MALIGNANT
MESOTHELIOMA OF THE TUNICA VAGINALIS
(
Download pdf )
KÁTIA R. M. LEITE, WILLIAM C. NAHAS, LUIZ H. CAMARA-LOPES
Laboratory of Molecular and Surgical Pathology, Sírio Libanês Hospital, São Paulo, SP, Brazil
ABSTRACT
Malignant
mesothelioma of tunica vaginalis is a rare and aggressive neoplasm. It
occurs in 55 to 75-year-old men, but 20% of the 76 cases reported affected
patients in the first 3 decades. It presents as hydrocele and tumor mass,
and the preoperative diagnosis is made only in 3% of the cases. The orchiectomy
should be the first choice for treatment and adjuvant radio and chemotherapy
are indicated only in disseminated disease. Age over 60 and dissemination
previously to the diagnosis are the worst prognostic parameters. Local
recurrence, followed by inguinal and iliac lymph node metastasis, are
the most frequent outcome. Metastasis to other organs are very rare. The
median survival rate is 23 months.
We report a case of malignant mesothelioma
of the tunica vaginalis, epithelial type, affecting a 74-year-old man
treated by inguinal orchiectomy, which developed local recurrence 2 months
after surgery.
Key words:
testis; tumor; testicular neoplasms; tunica vaginalis; mesothelioma
Braz J Urol, 28: 135-137, 2002
INTRODUCTION
Only 76 cases of malignant mesothelioma of the tunica vaginalis have been reported in the English literature. Although the typical tumor affects men between 55 and 75 years of age, 10% of patients are younger than 25. Previous exposure to asbestos is reported in 40% of the patients. A firm mass may be palpated, often associated with hydrocele. In 75% of the cases microscopic examination reveals epithelial, papillary mesothelioma. The outcome is unfavorable and the median survival is 23 months, besides any adjuvant therapy (1-3). We report a case of malignant mesothelioma of tunica vaginalis in a 74-year-old man treated with orchiectomy that developed precocious local recurrence, only 2 months after surgery.
CASE REPORT
A
74-year-old man presented with an ill-defined firm mass in the left testicle,
which had developed within the last 3 months. In 1995 the patient was
submitted to herniorrhaphy, and 6 months later to hydrocelectomy, and
no lesion was detected at that time. There were no other urological or
systemic symptoms. The physical examination revealed a firm mass infiltrating
the testicular parenchyma. The left inguinal orchiectomy was done, after
occlusion of the vascular pedicle. Gross examination revealed a multinodular,
firm, whitish mass, 5.5 cm in diameter, infiltrating the distal portion
of the spermatic cord, extending to the epididymis and infiltrating the
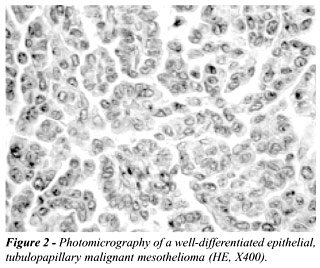
testicular parenchyma (Figure-1). The histology showed a well-differentiated
epithelial mesothelioma, tubulopapillary type, infiltrating the spermatic
cord, and extending to the epididymis and testicular parenchyma (Figure-2).
The mitotic index was high (3/10 high power field - HPF), and focal necrosis
was seen. Immunohistochemistry showed strong positivity of tumor cells
for antibody anti-cytokeratins (AE1-AE3; Dako, Carpinteria, CA, USA),
and no expression of CEA (Dako). The surgical margins were free of tumor.
Therefore, the resection was considered complete, and no other therapy
was introduced. Two months after surgery, a subcutaneous nodule was detected
at the scrotal wall. It was, at first, partially resected and the histology
revealed a well-differentiated epithelial mesothelioma, with the very
same microscopic aspect of the previous tumor. After diagnosis a hemiscrotectomy
was performed.

COMMENTS
The
age and presentation, as well as a disseminated disease, are the most
important prognostic parameters in this rare neoplasia. A review published
by Plas et al. (1) showed a median survival of 23 months for a group of
73 malignant mesotheliomas of tunica vaginalis reported in 30 years. Recurrence
occurred in 52.5% of the cases and it decreased survival to 14 months.
Approximately 20% of cases occurred in patients in the first 3 decades.
The prognosis is better for this group of patients.
The epithelial type mesothelioma accounts
for 75% of tumors and florid mesothelial hyperplasia is the first differential
diagnosis. The later is a benign lesion, and the tumor mass formation
excludes this entity. Clinical profile of carcinoma of the rete testis
overlaps with malignant mesothelioma, and both tumors have papillary and
tubular patterns. The location of the tumor within the rete testis, the
evidence of continuity with rete testis and the positivity for CEA at
immunohistochemistry are important to distinguish these 2 lesions.
Inguinal orchiectomy is the first-line surgical
approach, and adjuvant therapy has been indicated only in patients with
disseminated disease. Radiotherapy and different regimes of chemotherapy
have been given and no remission was achieved. Sixty percent of recurrences
occur within 2 years of follow-up, and local recurrence was reported in
23.7% of patients, with scrotal skin involvement in 10% of the cases.
The involvement of inguinal or iliac lymph nodes occurs in 3 to 5% of
the cases and the need of their dissection is still a matter of discussion.
Visceral metastasis are rare and the involvement of lung and liver is
reported in 10% and 4%, respectively.
REFERENCES
- Plas E, Claus RR, Pflüger H: Malignant mesothelioma of the tunica vaginalis testis. Review of the literature and assessment of prognostic parameters. Cancer, 83: 2437-2446, 1998.
- Butnor KJ, Sporn TA, Hammar SP, Roggli VL: Well-differentiated papillary mesothelioma. Am J Surg Pathol, 25: 1304-1309, 2001.
- Ulbright TM, Amin MB, Young RH: Miscellaneous Primary Tumors of The Testis, Adnexa, and Spermatic Cord. Hematopoietic Tumors. Secondary Tumors. In: Rosai J (ed.). Atlas of Tumor Pathology. Tumors of the Testis, Adnexa, Spermatic Cord and Scrotum. Washington DC, AFIP, pp. 247-253, 1999.
_________________________
Received: December 10, 2001
Accepted after revision: March 3, 2002
_______________________
Correspondence address:
Dr. Katia Ramos Moreira Leite
Rua Dona Adma Jafet, 91
São Paulo, SP, 01308-050, Brazil
Fax: + + (55) (11) 3231-2249
E-mail: katiaramos@uol.com.br