VIRTUAL
COMPUTED TOMOGRAPHY CYSTOSCOPY IN BLADDER PATHOLOGIES
(
Download pdf )
HALIL ARSLAN, KADIR CEYLAN, MUSTAFA HARMAN, YUKSEL YILMAZ, OSMAN TEMIZOZ, SABAN CAN
Departments of Radiology and Urology, Yuzuncu Yil University School of Medicine, Van, Turkey
ABSTRACT
Objective:
Assessed the usefulness of virtual cystoscopy performed with multidetector
computed tomography (CT) in patients with different urinary bladder pathologies
compared to the conventional cystoscopy.
Materials and Methods: Eighteen patients
with different bladder pathologies, which consisted of 11 tumors, 3 diverticula,
2 trabecular changes and 2 stones, were assessed with conventional cystoscopy
and virtual CT cystoscopy. The results of virtual CT cystoscopy were compared
with the findings of conventional cystoscopy. We determined the detection
rate and positive predictive value of CT imaging based virtual cystoscopy
in the diagnosis of urinary bladder lesions.
Results: CT scanning was well tolerated
by all patients, and no complications occurred. Images in 16 (88%) of
the 18 virtual cystoscopic examinations were either of excellent or good
quality. All tumors except one, 2 trabecular changes and 2 stones were
characterized with similar findings in the both of methods. The masses
ranged from 0.4 to 7.0 cm in diameter. While conventional cystoscopy could
not evaluate interior part of the diverticulum, virtual CT cystoscopy
could demonstrate clearly within it. There were no false-positive findings
in our series.
Conclusion: Virtual CT cystoscopy is a promising
technique to be used in the detection of bladder lesions. It should be
considered especially at the evaluation of bladder diverticula. In the
future, it may be possible or even advantageous to incorporate into the
imaging algorithm for evaluation of bladder lesion.
Key
words: bladder; cystoscopy; tomography, spiral computed; tumors;
diverticula; stones
Int Braz J Urol. 2006; 32: 147-54
INTRODUCTION
Bladder
pathologies are consisted of the important group of genitourinary tract
diseases. The most common complaints in bladder disease are microscopic
and macroscopic hematuria, disuria and other voiding symptoms. All these
symptoms may be related to inflammatory, neoplastic, stones, neurologic,
obstructive or congenital abnormalities. Urogram, sonography (US), computed
tomography (CT), magnetic resonant imaging (MRI) and some other radiological
modality have been used for a long time in all these pathologies. However,
conventional cystoscopy is a standard diagnostic approach for urinary
bladder evaluation, its primary indication is the diagnosis of lower urinary
tract disease, sings, and symptoms that may be related to the urinary
tract are evaluated using cystoscopy to directly visualize lower urinary
tract anatomy and macroscopic pathology. However, this procedure has drawbacks,
including its high costs and an invasiveness that may lead to iatrogenic
bladder injury and urinary sepsis. CT is usually recommended as a useful
radiologic approach for assessing bladder disease, but CT has low sensitivity
for detection of small bladder lesions. For CT to depict a small bladder
lesion, optimal imaging conditions, including adequate bladder distention
and thin-slice scanning, must be satisfied. Therefore, negative findings
on CT warrant performance of conventional cystoscopy in patients with
bladder pathology (1-4).
Recently, three-dimensional computer-rendering
techniques with rapid image acquisition have led to the development of
virtual-reality imaging. With commercially available software, virtual
reality imaging allows interactive intraluminal navigation through any
hollow viscus, simulating conventional cystoscopy. This technique of virtual
endoscopy has been applied to many organs, including the colon, bronchus,
stomach, and bladder (3-6).
Currently, most authors have been studied
with virtual cystoscopy about the bladder tumor. Few reports are found
in the literature regarding different bladder pathology such as diverticulum
or inflammatory pseudotumor based virtual cystoscopy of the urinary bladder
(7,8).
The purpose of this study was to evaluate
the usefulness of virtual cystoscopy using a volume rendering algorithm
performed with multidetector CT in patients with different urinary bladder
pathology compared with the gold standard that is, conventional cystoscopy
and to determine the modality’s detection rate and positive predictive
value.
