INVASIVE
BLADDER CANCER IN THE EIGHTIES: TRANSURETHRAL RESECTION OR CYSTECTOMY?
(
Download pdf )
Clinical Urology
Vol. 37 (1):
49-56, January - February, 2011
doi: 10.1590/S1677-55382011000100007
OSCAR RODRIGUEZ FABA, JOAN PALOU, GUILLERMO URDANETA, LUIS GAUSA, HUMBERTO VILLAVICENCIO
Department of Urology, Fundacio Puigvert, Universitat Autonoma de Barcelona, Barcelona, Spain
ABSTRACT
Purpose:
Describe morbidity and survival in patients older than 80 years with muscle
invasive bladder cancer (MIBC) treated with radical cystectomy (RC) or
transurethral resection (TUR) in our institution.
Materials and Methods: We reviewed our database
of all patients older than 80 years treated with RC and TUR for MIBC between
1993 and 2005 in our institution. Twenty-seven patients were submitted
to RC, with mean age of 82 years and mean follow-up of 16.4 months. RC
was carried out following diagnosis of previous MIBC in 14 cases (51.9%).
The American Society of Anesthesiology (ASA) score was III or IV in 23
patients (85.1%). Seventy-two patients with a mean age of 84 years and
mean follow-up of 33 months, diagnosed with MIBC, were managed by means
of TUR. The ASA score was III-IV in 64 (88.8%) patients.
Results: Pathological stage of the RC specimen
was pT3 in 18 cases (66.7%). Mean hospital stay was 16 days. Early complications
were assessed in 8 patients (29.6%), with an overall survival (OS) of
42.94%, and cancer-specific survival (CSS) of 60.54%. In patients submitted
to TUR, clinical stage was T2 in 36 cases (50%). The mean hospital stay
was 7 days, with a readmission rate (RR) of 87.5%. OS and CSS was less
than 20%.
Conclusions: RC in octogenarian patients
is a safe procedure, with complication and survival rates comparable to
RC series in general population. Transurethral resection (TUR) for patients
with MIBC within this age range is a much less morbid procedure, but disease
specific survival is lower.
Key
words:urinary bladder neoplasms; cystectomy; endoscopy; aged
Int Braz J Urol. 2011; 37: 49-56
INTRODUCTION
The
increased incidence and prevalence of genitourinary neoplasias over the
last few decades can be attributed to demographic evolution and increased
life expectancy. The National Cancer Institute has estimated that 89%
of the bladder tumors are found in patients older than 55, and that the
mean age at diagnosis, is 73 years(1).
Standard treatment for muscle invasive bladder
cancer (MIBC) is radical cystectomy with bilateral pelvic lymphadenectomy,
and is justified in patients with life expectancy greater than two years.
In patients more than 80 years old radical
surgery tends to be avoided, since is believed to be associated with increased
morbidity and mortality rates. Historically those patients have been treated
with TUR that is a less aggressive procedure. It is now accepted that
the American Society of Anesthesiology (ASA) score for patients undergoing
a major procedure is a predictive factor for morbidity and mortality which
is more significant than age alone (2). For the last seven years we have
actively performed radical cystectomy (RC) in patients of advanced age
with an ASA score compatible with this type of surgery.
MATERIALS AND METHODS
We reviewed our database of all patients that were treated with either RC or TUR between 1993 and 2005 for invasive bladder cancer and age over 80 that did not receive neoadjuvant or adjuvant therapy.
Radical Surgery
Twenty-seven
patients over 80 years with MIBC were submitted to RC and urinary diversion
at our institution between 1993 and 2005. Twenty-two (81.5%) were males
and 5 (18.5%) females with mean age 82 ± 3 years (range 80 - 91
years). Inclusion criteria for the patients were detailed medical history,
a physical examination, cardiovascular and pulmonary parameters including
their metabolic and nutritional status. Indications of RC were based on
finding MIBC in TUR, or recurrent high-grade superficial tumors unresponsive
to Bacillus Calmette-Guerin (BCG) therapy. Before surgery all patients
were staged according to the ASA score (3).
Following surgery patients were monitored
at the post-operative care unit during 24 hours. Ureteral catheters were
removed 7-10 days following cystectomy.
Transurethral Resection
A
total of 72 patients (59 males and 13 females) over 80 years old were
staged for MIBC and suitable for TUR. All cases were staged with bimanual
examination under anesthesia and underwent TUR (complete or palliative).
