CAVERNOUS
LYMPHANGIOMA OF THE PREPUCE
(
Download pdf )
LUIS LLANES, PATRICIA ORTEGA, ALVARO PAEZ, ANTONIO BERENGUER
Departments of Urology and Pathology, Getafe University Hospital, Madrid, Spain
ABSTRACT
We report a rare case of a benign vascular tumor of the prepuce (cavernous lymphangioma) in a young man. Because of its location, it may be misdiagnosed as a far more common cystic lesion of the penis (median line cysts, mucoid cysts or epidermal cysts). This entity should be considered in the differential diagnosis of preputial masses.
Key words:
penis; penile neoplasms; lymphangioma.
Braz J Urol, 28: 138-139, 2002
INTRODUCTION
The described vascular lesions of the penis are hemangioma, angiokeratoma, venous lakes, angiolymphoid hyperplasia and lymphangioma. We report on a case of an unusual benign lymphatic tumor of the prepuce.
CASE REPORT
A
20-year-old man presented with a soft lesion in the dorsal area of the
prepuce. He did not complain of any other urological symptom. The medical
history was unremarkable and the physical examination showed a soft fluctuant
mass with liquid content in the dorsal aspect of the prepuce.
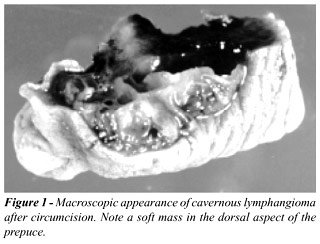
Under local anesthesia, the patient underwent
a circumcision because of the impossibility to resect the lesion (Figure-1).
The macroscopic examination of the specimen showed a multicystic lesion
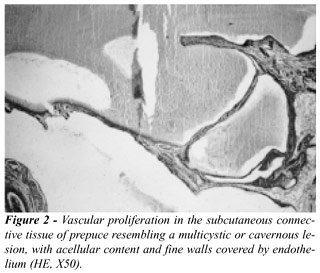
with fine walls. Microscopic study revealed a vascular proliferation containing
acellular material without any hematological elements (Figure-2). These
findings were concordant with the diagnosis of cavernous lymphangioma.
DISCUSSION
Lymphangiomas
are relatively rare tumors. In fact, it is difficult to state the nature
of lymphangiomas as true tumors, hamartoms of lymphangiectasia. Nowadays,
lymphangiomas are considered lymphatic malformations not communicated
with the lymphatic system. Incidence is slightly higher in males, and
the time of appearance is mainly in childhood, and in general before the
second year of life, although some cases have been described in adults.
Lymphangiomas are ubiquitous because of
the universal distribution of the lymphatic system, but the most common
affected sites are head, neck and axilla. Occasionally, they can occur
in deep organs such as lung, digestive tube, spleen, liver and bone. Lymphangiomas
have been classified in three groups: 1)- lymphangioma simplex or capillary
lymphangioma, composed of small thin-walled lymphatics; 2)- cavernous
lymphangioma, with large lymphatic vessels; 3)- cystic lymphangioma or
cystic hygroma, major lymphatic dilations lined with collagen and smooth
muscle, frequently diagnosed in newborns (1).
Cavernous lymphangiomas are often detected
in mouth, lips, cheek, tongue and other areas with dense connective tissue
and muscle, both allowing their expansion. They have also been denominated
deep cutaneous lymphangiomas because of their origin in the deep dermis
(2). Two cases of lymphangioma have been previously described in a genital
location: the glans of the penis, scrotum and retropubic space were affected,
and treatment was laser fulguration (2,3). The treatment of these lesions
must be individualized, specially according to their location. Laser fulguration
or local surgery are appropriate choices.
To our knowledge, this is the first case
ever reported of a cavernous lymphangioma of the prepuce. Hence, this
entity must be considered as another element in the differential diagnosis
of preputial masses together with the other cystic lesions of the penis
(median line cysts, mucoid cysts or epidermal cysts).
REFERENCES
- Enzinger FM, Weiss SW: Tumors of Lymph Vessels. In: Enzinger FM, Weiss SW (eds.). Soft Tissue Tumors. St. Louis, Mosby-Year Book, 3rd ed, chapt 26, 679-699, 1995.
- Forstner R, Hricak H, Kalbhen CL, Kogan BA, McAninch JW: Magnetic resonance imaging of vascular lesions of the scrotum and penis. Urology, 46: 581-583, 1995.
- Demir Y, Latifoglu O, Yenidunya S, Atabay K: Extensive lymphatic malformation of penis and scrotum. Urology, 58: 105-106, 2001.
_________________________
Received:
November 21, 2001
Accepted: December 11, 2001
_______________________
Correspondence address:
Dr. Antonio Berenguer
Department of Urology
Hospital Universitario de Getafe
Crta. Toledo km 12.500
28905, Getafe, Madrid, Spain
Fax: + + (34) (91) 683-3271
E-mail: luisllanes@airtel.net