STRADDLE
INJURIES TO THE BULBAR URETHRA: MANAGEMENT AND OUTCOME IN 53 PATIENTS
(
Download pdf )
MOHAMMED ABD-ALLA ELGAMMAL
Department of Urology, Assiut University Hospital, Assiut, Egypt
ABSTRACT
Objective: To describe our experience with blunt injuries to the bulbar urethra and their late sequelae to identify factors that may affect patient outcome.Materials and Methods: A retrospective study was performed on 53 male patients who presented, between January 2001 and December 2005, with blunt traumatic injury to the bulbar urethra. The definitive diagnosis of urethral rupture was made by retrograde urethrography, where urethral rupture was classified into partial or complete. The minimum follow-up period was 3 years. The initial management was either suprapubic cystostomy or endoscopic urethral realignment over a urethral catheter using a cystoscope to pass a guide-wire over which the catheter was inserted. Stricture formation was managed by visual internal urethrotomy (VIU) for passable strictures and urethroplasty (stricture excision and re-anastomosis) for impassable strictures or recurrence after VIU. The follow-up period was three years. The results were analyzed by SPSS software (chi-square and Student’s-t-test).
Results: Stricture formation occurred in 19 of 22 patients (86%) with complete urethral rupture and in 10 of 31 (32%) with partial rupture (p < 0.001). Strictures occurred in 11 of 31 (35%) patients treated initially with suprapubic cystostomy and in 18 of 22 (82%) treated with primary urethral realignment (p < 0.001). The success rate after VIU was 15% (4 of 26 patients) and after urethroplasty it was 96% (24 of 25 patients) (p < 0.001).
Conclusions: Suprapubic cystostomy is better than urethral realignment and catheterization as primary management after straddle injury to the bulbar urethra. Stricture excision and re-anastomosis is better than VIU as delayed management for strictures that develop after straddle injury to the bulbar urethra.
Key
words:
urethra; trauma; rupture: management; reconstructive surgical procedures
Int
Braz J Urol. 2009; 35: 450-8
INTRODUCTION
Blunt
or penetrating trauma may cause anterior urethral injuries. Blunt injuries
are more commonly diagnosed, and the bulbar urethra is the most frequently
injured segment (85%) (1) because it is fixed beneath the pubic bone,
unlike the freely mobile pendulous urethra. Blunt injuries to the bulbar
urethra are typically caused by straddle type injuries (e.g., motor vehicle
accidents; bicycle accidents; falling astride onto a fence, railing or
saddle) or kicks to the perineum. The force contacting the perineum crushes
the bulbar urethra against the inferior pubic rami, leading to contusion
or urethral laceration (2).
Management of partial and complete disruptions
after blunt trauma to the bulbar urethra remains controversial. The question
which is highly debated in the literature is whether it is better to divert
the urine by transurethral or suprapubic catheterization after injury
to the anterior urethra (3,4). Another question is whether strictures
that develop after straddle injury to the bulbar urethra are best treated
with surgical repair or endoscopic urethrotomy.
Because only a few small series have been published regarding straddle
injury of the bulbar urethra, we reviewed the urological trauma database
at our department to better define the clinical outcome of these injuries.
MATERIALS AND METHODS
A
retrospective study was carried out on 53 male patients who presented
to our trauma unit between January 2001 and December 2005 with blunt traumatic
injury of the bulbar urethra. No attempts were made to catheterize the
patients in the emergency room. Blood at the meatus was the single most
important clinical diagnostic sign of urethral injury.
The definitive diagnosis of urethral rupture
was made by retrograde urethrography. Complete urethral rupture was diagnosed
on the appearance of extravasation of contrast medium in the area of the
bulbar urethra outside the corpus spongiosum, with no contrast entering
the prostatic urethra or bladder. Partial urethral rupture was diagnosed
on the appearance of contrast extravasation in the area of the bulbar
urethra within the corpus spongiosum, with contrast entering the prostatic
urethra or bladder.
All patients received broad-spectrum antibiotics at induction of anesthesia.