MATERIALS AND METHODS
Eighteen
patients (mean age 56 ± 11 years, range 40 to 72 years) were referred
from the urology department because of the different urinary bladder disease,
which consisted of 11 tumors, 3 diverticula, 2 trabecular changes and
2 stones for this study. We carried out both conventional and virtual
cystoscopy in all patients. Time interval between conventional and CT
cystoscopy ranged from zero to 7 days. Each patient had various clinical
histories. Most of the patients presented painless hematuria or dysuria.
Conventional cystoscopies were carried out with unaware of virtual cystoscopic
findings. The conventional cystoscopies were performed with rigid 21F
cystoscope (Storz, Germany) with a field of view of 30 degrees in all
patients under general or local anesthesia. Virtual cystoscopic examinations
were started with obtaining adequate bladder distention in supine position.
Helical CT was performed with 4 channel CT scanner (Somatom Sensation
4, Siemens Medical Systems, Erlangen, Germany), in single breath hold,
with 1 mm collimation, 1 mm reconstruction interval and 3 mm thickness.
Other scanning parameters were as follows: 1 mm reconstruction interval,
mAs 153, and 120 kV, feed/rotation 5 mm. The scanning time was only 8-12
second. Prior to the scan, adequate filling of the bladder with approximately
250-450 mL of air was required. At the same time, IV 100 mL contrast medium
was administered in all patients by a power injector at a rate of 2.0-2.5
mL/s for possible extravesical invasion of the tumor or some other pathology.
The patients were then turned to the prone position, and CT of the bladder
was repeated with use of the same parameters after a repeated scout view
was obtained. Additional bladder distention with approximately 80-120
mL of air was necessary in some of the patients, since repositioning led
to leakage of some of the insufflated gas from the bladder.
The data were downloaded to an independent
workstation (Leonardo; Siemens Medical Systems) equipped with software
for interactive intraluminal navigation. Using multiplanar reformation
from source images, a central observation point was defined in the middle
of the lumen of the bladder. The camera for virtual cystoscopy was placed
in the center of the bladder lumen and thereafter was advanced to each
quadrant in turn. When a possible abnormality was discovered, it was fully
evaluated from various angles.
The number, location, and size of the tumors
were individually determined and noted after cystoscopy for later comparison
with the results of CT imaging-based virtual cystoscopy. The virtual and
conventional cystoscopic findings for each patient were documented on
separate worksheets. The number, size, location, and morphologic features
of the masses, mucosal thickness, trabeculations and diverticula and other
luminal pathology were also noted in both methods. On transverse section
and virtual CT images obtained with the patients in both supine and prone
positions, each mass lesion was characterized as a focal polypoid lesion,
a sessile mass, or wall thickening. A discrete lesion was considered polypoid,
if it was taller rather than wider, while a sessile mass was defined as
a lesion when it was wider at the base. A lesion was characterized as
wall thickening when there was elevation of the bladder wall without a
discrete mass. The quality of each CT image was also evaluated in terms
of the residual urine, which may obscure the bladder mucosa, and the degree
of distention. Complications due to CT cystoscopy were recorded.
Three radiologists (HA,MH,OT) blinded to
the findings of conventional cystoscopy, independently interpreted the
images prospectively, and any discrepant readings were resolved by consensus.
The results of virtual CT cystoscopy were compared with the findings of
conventional cystoscopy, which is considered the standard. The lesions
that were not prospectively identified at CT cystoscopy were retrospectively
evaluated for visibility on transverse and virtual images. The pathology
report in each patient with bladder tumor was also reviewed for further
correlation. Using conventional cystoscopy as the gold standard, we analyzed
them to determine the detection rate of CT imaging-based virtual cystoscopy
in the diagnosis of urinary bladder lesions.
RESULTS
CT
scanning was well tolerated by all patients, and no complication occurred.
