Endourological
Management of Forgotten Encrusted Ureteral Stents
(
Download pdf )
Clinical Urology
doi: 10.1590/S1677-55382010000400005
Kusuma V. R. Murthy, S. Jayaram Reddy, D. V. Prasad
Department of Urology, Osmania General Hospital, Hyderabad, Andhra Pradesh, India
ABSTRACT
Purpose:
To present our experience and discuss the various endourological approaches
for treating forgotten encrusted ureteral stents associated with stone
formation.
Materials and Methods: From July 2006 to
December 2008, 14 patients (11 men and 3 women) with encrusted ureteral
stents were analyzed. The average indwelling time of the stent was 4.9
years (range 1 to 12). Plain-film radiography was used to evaluate encrustation,
stone burden, and fragmentation of the stents. Intravenous urogram and
a Tc99m diethylene triamine penta acetic-acid renogram was used to assess
renal function.
Results: In seven patients, the entire stent
was encrusted, in three patients the encrustation was confined to the
ureteral and lower coil part of the stent, two patients had encrustation
of the lower coil, and minimal encrustation was observed in two patients.
Percutaneous nephrolithotomy was performed in 5 cases and retrograde ureteroscopy
with intra-corporeal lithotripsy in 9 patients. Cystolithotripsy was used
to manage the distal coil of the encrusted stent in eight patients. Simple
cystoscopic removal of the stents with minimal encrustation was carried-out
in two cases. Looposcopy and removal of the stent was performed in one
patient with an ileal conduit and retained stent. Only one patient required
open surgical removal of the stent. Thirteen out of 14 patients were rendered
stone and stent free in one session. All except two stents were removed
intact and stone analysis of encrustation and calcification revealed calcium
oxalate and calcium phosphate in the majority of the cases.
Conclusion: Endourological management of
forgotten encrusted stents is highly successful and often avoids the need
for open surgical techniques.
Key
words: stents; ureteral; forgotten; lithiasis; management; endourology
Int Braz J Urol. 2010; 36: 420-9
INTRODUCTION
Ureteral stents are widely used in urological practice. They are mainly indicated after any ureteral surgery and for managing ureteral obstruction due to intrinsic or extrinsic causes like stones, strictures, uretero-pelvic junction obstruction, retroperitoneal fibrosis, malignancies, and congenital anomalies (1-5). They are also placed after iatrogenic injuries to the ureter and before any complex abdominal procedure for identification and protection of the ureters (6). Because of their wide spread usage, complications due to these stents have also increased like, stent encrustation, stent fragmentation, stone formation and recurrent urinary tract infection (7,8). Retention of ureteral stents, often due to poor compliance of the patient is not uncommonly seen (9). If left untreated, these retained stents result in significant morbidity and mortality. Various methods of treatment combinations of extracorporeal shock wave lithotripsy (SWL), cystolithotripsy (CLT) retrograde ureteroscopy with intracorporeal lithotripsy, percutaneous nephrolithotomy (PCNL) and open surgery have been used for retrieval of these encrusted stents (10-14). We present our experience with the management of these forgotten stents, associated with significant encrustation and stone burden in 14 patients.
MATERIALS AND METHODS
Fourteen
patients (11 men and three women) with forgotten ureteral stents with
severe encrustation, who presented at our department between July 2006
and December 2008, were treated. Information was obtained through a retrospective
review of patients records. The mean patient age was 42.4 years (range
27-55 years) and the average indwelling time of the stent was 4.9 years
(range 1-12 years).All the stents were placed elsewhere. Poor compliance
and inability of the treating surgeon to counsel the patients were the
reasons for retention of these stents. All the patients were evaluated
for stent encrustation and associated stone burden by plain-film radiography
and intravenous urogram. In patients with non visualized kidneys on intravenous
urogram, Tc99m diethylene triamine penta acetic-acid (DTPA) renogram was
done to estimate the renal function. Treatment decision was made on clinical
and radiological findings. Before intervention, all patients had negative
urine cultures, and antibiotic prophylaxis was given for all cases.
Combined endourological procedures PCNL,
Cystolithotripsy (CLT), retrograde ureteroscopy with intracorporeal lithotripsy
were performed in one session. Retrograde ureteroscopy was performed using
8/9.8F and 6/7.5F semi rigid ureteroscope, under fluoroscopic guidance.
