ANALYSIS
OF RHYTHMIC RECTAL CONTRACTIONS DURING FILLING CYSTOMETRY IN WOMEN
(
Download pdf )
FRANÇOISE A. VALENTINI, BRIGITTE G. MARTI, GILBERTE ROBAIN, PIERRE P. NELSON
UMRS 731 (FAV, GR), INSERM / Université Pierre et Marie Curie (Université Paris 6), Paris, France and Service de Médecine Physique et Réadaptation (FAV, BGM, GR, PPN), Hôpital Charles Foix, Ivry-sur-Seine, France
ABSTRACT
Purpose:
Rhythmic or random rectal contractions independent of bladder activity
are frequently observed during cystometry and usually attributed either
to a neurological disease, or to ageing. The aim of our study was to search
for an association of rhythmic rectal contractions (RRCs) with a specific
lower urinary tract symptom or/and an urodynamic diagnosis.
Materials and Methods: The population consisted
of 534 consecutive women with lower urinary tract symptoms and without
specific gastro-intestinal disease referred for urodynamics; 382 (non-ND)
had no history of neurological disease and 152 (ND) a history of neurological
disease. Cystometries were performed according to ICS recommendations.
Rectal pressure was measured using a punctured balloon filled with 2 mL
of saline. RRCs were defined as rhythmic changes in the rectal pressure
of at least 3 cm H2O independent of the total vesical pressure.
Results: RRCs were observed in 69 patients,
with no difference in neurological status or age (non-ND: 12.3% and 65.5y;
ND: 14.5% and 62.7y). Patients with RRCs were significantly older than
the negative population (p = 0.0002). RRCs had a low frequency: 1 - 4/min;
their amplitude was = 15 cm H2O in 67 patients. RRCs were associated with
urgency (35 patients) whatever the neurological status and with detrusor
overactivity only in the neurological patients.
Conclusions: RRCs cannot be considered
as artefactual events during cystometry in women, occur in the older population,
are frequently associated with urgency but not with detrusor overactivity
or neurological disease. Occurrence of RRCs should prompt the physician
to look at the possible causes of urgency (colonic or bladder).
Key
words: urodynamics; rectum; urinary tract diseases; women
Int Braz J Urol. 2009; 35: 475-83
INTRODUCTION
Rhythmic
or random rectal contractions, independent of bladder activity are frequently
observed during filling cystometries. Usually they are attributed either
to a neurological disease (1), or to ageing (2). Recently, it has been
found that rectal contractions occur more frequently in males with benign
prostatic hyperplasia and detrusor overactivity (3). Spontaneous motor
activity of the rectum (isolated contraction or sequences of contractions)
has been observed and well described during prolonged manometric recordings
in both symptomatic and asymptomatic patients (4,5).
The aim of this retrospective study was to review consecutive multichannel
urodynamic recordings of women with demonstrated rhythmic rectal contractions
(RRCs) in order to determine if there is an association with a specific
lower urinary tract symptom (LUTS) and/or a urodynamic finding.
MATERIALS AND METHODS
The population
consisted of 534 consecutive women with LUTS referred for urodynamics
in our laboratory between January 2005 and December 2006. Investigated
LUTS were storage (stress, urge and mixed incontinence; increased daytime
frequency and nocturia) and voiding symptoms.
The population was divided in two sub-groups: 382 patients without a history
of neurological disease (non-ND) and 152 with a history of neurological
disease (ND), such as stroke, multiple sclerosis, lumbar disc injury,
etc. Exclusion criteria were complete spinal cord injury (because the
specific physiopathology), inflammatory bowel disease, previous colorectal
surgery, rectocele and isolated lower urinary tract pain.
Digital rectal examination allowed to verify that the rectal ampulla was
empty. Urodynamics were performed using the Bonito® unit (Laborie
Medical Technologies, Paris, France) Filling cystometry was performed
at the medium filling rate of 50 mL/min (normal saline at room temperature)
until maximum bladder capacity in a sitting position. Vesical and urethral
pressures were recorded using a triple lumen catheter 10F. Rectal pressure
was measured using a punctured balloon filled with 2 mL of saline solution
at room temperature in order to avoid pressure artifacts; the balloon
was inserted at 5 cm of the anal verge. Detrusor pressure was the difference
between vesical minus rectal pressure. Pressure transducers were zeroed
according with the ICS recommendations (6). Rectal catheter was first
inserted and after 2-3 min, then the urethral catheter was inserted. Recordings
began about 5 minutes after the insertion. Transmission of pressures was
verified by asking the patient to cough before and after the beginning
of filling.