Multiple random biopsies were taken to document presence of carcinoma
in situ. Follow-up consisted of cystoscopy and TUR if recurrence and/or
progression occurred. During follow-up, the numbers of re-admittance and
health state of the patients were considered to evaluate the progression
of the disease.
Peri-operative mortality was defined as
all-cause death up to 30 days after surgery. The overall mortality rate
included cancer-related or cancer-unrelated deaths. The morbidity rate
included early complications considered adverse effects in the course
of hospitalization or 30 days post-surgery and late complications longer
than 30 days post-surgery.
RESULTS
Cystectomy
Pathology
of radical cystectomy (RC) revealed urothelial carcinoma in 26 of the
27 patients (96.3%). Stage was pT3 in 18 cases (66.7%) and association
with prostate carcinoma was found in 10 cases (37%) (Table-1).
Urinary diversion was ileal conduit in 24 (88.8%) patients, cutaneous
diversion in two patients (7.40%) and Studer orthotopic substitution in
one patient (3.80%).
Concomitant cardiovascular disease was the
most frequent co-morbidity, with hypertension in 10 patients (37%), previous
acute myocardial infarction in 3 patients (11.1%) and arrhythmia in 2
patients (7.4%). Other concomitant pathologies were diabetes mellitus
in 4 patients (14.8%), bronchial asthma in 1 patient (3.7%) and emphysema
in 3 patients (11.1%).
Intra- or post-operative blood transfusion
was necessary in 10 patients (37%); furthermore there were two cases (7.4%)
of intraoperative mortality. Early complications occurred in 8 patients
(29.6%) and were paralytic ileus in 4 patients, wound infection in 3,
intra-abdominal abscess in 1 patient and entero-cutaneous fistula in another
one. The major complications were: acute myocardial infarction in one
patient and another patient require re-operation due to bleeding.
The mean hospital stay was 16 days (8-28)
and the mean follow-up of these patients was 16.4 months (1.4-84.2 months).
Distant disease was found in 8 patients
during follow-up: four of those diseases involved lymph nodes and 4 were
multiple.
Overall survival (OS) was 42.94% and cancer
specific survival (CSS) 60.54 % (Table-2, Figure-1).
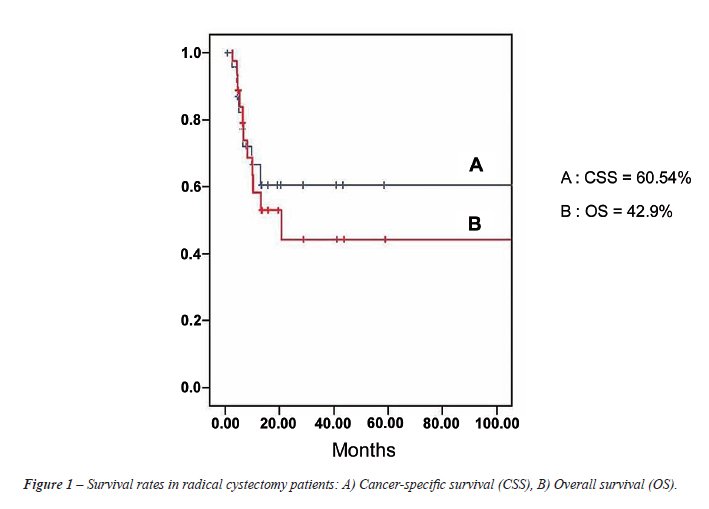
Transurethral Resection
In
patients submitted to TUR, the stage was cT2 in 36 cases (50%), cT3 in
10 cases (13.9%), cT2-T3 in 24 cases (33.3%), and cT4 in 2 cases (2.8%).
Grade was G3 in 49 cases (68%). Forty-nine patients (68%) had a complete
TUR, whereas in 32% resection was incomplete (Table-1).
Intra- or post-operative blood transfusion
was necessary in 10 patients (13.8%), and there was no case of intra-operative
death. Regarding early complications, hemostatic intervention was required
in 6 patients (8.3%), and 2 patients showed manifestations of hemodynamic
angina that required intensive care. The mean hospital stay was 7 days;
with a readmission rate of 87.5% (thirty patients had 1 readmission, 11
patients had 2 readmissions and 11 patients had 3 or more readmissions).