Images in 16 (88%) of the 18 virtual cystoscopic examinations were of
excellent or good quality, with adequate bladder distention and minimum
residual urine. Images in 2 examinations were suboptimal due to either
moderate residual urine or inadequate bladder distention. Tumoral lesions
were seen in one of them. However, in other patient, a smaller-than-4
mm polypoid tumoral lesion could not be detected.
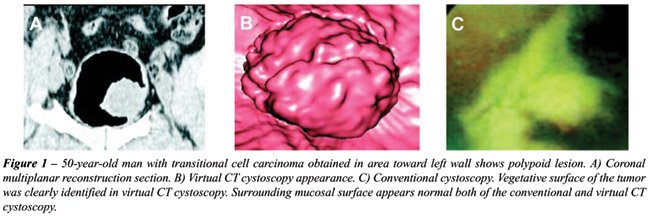
On conventional cystoscopy, 11 tumors were
found in 18 patients. These masses ranged from 0.4 to 7.0 cm in diameter
(mean, 1.5 cm). Out of 11 polypoid lesions, 8 were larger than 5 mm, and
3 were 5 mm or smaller. Eight out of the polypoid lesions were larger
than 5 mm, and 3 were 5 mm or smaller. One of the polypoid lesions was
calcified. Six out of the 11 lesions were located on the lateral wall
(Figures-1 and 2); 2 on the posterior wall; 2 on the anterior wall and
1 in the bladder neck. All lesions were diagnosed as transitional cell
carcinoma in the pathology reports. All these tumors had been described
by the virtual cistoscopy with nearly similar findings in size localization
and surface of the tumor except one lesion, which was smaller than 5 mm
90% of the tumors were diagnosed by virtual cystoscopy as compared to
conventional cystoscopy. Mucosal thickness and trabeculations were also
seen in the virtual CT cystoscopy and the appearance was similar in both
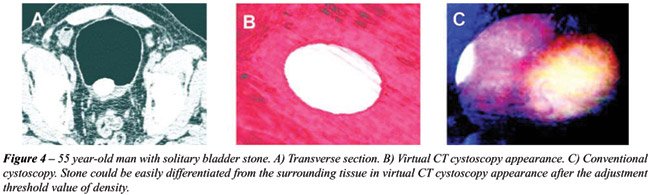
modalities (Figure-3). Bladder stone could not differentiate the tumor
or polyp without adjustment of the lowest and highest point of the density
value in the volume-rendering method in two patients (Figure-4).


Three diverticula were diagnosed, but the
interior of the diverticula could not be evaluated by conventional cystoscopy.
Their lumens were easily detected by virtual cystoscopy. In three diverticula,
virtual CT cystoscopies were superior to conventional cystoscopy in demonstration
of the interior of the diverticula (Figure-5).

Transverse section and virtual CT images
were complementary in lesion detection and characterization. Although
areas of wall thickening and trabeculation were seen on the virtual images,
they were more conspicuous on the transverse views. However, the lobulated
morphologic characteristics of a small polypoid lesion were better depicted
on the virtual image. There were no false-positive findings in our series.
The presence of every lesion seen at virtual cystoscopy was confirmed
at conventional cystoscopy. Virtual cystoscopy time, including catheter
placement, was approximately 20-25 minutes. Considering conventional cystoscopy
to be the gold standard, we found the following diagnostic values for
the identification of bladder lesions on virtual cystoscopy. In 17 out
of 18 patients (94.4%), lesions were detected by using virtual CT cystoscopy.
COMMENTS
Several
imaging techniques are available for use in the detection of bladder pathology.
US, urogram, CT, MRI and conventional cystoscopy could be used in the
bladder disease. Conventional cystoscopy was accepted as a gold standard
in bladder (3,5). However, there are several disadvantages of the conventional
cystoscopy. It is often difficult to perform adequately when exploring
the anterior bladder wall or a diverticulum cavity. Primary intradiverticular
carcinomas are rare, but diagnosis is often difficult with conventional
method (6,9,10,11). There are some contraindications for the conventional
cystoscopy such as bacteriuria, acute cystitis, urethritis, prostatitis,
obstructive prostatic hypertrophy, and stricture or rupture of the urethra.