Intracorporeal lithotripsy was performed with a pneumatic lithotripter.
PCNL was carried-out using a rigid 24F nephroscope. In stents with minimal
encrustation on plain-film radiography, a gentle attempt is made for removal
with the help of grasping forceps passed through the cystoscope under
local anesthesia and fluoroscopic guidance. For patients with encrustation
and stone burden involving the lower coil, ureteric (body) or whole of
the stent, initially, cystolithotripsy, retrograde ureteroscopy and intra
corporeal lithotripsy was performed in the dorsal lithotomy position.
Following this, a gentle attempt was made to retrieve the stent with the
help of an ureteroscopic grasper. If the stent failed to uncoil, a ureteric
catheter was placed adjacent to the encrusted stents for injection of
radio-contrast material to delineate the renal pelvis and the calyces.
Then the patient was placed in the prone position and PCNL of the upper
coil of the encrusted stent along with calculus was done. The approach
to the collecting system was through the lower calyx and middle posterior
calyx and no patient required upper pole or supra costal access. A 14F
nephrostomy tube was kept indwelling for 48 hours, in patients who required
PCNL. Stone analysis and encrustation analysis was done in all cases.
Post operatively, plain-film radiography was done to confirm the stone
free and stent free status.
RESULTS
The patient characteristics, initial indications for stenting, indwelling time, site of encrustation, type of procedure performed and length of hospital stay are shown in Table-1. The entire stent was encrusted in 7 patients; three patients had predominantly ureteric (body) and lower coil encrustation (Figure-1) and in 2 patients, there was minimal encrustation. In 11 out of 14 patients, the initial indication for stent placement was for urinary stone disease. General anesthesia was required for removal of the encrusted stents in eleven patients, and three patients were managed as outpatients under local anesthesia. The mean hospital stay in 11 patients was 4.9 days. As shown in Table-1, CLT was required to treat the distal end of the stent in seven cases. PCNL was done in 5 cases. Retrograde ureteroscopy and intra corporeal lithotripsy was performed in eight cases. Simple cystoscopic removal of the stent under fluoroscopic guidance was done in two cases.

A 54-year-old male patient who underwent
radical cystectomy and ileal conduit 4 years previously, presented with
left loin pain and dysuria for 3 months. Plain-film radiography of the
abdomen revealed a retained stent on the left side with minimal encrustation.
Looposcopy with 24F nephroscope and removal of the retained stent was
done with the help of a grasping forceps under fluoroscopic guidance.
One patient presented with a left retained
ureteral stent for 9 years and right upper ureteric calculus, and a serum
creatinine level of 5.4 mg%. Initially, a right ureteral stent was placed
to normalize the renal parameters, and subsequently, a push back PCNL
was done for the right ureteric calculus to achieve complete stone clearance.
On the left side, a retrograde ureteroscopy with intracorporeal lithotripsy
and PCNL was required to fragment and retrieve the encrusted stent (Figure-2).

Another patient presented with retained
stent for 9 years following pyelolithotomy on the left kidney. Plain-film
radiography showed extensive calcification of the entire stent. Intravenous
urogram and DTPA renogram showed good renal function. CLT of the lower
coil of the encrusted stent was attempted, but the pneumatic lithotripter
failed to fragment the stone. Since we do not have the facility of laser
lithotripsy open surgical removal by cystolithotomy, ureterotomy and pyelolithotomy
was done to retrieve the stent (Figure-3).

Percutaneous nephrostomy was carried-out in one patient who presented
with acute pyelonephritis. The dwelling time of the encrusted stent in
this patient was 12 years. After negative bacterial culture of the blood
and urine, the patient underwent surgery. CLT, retrograde ureteroscopy
with intracorporeal lithotripsy was required for removal of the stent.
On the second postoperative day, he developed urosepsis, requiring broad
spectrum antibiotics and intensive care management. This patient had a
prolonged hospital stay of 14 days. Thirteen out of 14 patients (93%)
were rendered stone free and stent free after a single anesthetic session.
Re-stenting was done in one patient requiring open surgery and subsequently,
his stent was removed after four weeks. No intra operative complications
occurred in any patient. All the stents were removed intact except in
two patients, who had fragmented stents at presentation. Stone analysis
showed calcium oxalate and phosphate in the majority of cases. Struvite
stones were seen in two cases.