Significant RRCs were defined as rhythmic changes in the rectal pressure
of at least 3 cm H2O independent of the total vesical pressure and independent
of respiratory movements.
Occurrence of RRCs was analyzed according to age, neurological history,
duration during filling, main complaint and urodynamic diagnosis. Special
attention was given to symptoms of urgency (with or without incontinence
- overactive bladder - OAB) evaluated from bladder diary and general interrogation,
and to detrusor overactivity (uninhibited detrusor contractions - DO)
during cystometry (7).
Each study was reviewed independently by two investigators (F.V. and B.M.);
to be retained, the study needed to be considered univocally positive
by both researchers.
For statistical analysis we used Student’s-t-test and chi-square
test with p < 0.05 considered to indicate significance.
RESULTS
Among
the 534 patients (mean age 57.5 years, range 20 to 92 years), 69 (12.9%)
had a rhythmic rectal activity.
Of the 382 patients with no history of
neurological disease, 47 (12.3%) exhibited RRCs compared to the 22 of
the 152 patients (14.4%) with a history of neurological disease. The neurological
disease was suprapontine lesion in 5 patients, incomplete spinal cord
lesion in 10 and demyelinating neuropathy in 7. Occurrence of RRCs was
not significantly different in the 2 sub-groups: non-ND and ND.
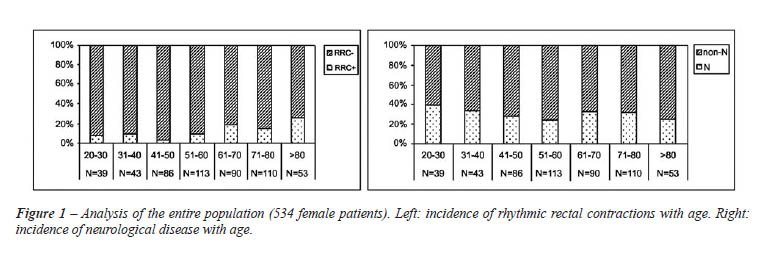
Age was not significantly different between
the two sub-groups of women with RRCs; the mean age was 65.5 ±
15.2 years in the non-ND group compared to 62.7 ± 18.0 years in
the ND group. However, women with RRCs were significantly older than the
negative population (64.6 ± 16.1 years vs. 56.3 ± 17.9 years;
p = 0.0002). Figure-1 shows the progressive increase in RRCs incidence
with age in our population while the neurological disease incidence is
stable or slightly reduced.
RRCs had a low very stable frequency in
the range 1 - 4/min; their amplitude was = 15 cm H2O in 45 non-ND (8.2
± 4.3 cm H2O) and 22 ND patients (8.0 ± 3.3 cm H2O), and
> 15 cm H2O in only 2 non-ND patients.
RRCs occurred during all the filling phase
in 30 non-ND and 19 ND patients, appeared at first desire to void in only
9 non-ND and disappeared during filling in 8 non-ND and 3 ND patients.
Figures 2-4 show examples of the three situations.
RRCs of same characteristics (frequency
and amplitude) were observed in 30 (64%) non-ND and 13 (59%) ND patients
during pressure recordings before the beginning of filling. That event
was independent of the onset, the duration and the end of RRCs during
cystometry.