Either suprapubic cystostomy or endoscopic urethral realignment was used
as primary management. In cases of endoscopic urethral realignment, a
cystoscope was used to bypass the ruptured segment by introducing a guide-wire
through its channel to the bladder and then a silicone catheter (F18)
was passed over the guide wire. Under fluoroscopic guidance, contrast
medium was injected into the catheter to verify its position inside the
bladder. Suprapubic catheters were left indwelling for three weeks, then
spigoted, and if patients could urinate freely, they were removed. If
patients could not urinate, re-evaluation of the urethra using ascending
urethrography was done. Urethral catheters after endoscopic realignment
were left in place for two and three weeks in partial and complete injury,
respectively. In cases of complete urethral injury with perineal hematoma
or extravasation, no attempt at urethral realignment was made. All patients
were instructed to return for follow-up routinely every three months in
the first year then every six months thereafter. Retrograde urethrography
was performed if the patient had difficulty urinating, maximum urine flow
rate (Qmax) was less than 10 mL/minute or the postvoiding residual urine
volume (PVR) was > 50 mL on ultrasound. Patients with a passable stricture
were managed by visual internal urethrotomy (VIU) as a trial of less invasive
treatment. Patients with an impassable stricture or failed VIU were managed
by open urethroplasty. Treatment success was defined as no symptoms of
infravesical obstruction, Qmax persistently > 15 mL/second, PVR persistently
< 50 mL and good urethral caliber on ascending urethrography.
Statistical analysis was performed on computer
software (SPSS for Windows; SPSS, Inc, Chicago, IL, USA) using the chi-square
and Student’s- t-test.
RESULTS
Patient Characteristics
The mean patient age was 31 (range 18 to 52 years). The mechanism of injury was a fall astride in 34 (64%) of the patients, a direct kick to the perineal region in 16 (30%) and a motorcar accident in 3 (6%). The main complaint was bleeding per urethra in 39 patients (74%) and inability to urinate in 14 (26%). Perineal and scrotal haematoma was present in 9 patients (17%) while perineal extravasation of urine was present in 3 (6%). Partial urethral disruption was found in 31 patients (58%) and complete urethral disruption in 22 (42%). There were no patients with urethral contusion alone.
Partial Urethral Disruption
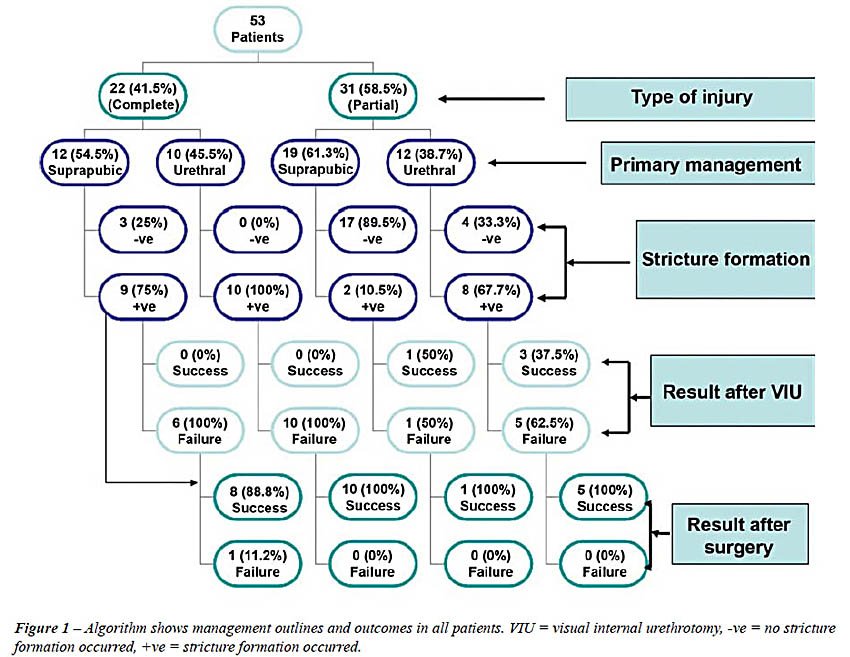
Of the 31 patients with partial urethral rupture, 19 (61%) were treated primarily with suprapubic cystostomy, and stricture formation occurred in 2 (11%) of these patients 2 and 6 months after catheter removal; 12 patients (39%) were treated primarily with urethral realignment, and stricture formation occurred in 8 (67%) 4-12 months (mean = 8 months) after catheter removal. Mean stricture length in patients treated primarily with suprapubic cystostomy was not statistically different from those treated primarily with urethral realignment (1.1 cm range 0.9 to 1.3 cm and 1.3 cm range 1.1 - 1.6 cm respectively (p = 0.65). All 10 patients who developed stricture after partial disruption were treated by VIU, re-stricture developed in 6 (60%) 4-9 months after VIU, and all of these patients were treated successfully with anastomotic urethroplasty (Figure-1).