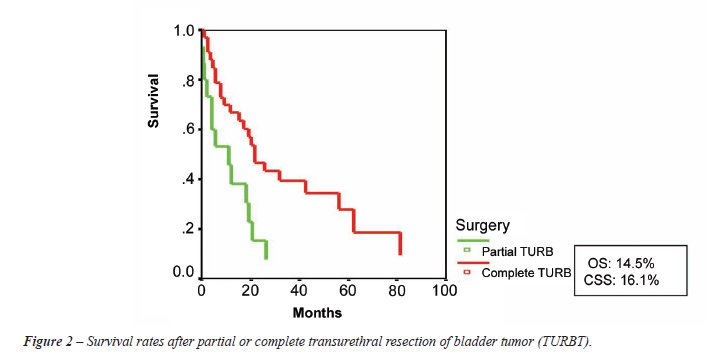
The mean follow-up was 19 months with an overall and CSS of less than
20% (Table-2, Figure-2).
At the end of the follow-up, 8 patients
(11%) were alive, 47 (65%) had died due to cancer, 7 (9.7%) had died due
to other causes, and 7 (9.7%) were lost to follow-up.
COMMENTS
In
the past, advanced age was a contraindication for cystectomy; some studies
reported peri-operative mortality rates of 5.5% in patients younger than
60, versus 11% in patients between 60 and 70 years old (4). Improvements
in the surgical technique, anesthetic management and post-operative care
have brought a reduction of major complications from an initial 51% down
to the current 10-30%, and the mortality rate subsequent to surgery has
decreased to 2% (5), with transfusion, hospital stay, early and late complications
and survival rates comparable to those of patients younger than 65 years.
Moreover, patients presenting with an ASA score compatible with a major
intervention are eligible for cystectomy because when it is compatible
with major procedures, it reflects the functional status of a patient
more accurately than age itself (2,3).
Fifteen years ago, at our institution we
only performed TUR. Later we started doing RC throughout the eighties,
with two main objectives: improve local control disease with better oncological
outcomes and minimize complications.
Regarding local control disease, the proportion
of patients with advanced pathological stage in our series was the highest
one of all the series reviewed (81.48%) (6-8); supporting the RC indication,
since application of conservative alternatives (TUR) would yield a much
poorer tumor control. Moreover, our 42.94% OS rate is similar to pT3 series
published in younger population (9,10) and the difference in elderly patient
data, is because of a shorter follow-up. As to the CSS rate we obtained
60.54% and observed important differences at each stage. If we compare
patients with pathologic stage pT2 to the rest of grouped stages, at our
follow-up period, all of the pT2 patients continue to be alive, whereas
survival of the rest of groups was 55.48%. Most series reviewed report
CSS rates between 62% and 84% (11-14) and no significant differences regarding
OS or CSS were found in the series reviewed between patients younger and
older than 70 years for RC (15,16).
Comparing these results with transurethral
resection of bladder tumor (TURBT) for MIBC, good results are shown in
case of small T2 tumors (17,18). Our survival rate is below 20%, but we
are dealing with not-selected patients with large tumor volumes (32% of
them received only palliative TUR). At the end of the follow-up, only
8 patients (11%) were alive and the OS rate was lower than 20% independently
of the TUR being complete or partial (Figure-2). Therefore, compared to
RC for this age group and with a similar follow-up, even if it is not
a prospective and randomized study; overall and cancer-specific survivals
are much more favorable for RC.
Regarding complications, intra-operative
mortality in our series show two cases (7.40%), whereas most studies reviewed,
show rates between 0% and 7.40%. The published series comparing intra
operative mortality among patients younger and older than 70 shown no
significant differences between both groups (15). Therefore, peri-operative
mortality in the published RC series, some of them with 30 years of follow-up
and with 1,359 patients with a mean 67 years of age, was only 2% (19);
in this period the primary causes of mortality were those due to cardiovascular
decompensation, sepsis frequently related to urinary or bowel fistula,
pulmonary embolism and massive postoperative hemorrhage. In case of TUR
we do not have any cases of intraoperative or perioperative mortality.
The most frequent intraoperative complications were hemorrhage that was
responsible for re-intervention in 84% of cases, perforation in 1.3% with
incidence that is variable in the various series consulted (2.5-5%) (20)
and TUR syndrome.
Ten patients (37%) required either intra-
or post-operative blood transfusion, and the mean of transfused units
was two (1-3). If differences between the mean units transfused and bleeding
in patients younger and older than 70 are compared, significant differences
between both groups regarding the mean bleeding in mL and in the number
of transfused patients are found, even though transfused patients are
larger in number in the older-than-70 group (9). In case of our TUR series,
transfusion was necessary in 10 patients (13.8%) that is lower compared
with the RC group, but higher if it is compared with our global transfusion
rate in TUR that is 3.4% (21).
