A SIMPLE SURGICAL TECHNIQUE TO MINIMIZE POSTOPERATIVE URINARY RETENTION WITH A PUBOVAGINAL SLING
STEVEN P. PETROU, FABIO BARACAT, L.A. RIBEIRO FILHO, PAUL R. YOUNG
Department of Urology, Mayo Clinic, Jacksonville, Florida, USA
ABSTRACT
Purpose:
Suburethral sling surgery has traditionally been associated with a high
incidence of permanent urinary retention. We describe a method of pubovaginal
sling placement that limits permanent postoperative urinary retention
and restores continence.
Material and Methods: A total of 100 women
with clinically proven stress urinary incontinence who received a suburethral
pubovaginal sling were reviewed retrospectively. Each patient had an autologous
abdominis rectus fascia pubovaginal sling placed by the identical technique
of adjusting tension by tying over an inverted Kelly surgical clamp with
the operative table in a 20° reverse Trendelenburg position. Emphasis
of chart review was on rate of surgical success and incidence of permanent
postoperative urinary retention.
Results: Ninety-eight of the women were
continent of urine. No patient suffered from permanent urinary retention.
Conclusions: This method provides a simple
way of placing a suburethral sling that limits permanent urinary retention
and still achieves good surgical results.
Key words:
urinary incontinence; female; prostheses and implants; urination disorders
Braz J Urol, 27: 275-280, 2001
INTRODUCTION
The
suburethral sling procedure may be among the most durable of all forms
of surgical treatment for stress urinary incontinence (SUI) (1-5).
Despite increased acceptance of suburethral
sling procedures, the technical aspect of intraoperative adjustment of
sling tension remains unclear. The goal of the standard suburethral sling
procedure is to cure urinary incontinence without inducing unwanted outflow
obstruction. To achieve this result, different technical methods of adjusting
the sling tension have been suggested: cystoscopic appearance, urodynamic
variables, or ultrasonography (5-8). Others have been based on simplified
trigonometric analysis using the cystoscope sheath or cotton swab angle
(9-11).
We present a simple method of suburethral
sling placement not dependent on radiographic or cystoscopic visualization
or rotational adjustment.
MATERIAL AND METHODS
Patients
Between January 1995 and May 1998, 100 consecutive
women with SUI underwent a pubovaginal sling procedure with autologous
rectus abdominis fascia by one of two surgeons using the identical technique.
The patients’ hospital charts, urodynamic tests, and clinical records
were reviewed retrospectively.
Preoperative evaluation included a urologic-based
history and physical examination, urinalysis, videourodynamic studies,
and, when indicated, cystourethroscopy. Urethral mobility was assessed
by fluoroscopic visualization of the urethra with maximal straining and
200 ml of 20% iodinated contrast medium in the bladder. Patients’
incontinence was classified urodynamically in a previously described manner
(12): urethral hypermobility if the abdominal leak point pressure was
greater than 90 cm H2O, intrinsic sphincter deficiency if the abdominal
leak point pressure was less than 60 cm H2O, and a combination of the
two if the abdominal leak point pressure was between 60 and 90 cm H2O.
Postoperatively, several clinical variables
were assessed. The first was whether the patients were continent of urine.
Continence was defined by the combination of patient perception, no pad
usage, and no visualized leakage per urethra while the patient strained
with 200 ml of isotonic saline in the bladder. The second was whether
they had urinary retention. This was defined by inability to void for
more than 30 days from the placement of the suburethral sling. The third
was the determination of the presence of postoperative urgency.
Surgical
Technique
All patients underwent a modified pubovaginal
suburethral sling procedure utilizing a Cobb-Ragde needle (13). With this
technique, a 2 x 10-cm rectus fascial strip is harvested from the anterior
rectus sheath. Each end of the sling is oversewn with a number one blue
monofilament polypropylene suture, which will act as the sling-suspending
suture (Figure-1). The harvest site is closed with a running number one
violet monofilament polydioxanone suture. Standard transvaginal dissection
through an inverted U incision allows access to the retropubic space.
A Cobb-Ragde needle is passed from an intact region of the anterior rectus
fascia, at least 2 to 3 cm inferior to the harvest site, under digital
control through the retropubic space and out through the vaginal incision.