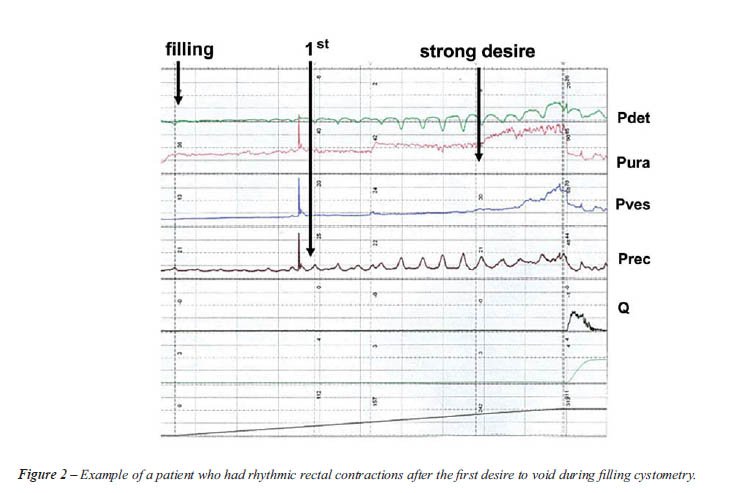
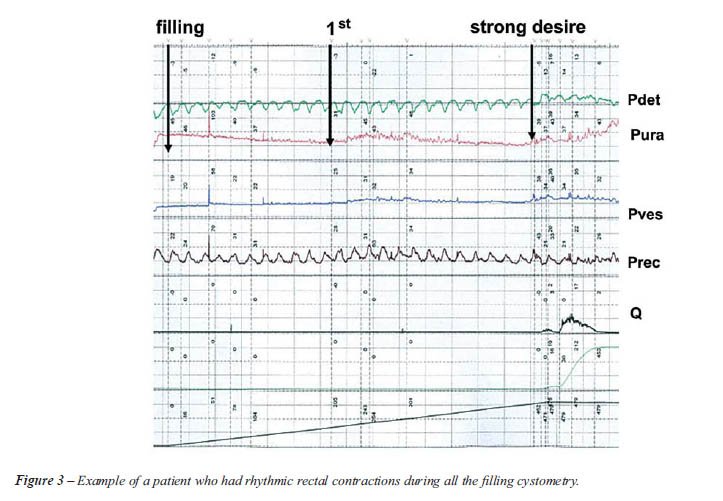
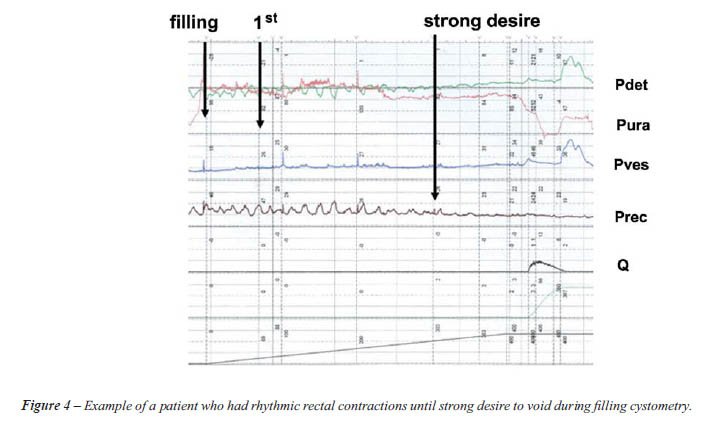
Table-1 describes the incidence of overactive
bladder syndrome and detrusor overactivity.
Comparison with the negative population
allowed to find a correlation of RRCs with OAB (p = 0.0026) but not with
DO (p = 0.35).
Isolated stress urinary incontinence was
observed in only 7 (14.9%) non-ND patients (mean age 56.8 years) of whom
5 had RRCs during all the filling phase.
COMMENTS
Despite
the large use of rectal pressure recordings and of Enhörning hypothesis
to evaluate the abdominal pressure during urodynamics (detrusor pressure
equals vesical pressure minus rectal pressure) only few urodynamicists
have paid attention to or studied the rectal activity during cystometries
(1-3, 8). In all these analyses of rectal contractions during multichannel
urodynamic testing, both rhythmic and random rectal contractions have
been considered. Our study has two distinctive characteristics. First,
we only analyzed the rhythmic rectal contractions and not the random ones;
Prior et al. (9) reported that single rectal contractions and bursts of
phasic motor activity in the human rectum may have a different origin;
filling cystometry is of short duration, less than 20 minutes, which does
not allow for an accurate study of random contraction. Second, the population
was only an adult female population.
