LAPAROSCOPIC
REMOVAL OF SEMINAL VESICLE CYST WITH ECTOPIC URETERAL INSERTION AND RENAL
REMNANT
(
Download pdf )
GILBERTO BUOGO, HENRIQUE RODRIGUES, PAULO RODRIGUES
Albarran Institute of Urology, Rio de Janeiro, RJ, Brazil
ABSTRACT
Seminal vesicle cysts associated with ectopic ureter and renal agenesis is a rare condition. We report on a 23-year-old man with a history of pelvic discomfort and post-coital testicular pain. The investigation disclosed a left seminal vesicle cyst, and an absent left kidney. The patient was successful submitted to resection of the left seminal vesicle, ureter, and dysplastic renal tissue altogether, through laparoscopic approach. Laparoscopy has shown to be an excellent treatment option for this rare condition.
Key words:
laparoscopy; urinary tract; seminal vesicles; abnormalities
Int Braz J Urol. 2002; 28: 335-7
INTRODUCTION
Seminal
vesicle cysts associated with ectopic ureter and renal agenesis are a
rare condition, with approximately 50 reports published about this theme
(1).
We describe a case of a seminal vesicle
cyst associated with ectopic ureter, and dysplastic renal tissue, treated
through a laparoscopic approach.
CASE REPORT
A
23-year-old man presented with a 2-year complaint of left inguinal discomfort,
and post-coital pain on the left testis. On physical exam, both testes
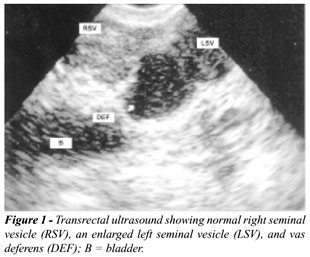
were normal, and a dilated left vas deferens could be palpated. Abdominal
ultrasound revealed absence of the left kidney, and an enlarged left seminal
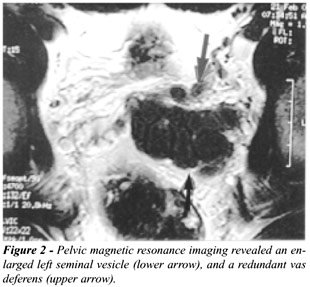
vesicle, which was confirmed by a transrectal ultrasound (Figure-1). Pelvic
magnetic resonance imaging showed absence of the left kidney, and a large
left seminal vesicle with a redundant vas deferens (Figure-2). The patient
was submitted to transperitoneal laparoscopy, with the camera placed at
the umbilicus, and 3 auxiliary ports (11mm at the left lateral border
of the rectus muscle, a 5mm port at its right lateral border, and another
5mm port on the right iliac fossa, allowing anterior traction of the bladder).
The retrovesical peritoneum was opened and the left vas deferens clipped
and divided. The left seminal vesicle was then dissected to the prostate
base, where it was divided. The insertion of the left ureter was at the
lateral aspect of the seminal vesicle. It was isolated and dissected cephalad
after mobilizing the colon. Another 5mm trocar was placed at the midline,
above the umbilicus, because of the very cranial position of the proximal
ureter and remnant kidney. At the usual kidney location, the ureter entered
a dysplastic tissue. This tissue was dissected and removed altogether
with the left ureter and the seminal vesicle (Figure-3). Operative time
was 290 minutes, and estimated blood loss was 180mL. The patient was discharged
home on postoperative day 2. Pathological analysis of the dysplastic kidney
revealed renal parenchyma with fetal characteristics.

DISCUSSION
Congenital
cysts of the seminal vesicles are rare entities, and two-thirds are associated
with renal dysplasia or agenesis, and ectopic ureter. The close relationship
between urinary and reproductive systems embryology responds for this
condition. During the 4th week of pregnancy the ureter arises from the
mesonephric duct and, due to a different growth between the mesonephric
duct and the urogenital sinus, reaches a more cranial position, opening
into the bladder. Seminal vesicles sprout from the distal mesonephric
duct at week 12 of pregnancy. When the ureteral bud originates in a more
cranial site it will not open into the bladder, resulting in an ectopic
ureter, placed in one of the structures originated from the mesonephric
duct (seminal vesicles, ejaculatory duct, or vas deferens). Moreover,
the inadequate stimulation of the metanephrogenic blastema results in
renal agenesis or dysplasia (1-3).
The diagnosis of a seminal vesicle cyst
is generally made in adulthood, and most common symptoms include bladder
irritation, post-coital pain, and hematospermia. Treatment is indicated
for symptomatic cases. Transrectal cyst aspiration and open surgery are
related to recurrence and elevated morbidity, respectively. Recently,
Cherullo et al. (1) reported on 2 seminal vesicle cysts treated successfully
through laparoscopic approach.
In this case, laparoscopy provided an excellent
visualization of the retrovesical space, allowing effective resection
of the seminal vesicle, ureter, and renal remnant, and with minimal blood
loss and low morbidity. We believe that laparoscopic approach is the treatment
of choice for such cases.
__________________________________
Ms. Michelle Pinheiro provided assistance
with manuscript preparation.
REFERENCES
- Cherullo EE, Meraney AM, Bernstein LH, Einstein DM, Thomas AJ, Gill IS: Laparoscopic management of congenital seminal vesicle cysts associated with ipsilateral renal agenesis. J Urol. 2002; 167: 1263-7.
- Carmignani G, Gallucci M, Puppo P, De Stefani S, Simonato A, Maffezini M: Video laparoscopic excision of a seminal vesicle cyst associated with ipsilateral agenesis. J Urol. 1995; 153: 437-9.
- Williams RD, Sandlow JI: Surgery of the Seminal Vesicles. In: Walsh PC, Retik AB, Vaughan Jr ED, Wein AJ (eds.), Campbell’s Urology. Philadelphia, W.B. Saunders, 1998, pp. 3299-3315.
_______________________
Correspondence address:
Dr. Henrique Rodrigues
Rua Djalma Ulrich, 329 / 301
Rio de Janeiro, RJ, 22071-020, Brazil
Fax: + 55 21 2579-2358
E-mail: hcrodrigues@uol.com.br