COMMENTS
Forgotten
ureteral stents are observed in urologic practice because of poor compliance
of the patient or failure of the physician to adequately counsel the patient.
These forgotten stents can produce considerable morbidity and mortality,
due to extensive encrustation with significant stone burden, knot formation,
upward migration and fragmentation (7,15). Encrustation of forgotten stents
associated with large stone burden is a serious problem, due to complications
like recurrent urinary tract infection, hematuria, obstruction and renal
failure (16). The deposition of encrusted material on retained ureteral
stents can occur in both infected and sterile urine. The mechanism of
encrustation in infected urine is a result of organic components in the
urine crystallizing out onto the surface of biomaterial and becoming incorporated
into a bacterial biofilm layer. Urease produced by the adhered bacteria
hydrolyses the urea to produce ammonia. This elevates urinary pH, favoring
the precipitation of magnesium and calcium as struvite and hydroxyl apatite
(17,18). Although the exact mechanism of encrustation in sterile urine
is unclear, it appears to be dependent on the pH, ionic strength and biomaterial
hydrophobic properties (19). The degree of encrustation is dependant on
the dwelling time. El faqih et al. found that encrustation increased from
9.2% at < 6 weeks to 47.5% at six to 12 weeks to 76.3% at > 12 weeks
of dwelling time (20). Other factors implicated in the increased incidence
of encrustations are chronic recurrent stone formers, metabolic predisposition
to stone disease, congenital renal anomalies, malignant urinary obstruction
and pregnancy (21).
Fragmentation is another important complication
of the forgotten stents. It is the result of loss of tensile strength,
which is due to hardening and degeneration of the stent polymers (22).
The risk of encrustation and fragmentation is dependant on the type of
material of the stent. Silicone was found to be least prone to encrustation,
followed by polyurethane, silitek, percuflex and hydro gel coated polyurethane
(23). Fragmentations of polyurethane stents are four times as frequent
as the silicone stents (9). In our series, fragmentation of the lower
coil of the stent is seen in two cases at the time of presentation. The
indwelling time in both the cases was five years. All the retrieved encrusted
stents in our series were made of polyurethane.
Retained ureteral stents with encrustation is a challenging problem for
endourologists. Very often, multiple endourological approaches are needed
because of encrustations and the associated stone burden that may involve
bladder, ureter and kidney. This may require single or multiple endourological
sessions or rarely open surgical removal of the encrusted stents. Singh
et al. described multiple accesses and approaches including open surgery
to treat the retained stents (24). Borboroglu et al. also reported the
endourological treatment of four patients with severely encrusted ureteral
stents with a large stone burden. All patients required two to six endourological
approaches (average 4.2) performed at one or multiple sessions, to achieve
stone-free and stent-free status. These authors concluded that percutaneous
nephrolithotomy and ureteroscopy are often necessary for treating a severely
encrusted stent and associated stone burden (13). One stage removal of
12 encrusted retained ureteral stents has been reported by Bukkapatnam
et al., in ten patients. Of these, 11 were managed by ureteroscopy alone
and in one patient; the stone was treated through a percutaneous approach.
They concluded that, these stents can be removed in one sitting with minimal
morbidity and short hospital stay (25). Using a combination of SWL, PCNL,
CLT, ureteroscopy with intra corporeal lithotripsy, clearance rates ranging
from 75 to 100% have been reported (10,12,22).