RRCs had a low very stable frequency as if produced by a pacemaker, which
led us to compare it with the periodic activity of the gastrointestinal
tract. Rhythmic rectal activity has been previously described: runs of
powerful phasic contractions (2-3/min) or clusters of contractions of
relatively low amplitude (5-6/min) in 12 healthy male volunteers (4) and
(3-6/min) in 9 among 11 healthy women (age range 20-46 years) (10). In
this study on women, rectal pressure was recorded using a perfused urethral
catheter and waves were of higher amplitude (mean 19 cm H2O; range 8-54
cm H2O) than in our study. Data regarding the causes and the circadian
rhythm of this periodic motor activity remain either lacking or conflicting
(11,12). We have observed a rhythmic rectal activity independent of bladder
filling in a large proportion of the population with RRCs despite the
use to measure the rectal pressure of a punctured balloon, which prevents
pressure artifacts arising from contact of the catheter with the rectum
wall. That rectal activity is independent of the neurological status.
Its characteristics (frequency and amplitude) evoke a phase-III like activity;
in the small intestine, the phase III activity (12) is influenced by meal.
The periodic rectal motor activity is supposedly triggered by events in
the neighboring structures (13). Pezzone et al. (14) have described acute
cross-organ sensitization for bladder to bowel and bowel to bladder. That
phenomenon may account for chronic pelvic pain disorders. In addition,
authors of the same team research (15) have demonstrated the convergence
of bladder and colon sensory innervations at the primary afferent level.
Therefore, one can consider the role of bladder filling to stimulate the
rectum and to evoke a contraction. In fact, disappearance of RRCs during
filling was observed in 11 (16%) patients and appearance after first desire
in 9 (13%).
In our population, occurrence of RRCs was not significantly associated
with a history of neurological disease (14.4% vs. 12.3%). That result
differs significantly from the findings of Combs and Nitti (1) and Miranne
et al. (8) who, studying a population including patients with spinal cord
injury and analyzing both rhythmic and random rectal contractions, found
respectively when comparing patients with a history of neurological disease
vs. patients without 51% vs. 29% (1) and 32% vs. 19% (8). In our sub-group
with neurological disease, complaint and urodynamic diagnosis were not
homogeneous. Note that the physiopathology of voiding disturbances due
to a neurological condition is only well characterized in cases of complete
spinal cord lesion.
Occurrence of RRCs is clearly correlated with age as reported by Ozawa
et al. despite the small studied group and probably their older population
(2). It is known that in elderly, DO might be the consequence of changes
in muscarinic receptor subtypes and the non-neural acetylcholine release
from urothelium (16). A similar condition with overproduction of acetylcholine
from the rectum mucosa could be proposed in elderly, leading to rectal
contractions (17). A significant difference is that DO is rarely rhythmic
while the studied phenomenon is rhythmic.
We found some other significant results. Urgency is frequently associated
with RRCs whatever the neurological status and is more frequent than in
the negative population. At the opposite obvious detrusor overactivity
during the cystometry is more frequently associated with RRCs in patients
with a history of neurological disease. Concerning that last result we
have to take into account that several central nervous system disorders
are associated with overactive bladder syndrome (18,19) and detrusor overactivity
(20).
CONCLUSION
RRCs cannot be considered as artefactual events during filling cystometry in women with LUTS. RRCs have to be identified during urodynamics due to their involvement in the detrusor pressure calculation. The rhythmic character of the contractions is consistent with the existence of an oscillator. RRCs occur in the older population, are frequently associated with urgency (OAB syndrome) whatever the population (whether or not there is a history of neurological disease). In the population with a history of neurological disease detrusor overactivity is frequent. Occurrence of RRCs must lead the physician to look at possible causes of urgency and detrusor overactivity. Finally, these findings bring to the fore the role of ageing and possibly of the common neurologic innervation of lower urinary and gastrointestinal tracts in the occurrence of rhythmic rectal contractions.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Combs AJ, Nitti VW: Significance of rectal contractions noted on multichannel urodynamics. Neurourol Urodyn. 1995; 14: 73-80.
- Ozawa H, Nagai A, Akiyama H, Ichikawa T, Akiyama M, Ono N, Oeda T, et al.: Significance of rectal contractions during multichannel urodynamic study. Nippon Hinyokika Gakkai Zasshi. 1997; 88: 874-9.
- Ghoniem GM, Khater U, Elsergany R, Sakr M. The significance of rectal contractions in benign prostatic obstruction. Urodinamica. 2005; 15: 33-8.
- Kumar D, Williams NS, Waldron D, Wingate DL: Prolonged manometric recording of anorectal motor activity in ambulant human subjects: evidence of periodic activity. Gut. 1989; 30: 1007-11.