Complete Urethral Disruption
Of the 22 patients with complete urethral rupture, 12 (55%) were treated primarily with suprapubic cystostomy, stricture formation occurred in 9 patients (75%) while the suprapubic catheter was still in place in 6 patients (67%) or within 6 months of catheter removal in 3 patients (33%); 10 patients (45%) were treated primarily with urethral realignment, and stricture formation occurred in all patients (100%) 4 - 9 months (mean = 6 months) after catheter removal. The duration of stricture formation was not significantly different between partial and complete urethral rupture (p = 0.15). Mean stricture length in patients treated primarily with suprapubic cystostomy was significantly shorter than in those treated primarily with urethral realignment (1.4 cm range 1.2 to 1.5 cm and 1.7 cm range 1.6 to 2.2 cm respectively (p = 0.031). Of the 19 patients who developed a stricture after complete disruption, 16 (84%) had a passable stricture and were treated by VIU; re-stricture developed in all these patients 2-6 months after the procedure. All 16 patients with recurrent stricture after VIU and 3 patients with impassable stricture after injury were treated with anastomotic urethroplasty, and only one of these 19 patients (5%) required a repeat urethroplasty for recurrent stricture (Figure-1). The incidence of stricture formation after complete urethral disruption was significantly higher than after partial disruption (Table-1).
Primary Management
Patient characteristics were analyzed in relation to primary management (Table-2). There were no significant differences with regard to patients characteristics between those treated primarily with suprapubic cystostomy and those treated with primary urethral catheterization (Table-2). In the group of 31 patients (58%) primarily treated with suprapubic cystostomy, stricture formation occurred in 11 (36%), whereas in the 22 (42%) treated, with primary urethral catheterization, stricture formation occurred in 18 (82%). The incidence of stricture formation after primary urethral catheterization was significantly higher than after suprapubic cystostomy (Table-1).
Stricture Management
In the group of 26 patients treated with VIU, 4 (13%) had a successful outcome after 3 years follow-up. In the group of 25 patients treated with anastomotic urethroplasty, 24 (96%) had a successful outcome after 3 years follow-up. The difference between these treatment outcomes was statistically significant (Table-3).
COMMENTS
Management
of partial urethral lacerations typically entails suprapubic urinary diversion
or primary realignment/urethral catheterization for 1 to 2 weeks. Incomplete
lacerations usually heal rapidly and with a low stricture rate. When strictures
do occur, they are typically short or flimsy and can be managed effectively
by VIU (5). In the present study, stricture formation developed in 11%
of patients managed primarily with suprapubic cystostomy and in 67% of
patients who were managed primarily with urethral realignment.
Early reports by Pontes and Pierce stated
that excellent results could be obtained with urinary diversion rather
than realignment (2,4) but Husmann et al. reported that urethral realignment
after surgical repair of the urethra achieved a better outcome (3). However,
the type of trauma in the study by Husmann et al. was penetrating, whereas
in the present study all patients had blunt trauma.
In the recent review of straddle injuries
to the bulbar urethra by Park and McAninch, 47 of 78 patients (60%) presented
6 months to 10 years after the acute injury with obstructive voiding symptoms
or frank urinary retention (6). In the present study stricture formation
developed after 4-12 months (mean = 8 months) in patients with partial
urethral disruption and after 3-9 months (mean = 6 months) in patients
with complete disruption (p = 0.15). The difference between the present
study and the series reported by Park and McAninch is that we calculated
the time to stricture formation only in patients who presented acutely
after urethral injury and excluded patients who presented late after trauma
without previous urinary diversion or urethral realignment.