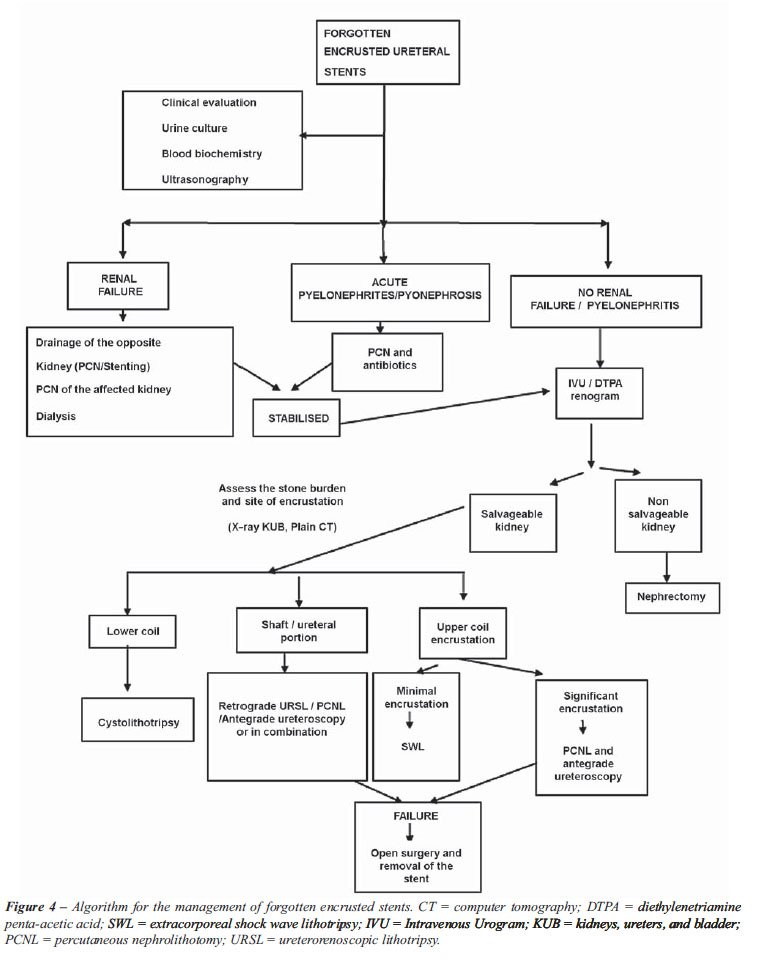
The site of encrustation, associated stone
burden and the function of the affected kidney often dictate the method
of access and treatment (Figure-4). Our approach towards management of
these difficult stents is based on the findings on plain-film radiography.
The proximal, distal coils and the body of the stent are examined for
encrustation, calcification and fragmentation. We did not find any additional
benefit in the management plan with the use of non contrast computed tomography.
Intravenous urogram and DTPA renogram is obtained to determine the function
of the kidney. Nephrectomy is done for non salvageable function of the
kidney. Nephrostomy or placement of second stent is done, if the patient
presented with pyelonephritis and sepsis. It is possible to put a second
stent adjacent to the encrusted stent because the ureter is dilated in
majority of these cases.
Extracorporeal shock wave lithotripsy (SWL)
is the initial treatment with stents with minimal encrustation. However,
in our series, no patient required SWL because of extensive stone burden
in majority of cases. If there are no encrustations visible on plain-film
radiography, our approach is cystoscopic removal using a grasping forceps
under local anesthesia with fluoroscopic guidance. Gentle traction on
the stent is applied, if patient complains of pain and if the stent does
not uncoil, the procedure is abandoned. An important precaution during
the procedure is to avoid using excessive force, which can result in breakage
of the stent along with ureteral injury or ureteral avulsion.
The next stage is CLT with the help of pneumatic
lithotripter on stents with minimal encrustation and those with lower
coil encrustation. This followed by gentle pull under fluoroscopic guidance.
If the cystoscopic approach fails, and in patients with encrustation involving
the ureteric portion of the stent, the next approach is under anesthesia,
a safety guide wire is passed along the retained stent and ureteroscope
is passed retrograde. Calcifications over the stent can be fragmented
with a pneumatic lithotripter or laser energy, while carefully advancing
the ureteroscope into the renal pelvis. After all the encrustations and
calcification have been fragmented, the stent is gently removed with the
help of grasping forceps passed through the ureteroscope under fluoroscopic
guidance. Following removal of the stent, it is mandatory to do a retrograde
uretrogram and check ureteroscopy to rule out a ureteric injury. If any
signs of ureteric injury or contrast extravasation present, the patient
should be re-stented.
For stents with large stone burden and those
stents which fail to be retrieved by the above-mentioned techniques, a
5F ureteric catheter is placed to enable the injection of radio contrast
material into the renal pelvis and calyces as an aid to subsequent percutaneous
access and the patient is placed in the prone position. Percutaneous access
is established by a lower calyceal or middle calyceal puncture and the
proximal coil of the stent along with stone is fragmented. The stent is
gently removed under fluoroscopic guidance through the percutaneous nephrostomy
tract.