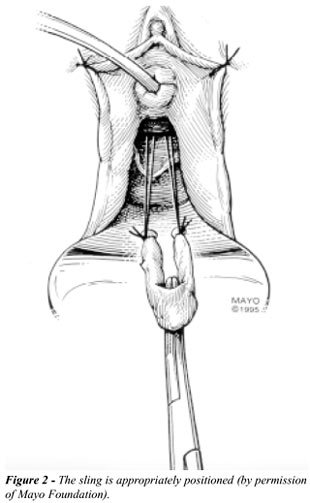
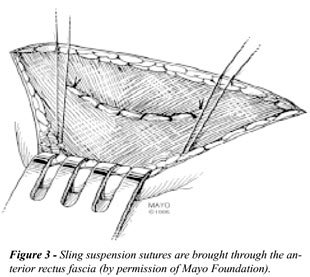
The sling sutures are threaded and transferred suprapubically and then
elevated to remove all slack (Figures-2 and 3). The sling is positioned
just distal to the bladder neck. To prevent twisting, the sling is sutured
in place to the periurethral fascia with 4-0 Vicryl. Indigo carmine is
administered intravenously and cystourethroscopy is done to ensure that
no suture material has violated the bladder and to document bilateral
blue-tinged ureteral efflux (14). A suprapubic tube is placed with standard
technique. After cystoscopy, a 16F Foley catheter is reinserted. The weighted
vaginal retractor previously placed is removed. The patient is placed
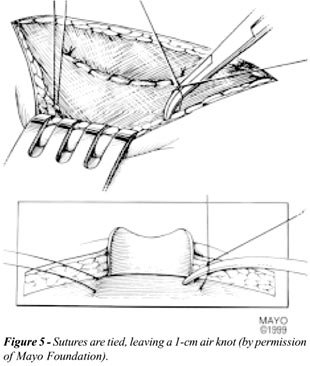
in 20° reverse Trendelenburg position (Figure-4). The ipsilateral
sling-suspending sutures are now tied over an inverted 10-inch Kelly clamp
(the convex side), yielding an approximately 1-cm air knot (Figure-5).
The bilateral sutures are tied to each other over the midline in a loose
loop. Surgical closure is now completed.

With this technique, once the Kelly clamp
is removed, there is no tension on the suspending sutures because of the
air knot. Cystoscopy is not performed to confirm urethral wall coaptation.
The procedure is performed in the same fashion for patients with urethral
hypermobility and for those with intrinsic sphincter deficiency, including
stovepipe urethra.
The urethral catheter is removed on the
first postoperative day, and the suprapubic tube is plugged. The patients
begin their voiding trial and measure postvoid residuals via the suprapubic
tube after each void. The suprapubic tube is removed once the postvoid
residual is consistently less than 100 ml.
Follow-up
Follow-up in these 100 patients ranged from
4 to 36 months (mean, 6.3 months). Face-to-face interviews with the patients,
telephone interviews, and chart review were done.
RESULTS
Preoperative
evaluation determined that 55 patients had urinary incontinence secondary
to urethral hypermobility, 21 had urinary incontinence due to intrinsic
sphincter deficiency, and 24 had both.
Concomitant procedures performed with the
pubovaginal sling in the 100 patients included: anterior repair (6), posterior
repair (3), anterior and posterior repair (2), vaginal hysterectomy (1),
transurethral resection of bladder tumor (1), urethral diverticulectomy
(1), abdominal panniculectomy (1), urethrovesical fistulectomy (1), and
pelvic lipoma resection (1).
The operative procedure was well tolerated
by all the patients; no patients required transfusion or experienced any
medical or surgical complications.
The suprapubic tube was removed within 4
weeks after operation in all patients. Actual date of removal depended
on the combination of acceptable residuals and when the patient could
come to the clinic.
Of the 100 patients, 98 had no postoperative
SUI. Both failures were reevaluated with videourodynamics. The first patient
had urethral hypermobility preoperatively and had a pubovaginal sling
only. Postoperative urodynamics revealed a decline of her Valsalva leak
point pressure from 126 to 86 cm H2O. On fluoroscopic imaging, her bladder
neck and urethra revealed increased mobility as well as leakage of contrast
medium consistent with new-onset intrinsic sphincter deficiency. The second
patient also had urethral hypermobility preoperatively and had a pubovaginal
sling only. Her postoperative urodynamics showed an increase of her Valsalva
leak point pressure from 127 cm H2O to 135 cm H2O. On fluoroscopy with
stress maneuvers, her urethra no longer had any hypermoblility but she
did have leakage per urethra of contrast medium. There were no patients
with permanent urinary retention.
Seven of the 100 patients had new-onset
urgency after operation. Four manifested the urgency symptoms immediately
after operation, and three presented with the symptoms more than 1 year
after the procedure. Patients with de novo urgency underwent evaluation,
including repeat assessment of postvoid residual and urethral sounding
to eliminate the possibility of any undue tethering and videourodynamics
when indicated. Average postvoid residual in the new-onset urgency group
was 60 ml (range, 20-100 ml). No objective evidence of outflow obstruction
was found, and none of the patients underwent a later urethrolysis.
DISCUSSION
An
active debate continues over the optimal sling tension that produces urinary
continence but avoids permanent urinary retention. Urinary retention is
a well-known potential complication of suburethral sling surgery (1).