Extrapolating from the experience with posterior
urethral avulsion injuries, it could be expected that early endoscopic
realignment over a Foley catheter in anterior urethral injury should produce
fewer strictures than suprapubic cystostomy alone. The San Francisco General
Hospital group recently reported its experience with 78 straddle injuries
to the bulbar urethra (6). The primary realignment group more commonly
required urethroplasty than the suprapubic diversion group (100% versus
88%) and, moreover, complex flap or graft urethroplasty was more often
required. In the current study, stricture formation developed in 75% of
patients managed primarily with suprapubic cystostomy and in 100% of patients
who were managed primarily with urethral realignment. Also, the strictures
that developed after suprapubic cystostomy were, on average, significantly
shorter than the strictures that developed after urethral realignment.
It is possible that with early suprapubic
cystostomy for total or partial urethral disruption the extent of the
acute and chronic inflammatory cascade would be limited and the severity
of stricture formation may be mitigated. Moreover, the presence of a catheter
in the area of urethral injury may cause a foreign body reaction, exacerbating
the acute and chronic inflammatory cascade (6). Also, irrigation and manipulation
during endoscopic realignment may cause additional injury to the ruptured
urethra. However, primary realignment by minimally invasive methods has
become a common contemporary management option, for posterior urethral
disruption particularly at high-volume trauma centers in case of posterior
urethral disruptions and the stricture rates are decreased (53% versus
97%) (7,8). This fact is true with regard to posterior urethral disruption,
where the main problems are urethral distraction and misalignment but
in the case of anterior urethral ruptures the urethra is maintained in
alignment as it enclosed inside the corpus spongiosum and strictures that
develop later on are due to subsequent spongiofibrosis.
Endoscopic procedures, such as dilation
or VIU, are seldom curative. The resulting strictures are usually narrower,
shorter, and can be repaired by a perineal approach. The gold standard
treatment is stricture excision with primary re-anastomosis. Several medical
centers report success rates exceeding 95% (9). In the current study the
success rate after VIU was 15%, compared to 96% after excision and re-anastomosis.
The lower success rate of VIU for urethral strictures after straddle injury
may be explained by excessive peri-urethral fibrosis resulting from the
blunt force acting as a hammer crushing the urethra against the anvil
of the pubis.
The limitations of this study are that it is not truly randomized and
longer follow-up is required.
CONCLUSION
Suprapubic cystostomy is associated with a lower stricture rate than urethral catheterization as primary management after straddle injury to the bulbar urethra. Stricture excision and re-anastomosis is associated with a lower recurrence rate than VIU as delayed management for strictures after straddle injury to the bulbar urethra.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Richter ER, Morey AF. Urethral trauma. In: Wessells HB, McAninch JW, (ed.), Urological emergencies. Totowa (NJ). Humana Press. 2005; pp. 57-69.
- Armenakas NA, McAninch JW. Acute anterior urethral injuries: diagnosis and initial management. In: McAninch JW, Jordan GH, Carroll PR (ed.), Traumatic and reconstructive urology. Philadelphia, W.B. Saunders. 1996; pp. 543-50.
- Husmann DA, Boone TB, Wilson WT: Management of low velocity gunshot wounds to the anterior urethra: the role of primary repair versus urinary diversion alone. J Urol. 1993; 150: 70-2.
- Pontes JE, Pierce JM Jr: Anterior urethral injuries: four years of experience at the Detroit General Hospital. J Urol. 1978; 120: 563-4.
- Brandes S: Initial management of anterior and posterior urethral injuries. Urol Clin North Am. 2006; 33: 87-95.
- Park S, McAninch JW: Straddle injuries to the bulbar urethra: management and outcomes in 78 patients. J Urol. 2004; 171: 722-5.
- Elliott DS, Barrett DM: Long-term followup and evaluation of primary realignment of posterior urethral disruptions. J Urol. 1997; 157: 814-6.