The mean hospitalization stay of our patients
in the group of RC was 16 days (range 8-28). Hospital stay varies between
7-34 days, and in our experience prolongation of hospital stay in patients
older than 80 is related with the more difficult solution of their major
complications. Moreover, patients with a poor ASA score will potentially
be at greater risk of urinary derivation-related post-operative fistulae
(2). In our series, the only patient that developed an entero-cutaneous
fistula in the postoperative period had an ASA score of III.
TUR group reflect a mean hospitalization
stay of seven days that is much better than the RC group, related to the
lower impact of the endoscopic surgery for the patient. The problem with
this group is a readmission rate that was 87%, related in most cases with
hematuria in the context of tumor persistence.
The evaluation of the risk-benefit ratio
of the radio-chemotheraphy protocols in this cohort of patients over 80
with co-morbidities avoided their use. Available meta-analysis of randomized
trials on cisplatin-containing combination neoadjuvant chemotherapy revealed
a 5% difference in favor of neoadjuvant chemotherapy, and no randomized
trials have yet compared survival with TURBT alone versus cystectomy for
the management of patients with muscle-invasive disease, moreover collaborative
international adjuvant chemotherapy trials are needed to assist researchers
in assessing the true value of adjuvant chemotherapy (22).
Limitation of this study is that it was
a descriptive, and not a comparative analysis of two independent series
of patients. Further prospective randomized trials are necessary to confirm
these findings.
CONCLUSIONS
RC
in octogenarian patients is a safe procedure, with complication and survival
rates comparable to those of the series of patients younger than 80, and
therefore we consider that age is not a contraindication of surgery if
it is not accompanied by an unfavorable ASA score.
TUR for patients with MIBC within this age
range is a much less morbid procedure, but disease specific survival is
lower.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Ries LAG, Melbert D, Krapcho M, Stinchcomb DG, Howlader N, Horner MJ, Mariotto A, Miller BA, Feuer EJ, Altekruse SF, Lewis DR, Clegg L, Eisner MP, Reichman M, Edwards BK (Ed.), SEER Cancer Statistics Review, 1975-2005, National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/csr/1975_2005/, based on November 2007 SEER data submission, posted to the SEER web site, 2008.
- Malavaud B, Vaessen C, Mouzin M, Rischmann P, Sarramon J, Schulman C: Complications for radical cystectomy. Impact of the American Society of Anesthesiologists score. Eur Urol. 2001; 39: 79-84.
- Wolters U, Wolf T, Stützer H, Schröder T: ASA classification and perioperative variables as predictors of postoperative outcome. Br J Anaesth. 1996; 77: 217-22.
- Zincke H: Cystectomy and urinary diversion in patients eighty years old or older. Urology. 1982; 19: 139-42.
- George L, Bladou F, Bardou VJ, Gravis G, Tallet A, Alzieu C, et al.: Clinical outcome in patients with locally advanced bladder carcinoma treated with conservative multimodality therapy. Urology. 2004; 64: 488-93.
- Soulié M, Straub M, Gamé X, Seguin P, De Petriconi R, Plante P, et al.: A multicenter study of the morbidity of radical cystectomy in select elderly patients with bladder cancer. J Urol. 2002; 167: 1325-8.
- Chang SS, Alberts G, Cookson MS, Smith JA Jr: Radical cystectomy is safe in elderly patients at high risk. J Urol. 2001; 166: 938-41.
- Clark PE, Stein JP, Groshen SG, Cai J, Miranda G, Lieskovsky G, et al.: Radical cystectomy in the elderly: comparison of clincal outcomes between younger and older patients. Cancer. 2005; 104: 36-43.
- Kulovac B, Aganovic D, Prcic A: Radical cystectomy early postoperative complications and mortality rate. Med Arh. 2005; 59: 358-9.
- Soloway MS, Lopez AE, Patel J, Lu Y: Results of radical cystectomy for transitional cell carcinoma of the bladder and the effect of chemotherapy. Cancer. 1994; 73: 1926-31.
- Gamé X, Soulié M, Seguin P, Vazzoler N, Tollon C, Pontonnier F, et al.: Radical cystectomy in patients older than 75 years: assessment of morbidity and mortality. Eur Urol. 2001; 39: 525-9.
- Stroumbakis N, Herr HW, Cookson MS, Fair WR: Radical cystectomy in the octogenarian. J Urol. 1997; 158: 2113-7.