Our technique is simple and has yielded excellent results with regard
to continence and retention. The rate of new-onset urgency compares well
with other studies (1,12). The association and causes of urgency after
anti-incontinence procedures have been discussed in the literature and
are not within the scope of this report (1,9,12); nevertheless, a technique
that minimizes permanent urinary retention may reduce partial obstruction
as well. This approach removes any emotionality from determination of
sling tension and is devoid of the need for any intellectual exercise
or special equipment during that portion of the surgery. Placement of
the patient in the reverse Trendelenburg position shifts the abdominal
contents into a more dependent position in the pelvis and may limit the
potential inadvertent oversupport of the urethra by the sling. Cystoscope
rotation has provided a method of determining intraoperative sling tension
with good results, but it does add an operative step, with the need for
urethral angle assessment, and a measure of subjectivity.
It would be difficult to tie the sutures
any more loosely than with this method, yet there was minimal postoperative
SUI. We did not alter surgical methods for urethral hypermobility and
intrinsic sphincter deficiency and still were successful. The proximal
urethral pressures after a suburethral sling have been reported to be
approximately 10 cm H2O (15), with the sling increasing the closing pressure
in the urethra just beneath the sling by only 5 to 6 cm H2O (16). Perhaps
this amount of suburethral sling support can be achieved by just removing
the slack from the suspension sutures, and this is truly all the tension
that is needed.
CONCLUSION
This method of adjusting sling tension should be considered secondary to its ease of performance while providing acceptable surgical results. It allows the surgeon to place the sling with no undue tension in a reproducible and satisfactory fashion.
REFERENCES
- Chaikin DC, Rosenthal J, Blaivas JG: Pubovaginal fascial sling for all types of stress urinary incontinence: long-term analysis. J Urol, 160: 1312, 1998.
- Raz S, Stothers L, Young GP, Short J, Maraks B, Chopra A, Wahle GR: Vaginal wall sling for anatomical incontinence and intrinsic sphincter dysfunction: efficacy and outcome analysis. J Urol, 156: 166, 1996.
- Blaivas JG, Jacobs BZ: Pubovaginal fascial sling for the treatment of complicated stress urinary incontinence. J Urol, 145: 1214, 1991.
- Morgan JE, Heritz DM, Stewart FE, Connolly JC, Farrow GA: The polypropylene pubovaginal sling for the treatment of recurrent stress urinary incontinence. J Urol, 154: 1013, 1995.
- Kaplan SA, Santarosa RP, Te AE: Comparison of fascial and vaginal wall slings in the management of intrinsic sphincter deficiency. Urology, 47: 885, 1996.
- Yamada T, Kura N, Kawakami S, Watanabe T, Negishi T, Mizuo T: Suburethral sling procedure for urinary stress incontinence: with special reference to determination of tension of suspension from posturethrovesical angle measured by ultrasonography [Japanese]. Nippon Hinyokika Gakkai Zasshi, 81: 1351, 1990.
- Sirls LT, Leach GE: Use of Fascia Lata for Pubovaginal Sling. In: Raz S (ed.). Female Urology, 2nd ed. Philadelphia, WB Saunders Company, pp. 376-381, 1996.
- McGuire EJ, Lytton B: Pubovaginal sling procedure for stress incontinence. J Urol, 119: 82, 1978.
- Rovner E S, Ginsberg DA, Raz S: A method for intraoperative adjustment of sling tension: prevention of outlet obstruction during vaginal wall sling. Urology, 50: 273, 1997.
- Rovner ES, Wein AJ: Sling Tension for Stress Incontinence Surgery. In: Issues in Incontinence. vol. 3, no. 2, pp. 1-6, 1997.
- Ogundipe A, Rosenzweig BA, Karram MM, Blumenfeld D, Bhatia NN: Modified suburethral sling procedure for treatment of recurrent or severe stress urinary incontinence. Surg Gynecol Obstet, 175: 173, 1992.
- Cross CA, Cespedes RD, McGuire EJ: Our experience with pubovaginal slings in patients with stress urinary incontinence. J Urol, 159: 1195, 1998.
- Petrou SP: Use of the Cobb-Ragde needle in pubovaginal sling surgery. Tech Urol, 1: 136, 1995.
- Pettit PD, Petrou SP: The value of cystoscopy in major vaginal surgery. Obstet Gynecol, 84: 318, 1994.
- McGuire EJ, O’Connell HE: Surgical treatment of intrinsic urethral dysfunction. Slings. Urol Clin North Am, 22: 657, 1995.
- McGuire EJ, Wan J: Pubovaginal Slings. In: WG Hurt (ed.). Urogynecologic Surgery. Gaithersburg, Aspen Publishers, pp 98-99, 1992.
____________________
Received: July 28, 2000
Accepted after revision: March 30, 2001
_______________________
Correspondence address:
Dr. Steven P. Petrou
Department of Urology, Mayo Clinic
4 500 San Pablo Road
Jacksonville, Florida, 32224, USA
Fax: + + (1) (904) 953-2218
E-mail: petrou.steven@mayo.edu