- Koraitim MM, Marzouk ME, Atta MA, Orabi SS: Risk factors and mechanism of urethral injury in pelvic fractures. Br J Urol. 1996; 77: 876-80.
- Jordan GH, Virasoro R, Eltahawy EA: Reconstruction and management of posterior urethral and straddle injuries of the urethra. Urol Clin North Am. 2006; 33: 97-109.
____________________
Accepted
after revision:
April 15, 2009
_______________________
Correspondence
address:
Dr. Mohammed Abd-alla Elgammal
Lecturer of Urology
Assiut University Hospital
Assiut, 71526, Egypt
Fax: + 0020 8833-3327
E-mail: mo_elgammal@yahoo.com
EDITORIAL COMMENT
The main
shortcoming of this retrospective, non-randomized study is that it does
not provide information about the factor(s) that determined the choice
of initial management by suprapubic cystostomy or urethral catheterization.
Therefore, unidentified selection biases may explain the results.
Nonetheless, the findings support a number of conclusions that appear
logical and explicable: (1) complete urethral rupture compared with partial
rupture leads to a higher rate of stricture formation, probably because
there has been more damage to the peri-urethral tissues; (2) urethral
re-alignment and catheterization lead to a higher stricture rate than
suprapubic cystostomy, possibly because cystoscopy causes more damage
to the urethra, and infection or inflammation caused by the transurethral
catheter leads to more severe fibrosis; (3) urethral stricture formation
after blunt external trauma usually occurs within 9 months (mean 4 to
8 months) after the injury, similar to recurrences after VIU, where the
majority also occur within 12 months; (4) VIU has a lower success rate
than urethroplasty, no doubt because it does not remove fibrotic tissues,
and may lead to even more spongiofibrosis.
In the Results section the authors state that, in the group of 26 patients
treated with VIU, only 4 (13%) had a successful outcome after 3 years
follow-up. However, 4/26 is 15%, as shown in Table-3. This early stricture
recurrence rate of 85% after VIU is exceptionally high, compared with
the recurrence rates reported in the literature. Importantly, the recurrence
rate was lower (60%) for VIU performed for strictures after partial urethral
rupture, compared with complete rupture (100%), indicating that VIU for
stricture formation after complete urethral rupture is virtually futile.
Dr.
Christiaan F. Heyns
Department of Urology
University of Stellenbosch & Tygerberg Hospital
Tygerberg, South Africa
E-mail: cfh2@sun.ac.za
EDITORIAL COMMENT
This
is a retrospective analysis of a cohort of patients managed for acute
presentation of bulbar urethral straddle injury at a single institution
between 2001 and 2005. The outcomes analyzed were a) rate of development
of stricture after initial management with suprapubic cystostomy tube
(SPT) or endoscopic realignment, and b) success rates after visual internal
urethrotomy (VIU) or primary anastomotic urethroplasty. All patients had
partial or complete disruption of the urethra and were roughly equally
distributed between the two different acute management protocols.
Whereas other authors have discussed success
with SPT vs. endoscopic realignment in posterior urethral disruption injuries,
little is known about how these treatments fare relative to each other
in acute management of straddle injuries to the bulbar urethra. Contrary
to the findings in the posterior urethra, the authors report that whether
the injuries to the bulbar urethra were partial or complete disruptions,
patients managed with SPT had a lower incidence of stricture formation
than those undergoing endoscopic realignment. The authors present possible
reasons for these counterintuitive finding. Certainly, the pathophysiology
of stricture formation in crush injuries to the bulbar urethra is quite
different from that of shear injuries to the posterior membranous urethra.
Perhaps this accounts for the difference in findings. Of note, the results
should be evaluated with some skepticism, as this is a non-randomized
study and by definition subject to selection bias. The author did not
provide any information about the selection criteria in acute management.
Urethral realignment may have been attempted in patients who were older,
had more comorbidities or had more severe injuries.
Following stricture formation, the authors
evaluate the success rates for urethroplasty and VIU. The success rates
for primary anastomotic urethroplasty quoted at 96% are in agreement with
the published literature. It is interesting to note the low success rated
for VIU (15%) for strictures that are less than 2 cm in length. The published
success rates of VIU for bulbar urethral strictures are in the range of
42-73%. The lower rates seen in the current study attests to the great
degree of spongiofibrosis that occurs in the setting of crush injury.
