107-13.
- Gividen J, Van Savage JG: Improvement in neurogenic bladder after the antegrade continence enema procedure. Urology. 2002; 59: 137.
- Milne HJ: An unusual cause of constipation presenting to the emergency department. Eur J Emerg Med. 2006; 13: 119-21.
- Merenda L, Brown JP: Bladder and bowel management for the child with spinal cord dysfunction. J Spinal Cord Med. 2004; 27(Suppl 1): S16-23.
- Wyndaele JJ, Kovindha A, Madersbacher H, et al.: Neurologic Urinary and Faecal Incontinence. In: Abrams P, Cardozo L, Khoury S, Wein A (ed.), Incontinence. Paris, Health Publication Ltd. 2009; Committee 10, pp. 797.
- O’Regan S, Yazbeck S, Hamberger B, Schick E: Constipation a commonly unrecognized cause of enuresis. Am J Dis Child. 1986; 140: 260-1.
- Irvine EJ, Ferrazzi S, Pare P, Thompson WG, Rance L: Health-related quality of life in functional GI disorders: focus on constipation and resource utilization. Am J Gastroenterol. 2002; 97: 1986-93.
- Koelbl H, Nitti V, Baessler K, et al.: Pathophysiology of Urinary Incontinence, Faecal Incontinence and Pelvic Organ Prolapse. In: Abrams P, Cardozo L, Khoury S, Wein A (ed.), Incontinence. Paris, Health Publication Ltd. 2009; Committee 4, pp. 283.
- Norton C, Whitehead W, Bliss DZ, et al.: Conservative and Pharmacological Management of Faecal Incontinence in Adults. In: Abrams P, Cardozo L, Khoury S, Wein A (ed.), Incontinence. Paris, Health Publication Ltd. 2009; Committee 16, pp. 1333.
____________________
Accepted after revision:
June 7, 2010
_______________________
Correspondence address:
Dr. Márcio Augusto Averbeck
Rua Soledade, 569 Bairro Três Figueiras
Porto Alegre, RS, 90470-340, Brazil
Fax: + 55 51 3378-9996
E-mail: marcioaverbeck@gmail.com