- Orkin BA, Hanson RB, Kelly KA: The rectal motor complex. J Gastrointest Motil. 1989; 1: 5-8.
- Djurhuus JC, Navarrete RV, Whitaker R, Griffiths D: Standardization of terminology of the hydrodynamics of the upper urinary tract. International Society for the Dynamics of the Upper Urinary Tract, Subcommittee on Standardization of Terminology. Neurourol Urodyn. 1994; 13: 647-54.
- Abrams P, Cardozo L, Fall M, Griffiths D, Rosier P, Ulmsten U, et al.: The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn. 2002; 21: 167-78.
- Miranne JM, Yavagal S, Hernandez-Silen A, Feustel PJ, De EJB. Higher index of suspicion for neurological disease is warranted if rectal contractions occur during multichannel urodynamic testing. J Urol. 2008; 179(suppl 4): 518. Abstract 1520.
- Prior A, Fearn UJ, Read NW: Intermittent rectal motor activity: a rectal motor complex? Gut. 1991; 32: 1360-3.
- Sørensen SM, Gregersen H, Sørensen S, Djurhuus JC: Spontaneous anorectal pressure activity. Evidence of internal anal sphincter contractions in response to rectal pressure waves. Scand J Gastroenterol. 1989; 24: 115-200.
- Auwerda JJ, Bac DJ, Schouten WR: Circadian rhythm of rectal motor complexes. Dis Colon Rectum. 2001; 44: 1328-32.
- Rao SS, Welcher K: Periodic rectal motor activity: the intrinsic colonic gatekeeper? Am J Gastroenterol. 1996; 91: 890-7.
- Kellow JE, Borody TJ, Phillips SF, Tucker RL, Haddad AC: Human interdigestive motility: variations in patterns from esophagus to colon. Gastroenterology. 1986; 91: 386-95.
- Pezzone MA, Liang R, Fraser MO: A model of neural cross-talk and irritation in the pelvis: implications for the overlap of chronic pelvic pain disorders. Gastroenterology. 2005; 128: 1953-64.
- Christianson JA, Liang R, Ustinova EE, Davis BM, Fraser MO, Pezzone MA: Convergence of bladder and colon sensory innervation occurs at the primary afferent level. Pain. 2007; 128: 235-43.
- Andersson KE, Yoshida M: Antimuscarinics and the overactive detrusor--which is the main mechanism of action? Eur Urol. 2003; 43: 1-5.
- Sarna SK: Physiology and pathophysiology of colonic motor activity (2). Dig Dis Sci. 1991; 36: 998-1018.
- Andersson KE, Pehrson R: CNS involvement in overactive bladder: pathophysiology and opportunities for pharmacological intervention. Drugs. 2003; 63: 2595-611.
- Brading AF: A myogenic basis for the overactive bladder. Urology. 1997; 50(6A Suppl): 57-67; discussion 68-73.
- Andersson KE: Mechanisms of Disease: central nervous system involvement in overactive bladder syndrome. Nat Clin Pract Urol. 2004; 1: 103-8.
____________________
Accepted after revision:
March 12, 2009
_______________________
Correspondence address:
Dr. Françoise A. Valentini
Hôpital Charles Foix
7, avenue de la République
Ivry-sur-Seine, 94200, France
Fax: + 33 1 4959-4697
E-mail: francoise.valentini@jrs.aphp.fr
EDITORIAL COMMENT
This is
an excellent paper that clearly establish that rhythmic rectal contractions
(RRCs) and is of clinical interest and value. For those of us who do urodynamics
for a living we all suspect that there is science in the RRC’s we
have seen but were always sort of shy to speak up because other experts
may not believe us. However, since my collaboration with Dr. Mike Pezzone
in the field of gastroenterology over the past decade it is becoming obvious
to me of the interconnection between urinary and colorectal system (1).
The take home message is that cross-talk exists between the bladder/urethra
and rectum/anus and that RRCs may be a valuable parameter to help us to
help our patients with pelvic diseases.
REFERENCE
- Pezzone MA, Liang R, Fraser MO: A model of neural cross-talk and irritation in the pelvis: implications for the overlap of chronic pelvic pain disorders. Gastroenterology. 2005; 128: 1953-64.
Dr.