It would be interesting to know whether the initial management (SPT or
realignment) affects the success rates of subsequent stricture treatments
(VIU or urethroplasty). However, such a subset analysis is not possible
in this series due to small numbers.
The author should be congratulated for
their contribution to the published literature on urethral straddle injuries.
Further studies should attempt to address similar questions in a randomized
setting.
Dr.
Bahaa Malaeb &
Dr. Sean P. Elliott
Department of Urology Surgery
University of Minnesota
Minneapolis, Minnesota, USA
E-mail: selliott@umn.edu
EDITORIAL COMMENT
The
primary responsibilities of the urologist when encountering a patient
with an acute anterior urethral injury are 1) to diagnose the extent of
the injury and 2) to divert the urine away from the injury if appropriate,
whether it is with urethral catheterization or suprapubic diversion (1).
Many times, the initial evaluation includes cystourethroscopy, which serves
to both visualize the injury and to then aid in urethral catheterization,
usually over a cystoscopically placed wire. Conventional wisdom would
say that having a catheter across a urethral injury would augment appropriate
urethral healing and subsequently decrease urethral stricture rates. This
is why, for example, a catheter is nearly universally placed after radical
retropubic prostatectomy or urethral reconstructive surgery. However,
the superiority of suprapubic tube placement over urethral catheterization,
reported by Abd-alla Elgammal in this manuscript, challenges that notion.
As discussed in the manuscript, this finding
has been reported before. Park et al. analyzed a series of anterior urethral
injuries from San Francisco General Hospital, and found that while strictures
requiring intervention were high regardless of initial management (88%
for suprapubic diversion v 100% for urethral catheterization, p = 0.37),
the group that initially had suprapubic diversion without urethral manipulation
were less likely to require complex reconstruction (2). The authors in
the current study report similar findings. Patients with complete anterior
urethral disruption managed with a urethral catheter had a 100% stricture
rate versus a 75% stricture rate with suprapubic management. In partial
disruptions, the results were even more dramatic, with strictures developing
in 68% of men managed with urethral catheterization versus only 11% in
men with suprapubic tubes.
What is the mechanism for the differences
found in this study? If the reported outcomes are to be believed, a multi-factorial
explanation is most plausible. As suggested in the manuscript, it is possible
that the initial cystoscopic exam with subsequent urethral catheterization
could propagate the original injury. The catheter, being a foreign body,
could also worsen the periurethral inflammatory reaction and hence, scar
formation (3). Finally, when a urethral catheter is in place, it serves
to stent open the bladder neck, which can allow for leakage of urine around
the catheter, further urinary extravasation through the urethral injury,
and again, a worse periurethral inflammatory reaction.
So should all anterior urethral injuries
be managed with suprapubic tube alone? Unfortunately, without a controlled,
randomized study this question cannot be completely answered. However,
the findings from this study should make all urologists question the need
for heroic attempts at endoscopic realignment of an anterior urethral
injury, as outcomes in terms of future stricture rates are at least similar
and at worst, much higher, when placing a urethral catheter than when
simply placing a suprapubic tube.
REFERENCES
1. Chapple
C, Barbagli G, Jordan G, Mundy AR, Rodrigues-Netto N, Pansadoro V, et
al.: Consensus statement on urethral trauma. BJU Int. 2004; 93: 1195-202.
2. Park S, McAninch JW: Straddle injuries to the bulbar urethra: management
and outcomes in 78 patients. J Urol. 2004; 171: 722-5.
3. Talja M, Korpela A, Järvi K: Comparison of urethral reaction to
full silicone, hydrogen-coated and siliconised latex catheters. Br J Urol.
1990; 66: 652-7.
Dr.
Bradley A. Erickson &
Dr. Christopher M. Gonzalez
Department of Urology
Feinberg School of Medicine
Northwestern University
Chicago, Illinois, USA
E-mail: j-meeks@md.northwestern.edu