CHRONIC
PENILE STRANGULATION
(
Download pdf )
ROBERTO I. LOPES, SILVIA I. LOPES, ROBERTO N. LOPES
Women’s Beneficent Society, Syrian and Libyan Hospital, São Paulo, SP, Brazil
ABSTRACT
Chronic
penile strangulation is exceedingly rare with only 5 cases previously
reported. We report an additional case of progressive penile lymphedema
due to chronic intermittent strangulation caused by a rubber band applied
to the penile base for 6 years.
A 49-year-old man presented incapacity to
exteriorize the glans penis. For erotic purposes, he had been using a
rubber-enlarging band placed in the penile base for 6 years. With chronic
use, he noticed that his penis swelled. Physical examination revealed
lymphedema of the penis, phimosis and a stricture in the penile base.
The patient was submitted to circumcision and the lymphedema remained
stable 10 months postoperatively.
Chronic penile incarceration usually causes
penile lymphedema and urinary disturbance. Treatment consists of removal
of foreign devices and surgical treatment of lymphedema.
Key
words: penis; lymphedema; compression; device
Int Braz J Urol. 2003; 29: 327-9
INTRODUCTION
While penile incarceration with foreign bodies is generally acute and common enough to be seen by most urologists throughout their careers, chronic penile strangulation by the same mechanism is exceedingly rare and to our knowledge only 5 cases have been reported in the literature (1-3). We report a case of progressive penile lymphedema due to chronic intermittent strangulation caused by a rubber band.
CASE REPORT
A
49-year-old single white man was admitted to the hospital because of his
incapacity to exteriorize the glans penis. Approximately 6 years prior
to admission, he began to use a rubber-enlarging band, acquired in a sex
shop, in order to enhance sexual experience and to prolong erection. The
rubber-band with 2-cm in diameter was placed in the penile root for approximately
3 hours, 3 to 4 times a week, during the night. With chronic use, he noticed
that his penis swelled and that he was unable to ejaculate, but he could
maintain prolonged erections, usually over 4 hours without any episode
of priapism. He was extremely satisfied with his sexual performance and
genital appearance. Two years after the beginning of the rubber band usage,
he observed progressive penile swelling and an incapability of exteriorizing
his glans penis one year later. However, he only decided to seek medical
assistance after 3 years. He denied previous episodes of urinary infection
and voiding dysfunction.
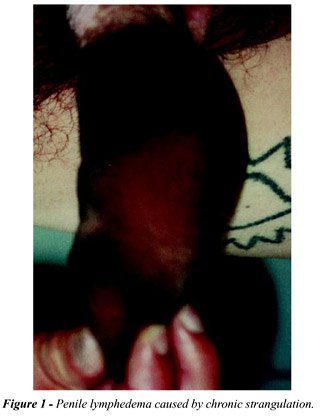
Physical examination revealed lymphedema
of the penis without scrotal involvement (Figure-1). The penis was covered
with dark brown hypertrophic skin and it had a 6.7 cm in diameter. A stricture
could be observed in the penile base corresponding to the place on which
the band was applied. Phimosis was present. No skin ulceration, urethral
injury, loss of sensation or other alterations were noticed. Urinalysis
and urine culture were not suggestive of urinary tract infection.
The patient was advised to stop immediately
the rubber-band usage and a month later, we performed a circumcision.
Cosmetic result was acceptable (Figure-2) and the patient stated he was
well satisfied with function and appearance. Lymphedema remained stable
10 months postoperatively.

COMMENT
Chronic
penile strangulation by foreign bodies may be the result of the impossibility
to remove the object applied to the penis (1,2) or caused by inappropriate
usage of devices developed for autoerotic purposes and to prolong erection
(3) that may be regularly acquired at specialized shops.
Chronic penile incarceration usually led
to penile lymphedema and may also cause voiding dysfunction (1), urinary
infections (1,2), skin ulcerations (1), necrosis (1), urethral cutaneous
fistula (2) and colonization of hypertrophic skin (3). Treatment consists
of removal of foreign devices and/or medical orientations on the correct
usage of erection devices. Surgical treatment of lymphedema may involve
lymphangiectomy with covering of denuded areas with skin flaps or full
and split skin grafts (3), and in some cases, penectomy and circumcision
may be indicated (1,2).
In the present case, we did not indicate
removal of all lymphedematous tissue because the patient was satisfied
with his penile appearance and sexual performance since the onset of penile
lymphedema.
REFERENCES
- Hoffman HA, Colby FT: Incarceration of the penis. J Urol. 1945; 54: 391-9.
- Stuppler SA, Walker JG, Kandzari SJ, Milam DF: Incarceration of penis by a foreign body. Urology 1973; 2: 308-9.
- Tanabe N, Muya M, Isonokami M, Kozuka T, Honda T, Ohtani H: Lymphedema due to chronic penile strangulation: a case report. J Dermatol. 1996; 23: 648-51.
______________________
Received:
March 31, 2003
Accepted after revision: May 16, 2003
_______________________
Correspondence address:
Dr. Roberto Iglesias Lopes
Rua Baronesa de Itu, 721 / 121
São Paulo, SP, 01231-001, Brazil
Fax: + 55 11 3666-8266
E-mail: robertoiglesias@
terra.com.br