Michael B. Chancellor
Neurourology Program
Department of Urology
William Beaumont Hospital
Royal Oak, Michigan, USA
E-mail: chancellormb@gmail.com
EDITORIAL COMMENT
This interesting
study reported the rhythmic rectal contractions (RRCs) during a urodynamic
study in women with lower urinary tract symptoms (LUTS) with or without
any neurological lesion. The incidence of RRCs was 69/534 (13%) without
significant difference between those with (14.5%) and without (12.3%)
neurological lesion. However, the mean age of women with RRCs was significantly
older than those without RRCs. RRCs were also noted to associate with
urgency symptoms, but RRCs were associated with occurrence of detrusor
overactivity (DO) only in patients with neurological lesions.
In fact, RRCs are not uncommon finding during urodynamic study especially
in patients with neurogenic voiding dysfunction. Convergence of the bladder
and distal colon sensory innervation had been shown in rat model at dorsal
root ganglion neurons. This pelvic organ cross-sensitization may play
a role in the overlap of pelvic pain disorders (1). Because rectum and
bladder have common neurological reflex arc in sacral cords, therefore,
RRCs can be regarded as reflex contractions associated with sensory input
through inserting rectal catheter or urethral catheter. If the rectal
catheter or urethral catheter is placed for a longer period, RRCs could
disappear. The authors might observe the disappearance of RRCs after resting
for a longer period. If this phenomenon is observed after a longer period
of rest, we should wait for the disappearance of RRCs before starting
the urodynamic study to ensure a correct subtracted detrusor pressure.
The results of this study also found a higher incidence of RRCs in older
population although there was no significant difference between women
with and without neurological lesions. Studies have revealed that the
urothelium is involved in sensory mechanisms It has been demonstrated
that in the human bladder mucosa, acetylcholine and adenosine triphosphate
production from urothelium increased in older patients (2). Intravesical
instillation of antimuscarinic agent in rat bladder can block muscarinic
receptors in bladder-afferent pathways (3). Older women might also have
overproduction of acetylcholine in the mucosa of rectal wall, which might
also result in spontaneous contractions through stretching of the rectal
wall after inserting rectal catheter. Moreover, chronic constipation is
a more frequent disorder in the elderly. It is possible that the elderly
women have a higher incidence of chronic constipation, which in turn causes
frequent RRCs in response to rectal stimulation by the rectal catheter.
The bladder and rectum are located at the convergence area in the sacral
cord. The sensation of one organ (bladder) can be induced by stimulating
the other organ (rectum). Therefore, rectal stimulation might evoke sensory
response (urgency sensation) or DO in the urinary bladder and hence resulting
in an urgency sensation during urodynamic study. Therefore, it is not
surprising that occurrence of RRCs is associated with urgency sensation
in overall patients and with DO in patients with neurological lesion.
The clinical implication of RRCs might be the provocation of sensory urgency
or DO in women who have a hyperactive rectum during natural bladder filling.
This phenomenon may be observed in some patients with chronic constipation
and overactive bladder symptoms due to this hyperactive rectum and RRCs
in their daily life. Based on the findings of this study and the possible
mechanism of RRCs, we should not consider RRCs as artefactual events during
cystometry. Moreover, in cases of RRCs occurrence without concomitant
urgency or DO (as in 34 patients in this study) during the urodynamic
study, the disordered rectum might be considered as the origin of their
LUTS. Treatment with antimuscarinic might also be beneficial in these
patients.
REFERENCES
- Christianson JA, Liang R, Ustinova EE, Davis BM, Fraser MO, Pezzone MA: Convergence of bladder and colon sensory innervation occurs at the primary afferent level. Pain. 2007; 128: 235-43.
- Yoshida M, Miyamae K, Iwashida H, Otani M, Inadome A: Management of detrusor dysfunction in the elderly: Changes in acetylcholine and adenosine triphosphate release during aging. Urology. 2004; 63 (3 Suppl 1): 17-23.
- Kim Y, Yoshimura N, Masuda H, de Miguel F, Chancellor MB: Antimuscarinic agents exhibit local inhibitory effects on muscarinic receptors in bladder-afferent pathways. Urology. 2005; 65: 238-42.
Dr.
Hann-Chorng Kuo
Department of Urology
Buddhist Tzu Chi General Hospital and
Tzu Chi University
Hualien, Taiwan
E-mail: hck@tzuchi.com.tw