Using the above-mentioned approach, it was possible to remove all stents
in 13 out of 14 patients, using the endourological approach alone under
a single anesthesia. Open surgery was done in one case because of the
extensive stone burden and failure of the pneumatic lithotripter to fragment
the stone. Based on our method of approach, an algorithm has been proposed
for the management of these stents (Figure-4).
Although, endourological management of these
stents achieves success in majority of the cases with minimal complications,
the best treatment that remains is prevention of this complication. The
treating physician should be very selective in placing the stents and
they must be tracked very closely by documenting insertion and removal
of the stents. All patients should be counseled with respect to the complications
of long term use and advised when their stent should be changed. As mentioned
earlier, the degree of encrustation is dependant on the indwelling time,
so, it is necessary to keep the indwelling time to as short as possible.
Various authors have reported that indwelling time between 2-4 months
is safe (9-12,20). For patients requiring stents beyond this period, they
should be kept on prophylactic antibiotics and have their stents frequently
changed.
It is interesting to note that, two of three
patients who did not have stents for stone disease, were able to have
their stents simply removed by cystoscopy, while this was successful in
none of the stone formers. The reason for this could be due to increase
risk of encrustation and stone formation in patients who have a history
of stone disease. This underscores the importance of frequent monitoring
in these groups of patients to avoid life threatening complications.
It is also important to maintain a proper
record of all stents inserted and keep a track of their due date of removal.
Some authors have proposed a computerized tracking program for removal
stents (26). Coatings such as hydrophilic polymers, heparin, pentosan
polysulfate, or oxalate -degrading enzymes have been used in an attempt
to reduce encrustation (27-30). The use of bio-degradable compound of
poly-L-lactic and glycolic acids which are designed to disintegrate can
eliminate the problem of retention and encrustation of the stents in the
near future (31).
CONCLUSION
Encrustation
and stone formation in forgotten stents often lead to life threatening
complications and pose a challenging management task for the treating
surgeon.
The use of various combinations of endourological
techniques can achieve effective stent and stone treatment after a single
anesthesia session with minimal morbidity and short hospital stay. Imaging
and assessment of the degree of stone burden is important, before making
any attempt to remove these stents. Maintenance of efficient log book
under direct supervision of treating surgeon and proper patient counseling
is required to prevent this complication.
ACKNOWLEDGEMENTS
Drs. Panduranga Rao, T. Jagadeshwar, Srinivas, Purusotham, Sudershan, and Roopali provided support to this study.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Saltzman B: Ureteral stents. Indications, variations, and complications. Urol Clin North Am. 1988; 15: 481-91.
- Chew BH, Knudsen BE, Denstedt JD: The use of stents in contemporary urology. Curr Opin Urol. 2004; 14: 111-5.
- Hepperlen TW, Mardis HK, Kammandel H: The pigtail ureteral stent in the cancer patient. J Urol. 1979; 121: 17-8.
- Gogas J, Markopoulos C, Kouskos E, Gogas H, Kiriakou V: Metastatic retroperitoneal and mediastinal fibrosis as first sign of recurrence of breast cancer. Eur J Surg. 2001; 167: 715-8.
- Park DS, Park JH, Lee YT: Percutaneous nephrostomy versus indwelling ureteral stents in patients with bilateral nongenitourinary malignant extrinsic obstruction. J Endourol. 2002; 16: 153-4.
- Kuno K, Menzin A, Kauder HH, Sison C, Gal D: Prophylactic ureteral catheterization in gynecologic surgery. Urology. 1998; 52: 1004-8.
- Damiano R, Oliva A, Esposito C, De Sio M, Autorino R, D’Armiento M: Early and late complications of double pigtail ureteral stent. Urol Int. 2002; 69: 136-40.
- Schulze KA, Wettlaufer JN, Oldani G: Encrustation and stone formation: complication of indwelling ureteral stents. Urology. 1985; 25: 616-9.
- Monga M, Klein E, Castañeda-Zúñiga WR, Thomas R: The forgotten indwelling ureteral stent: a urological dilemma. J Urol. 1995; 153: 1817-9.
- Mohan-Pillai K, Keeley FX Jr, Moussa SA, Smith G, Tolley DA: Endourological management of severely encrusted ureteral stents. J Endourol. 1999; 13: 377-9.
- Flam TA, Brochard M, Zerbib M, Debre B, Steg A: Extracorporeal shock-wave lithotripsy to remove calcified ureteral stents. Urology. 1990; 36: 164-5.