- Ogawa A, Yanagisawa Y, Nakamoto T, Wajiki M, Hirabayashi N, Nakama M: Treatment of bladder carcinoma in patients more than 80 years old. J Urol. 1985; 134: 889-91.
- Lodde M, Palermo S, Comploj E, Signorello D, Mian C, Lusuardi L, et al.: Four years experience in bladder preserving management for muscle invasive bladder cancer. Eur Urol. 2005; 47: 773-8; discussion 778-9.
- Deliveliotis C, Papatsoris A, Chrisofos M, Dellis A, Liakouras C, Skolarikos A: Urinary diversion in high-risk elderly patients: modified cutaneous ureterostomy or ileal conduit? Urology. 2005; 66: 299-304.
- May M, Fuhrer S, Braun KP, Brookman-Amissah S, Richter W, Hoschke B, et al.: Results from three municipal hospitals regarding radical cystectomy on elderly patients. Int Braz J Urol. 2007; 33: 764-73; discussion 774-6.
- Solsona E, Iborra I, Ricós JV, Monrós JL, Dumont R: Feasibility of transurethral resection for muscle-infiltrating carcinoma of the bladder: prospective study. J Urol. 1992; 147: 1513-5.
- Herr HW: Transurethral resection of muscle-invasive bladder cancer: 10-year outcome. J Clin Oncol. 2001; 19: 89-93.
- Quek ML, Stein JP, Daneshmand S, Miranda G, Thangathurai D, Roffey P, et al.: A critical analysis of perioperative mortality from radical cystectomy. J Urol. 2006; 175: 886-9; discussion 889-90.
- Mydlo JH, Weinstein R, Shah S, Solliday M, Macchia RJ: Long-term consequences from bladder perforation and/or violation in the presence of transitional cell carcinoma: results of a small series and a review of the literature. J Urol. 1999; 161: 1128-32.
- Collado A, Chéchile GE, Salvador J, Vicente J: Early complications of endoscopic treatment for superficial bladder tumors. J Urol. 2000; 164: 1529-32.
- Calabrò F, Sternberg CN: Neoadjuvant and adjuvant chemotherapy in muscle-invasive bladder cancer. Eur Urol. 2009; 55: 348-58.
____________________
Accepted after revision:
July 7, 2010
_______________________
Correspondence address:
Dr. Oscar Rodríguez Faba
C/ Cartagena, 340-350
Barcelona, 08025, Spain
Fax: + 34 9 3416-9730
E-mail: orodriguez@fundacio-puigvert.es
EDITORIAL COMMENT
In the present
manuscript, the authors compare the cancer specific outcomes of transurethral
resection (TUR) versus radical cystectomy in octogenarians with muscle
invasive bladder cancer. The authors address an interesting clinical question
in a cohort we have traditionally associated to be at increased risk of
perioperative complications with aggressive surgical intervention. The
authors conclude appropriately that patients underlying (pre-treatment)
co-morbidities (measured using ASA score) is more of a determinant of
surgical risk than age alone. Similarly, the authors conclude that radical
cystectomy offers an improved cancer specific survival (versus TUR) at
the cost of increased perioperative morbidity. I would argue that TUR
alone (without consideration of a bladder sparing type approach using
chemo-radiotherapy or at the very least of adjuvant radiotherapy to the
bladder and pelvic lymph nodes for local/regional cancer control) is not
an oncologic efficacious treatment alternative except in the very rare
case of a patient with a focally muscle invasive bladder tumor. Hence,
the importance of repeat TUR (to ensure complete resection), random bladder
biopsies (to rule out multifocal disease), and exam under anesthesia (to
adequately assess clinical stage) should be considered essential in these
select patients treated by TUR alone. Similarly, careful pathologic review
of the TUR specimen by an experienced genitourinary pathologist is essential
to confirm tumor invasion into the muscularis propria and rule out the
presence of adverse pathological features such as lymphovascular invasion
or micropapillary histology.
In summary, there clearly remains a subset of patients with muscle invasive
bladder cancer for whom cystectomy is not a feasible choice because of
pre-operative co-morbidities or by their refusal to proceed with aggressive
surgical intervention. In these patients, clinicians must tailor their
treatment options based on patient and tumor specific characteristics.
Dr.
Philippe E. Spiess
Department of Interdisciplinary Oncology
Moffitt Cancer Center
University of South Florida
Tampa, Florida, USA
E-mail: Philippe.Spiess@moffitt.org