- Somers WJ: Management of forgotten or retained indwelling ureteral stents. Urology. 1996; 47: 431-5.
- Borboroglu PG, Kane CJ: Current management of severely encrusted ureteral stents with a large associated stone burden. J Urol. 2000; 164: 648-50.
- Lam JS, Gupta M: Tips and tricks for the management of retained ureteral stents. J Endourol. 2002; 16: 733-41.
- Eisner B, Kim H, Sacco D: Repeat knot formation in a patient with an indwelling ureteral stent. Int Braz J Urol. 2006; 32: 308-9.
- Singh V, Srinivastava A, Kapoor R, Kumar A: Can the complicated forgotten indwelling ureteric stents be lethal? Int Urol Nephrol. 2005; 37: 541-6.
- Wollin TA, Tieszer C, Riddell JV, Denstedt JD, Reid G: Bacterial biofilm formation, encrustation, and antibiotic adsorption to ureteral stents indwelling in humans. J Endourol. 1998; 12: 101-11.
- Robert M, Boularan AM, El Sandid M, Grasset D: Double-J ureteric stent encrustations: clinical study on crystal formation on polyurethane stents. Urol Int. 1997; 58: 100-4.
- Keane PF, Bonner MC, Johnston SR, Zafar A, Gorman SP: Characterization of biofilm and encrustation on ureteric stents in vivo. Br J Urol. 1994; 73: 687-91.
- el-Faqih SR, Shamsuddin AB, Chakrabarti A, Atassi R, Kardar AH, Osman MK, et al.: Polyurethane internal ureteral stents in treatment of stone patients: morbidity related to indwelling times. J Urol. 1991; 146: 1487-91.
- Lojanapiwat B: Endourological management of severely encrusted ureteral stents. J Med Assoc Thai. 2005; 88: 1203-6.
- Zisman A, Siegel YI, Siegmann A, Lindner A: Spontaneous ureteral stent fragmentation. J Urol. 1995; 153: 718-21.
- Tunney MM, Keane PF, Jones DS, Gorman SP: Comparative assessment of ureteral stent biomaterial encrustation. Biomaterials. 1996; 17: 1541-6.
- Singh I, Gupta NP, Hemal AK, Aron M, Seth A, Dogra PN: Severely encrusted polyurethane ureteral stents: management and analysis of potential risk factors. Urology. 2001; 58: 526-31.
- Bukkapatnam R, Seigne J, Helal M: 1-step removal of encrusted retained ureteral stents. J Urol. 2003; 170: 1111-4.
- Ather MH, Talati J, Biyabani R: Physician responsibility for removal of implants: the case for a computerized program for tracking overdue double-J stents. Tech Urol. 2000; 6: 189-92.
- Gorman SP, Tunney MM, Keane PF, Van Bladel K, Bley B: Characterization and assessment of a novel poly(ethylene oxide)/polyurethane composite hydrogel (Aquavene) as a ureteral stent biomaterial. J Biomed Mater Res. 1998; 39: 642-9.
- Riedl CR, Witkowski M, Plas E, Pflueger H: Heparin coating reduces encrustation of ureteral stents: a preliminary report. Int J Antimicrob Agents. 2002; 19: 507-10.
- Watterson JD, Cadieux PA, Beiko DT, Cook AJ, Burton JP, Harbottle RR, et al.: Oxalate-degrading enzymes from Oxalobacter formigenes: a novel device coating to reduce urinary tract biomaterial-related encrustation. J Endourol. 2003; 17: 269-74.
- Zupkas P, Parsons CL, Percival C, Monga M: Pentosanpolysulfate coating of silicone reduces encrustation. J Endourol. 2000; 14: 483-8.
- Lingeman JE, Preminger GM, Berger Y, Denstedt JD, Goldstone L, Segura JW, et al.: Use of a temporary ureteral drainage stent after uncomplicated ureteroscopy: results from a phase II clinical trial. J Urol. 2003; 169: 1682-8.
____________________
Accepted
after revision:
January 12, 2010
_______________________
Correspondence
address:
Dr. K. V. R. Murthy
Department of Urology
Osmania General Hospital
Afzal gunj, Hyderabad 500012
Andhra Pradesh, India
Fax: + 91 40 2460-0260
E-mail: murthy.kusuma@rediffmail.com