Marked hematuria is another factor that limits the technical success of
cystoscopy, thereby decreasing its reliability. On the other hand, cystoscopy
is performed in general or local anesthesia and it is an invasive and
uncomfortable procedure for patients, and complications such as infections,
uretral or bladder perforation, scarring, and stricture of the urethra
have been observed (3,6,12-14).
Virtual endoscopy is a recently developed
noninvasive method to detect tumors protruding from the walls of hollow
organs. A promising advantage of this imaging modality is that views not
possible in conventional endoscopic examination can be created. The volumetric
data obtained with helical CT or MR imaging are computer-rendered to generate
three-dimensional images, and with commercially available software, intraluminal
navigation through any hollow viscus is possible. There are two main techniques
for the reconstruction of virtual image. One of them is volume rendering
and the other is surface-rendering algorithm. Of the different three-dimensional
rendering techniques available, the perspective volume rendering provides
more information because the entire data set is incorporated (15-19).
We used a volume-rendering algorithm in this study.
Virtual endoscopy has been most widely applied
to imaging of the colon and many investigators report its feasibility
in the depiction of colorectal polyps (20,21). After the first report
of virtual cystoscopy, in the study by Vining at al., there have been
a lot of studies on the utility of virtual cystoscopy of the bladder.
The urinary bladder is a good candidate for virtual cystoscopy because
of its simple luminal morphology, its relatively small volume, and the
absence of involuntary peristalsis. Therefore, a virtual cystoscopic rendering
of the bladder takes a short time to navigate and does not require great
skill on the part of the operator (4-6,18). On the other hand, according
to a study by Kim et al., virtual cystoscopy was found superior than multiplanar
reconstruction and source CT images for lesion detection in the contrast
material-filled bladder (22). However, most studies were performed in
bladder tumor and previous studies have focused solely on known bladder
lesion. There have been no enough studies on different pathologies. We
carried out this study on different bladder pathologies and evaluated
the capabilities of virtual cystoscopy, such as diverticula, trabeculation
and stone.
As a minimally invasive procedure, virtual
CT cystoscopy provides many advantages as compared to conventional cystoscopy.
The virtual CT cystoscopy images could be stored in file and the lesion
could be compared in follow up period with based images. The size of a
tumor is measured objectively. Access to the anterior bladder wall or
the lumen of a diverticulum is not restricted in virtual cystoscopy because
various software reconstruction tools can be used and the tumor can be
easily detected (23). Patients with a severe urethral stricture or marked
prostatic hypertrophy, who may be poor candidates for conventional cystoscopy,
can safely undergo virtual CT cystoscopy. It is also indicated for patients
who are at risk of complications such as hemorrhage, perforation, infection,
or pain, and for the examination of young patients (3,5,6). In our group,
diverticula were very well examined by virtual CT cystoscopy while conventional
cystoscopy could not evaluate the interior of lesions. However, we had
some difficulties in bladder stone using virtual cystoscopy. It was very
difficult to differentiate the polyp without setting the threshold density
value. This also showed us that axial images and virtual cystoscopy images
should be evaluated together.
Two techniques have been used to obtain
the CT source data for reconstructed virtual cystoscopic images, scanning
the bladder that has been filled with either air or contrast material.
Both methods have some advantages and disadvantages when compared with
one another. Most previous studies have been chosen to scan the air-filled
bladder. However, virtual cystoscopy of the air-filled bladder is inherently
invasive because catheterization is required to introduce air into the
bladder. Supine and prone examination is another disadvantage of the air-filled
bladder method. On the other hand, filling the bladder with IV contrast
material has been easily achieved in many studies. In this method, there
is no need for examination in prone and supine position. Therefore, this
means lesser radiation and cost (3,22). However, urine and contrast could
not be mixed properly with this method for virtual cystoscopy. This is
one of the disadvantages. Secondly, IV contrast application is mandatory
and this is another difficulty. Waiting for bladder filling and inadequate
distention is another disadvantage. In addition to these disadvantages,
possible scheduling problems may arise in a busy CT practice because of
the repeated patient positioning and scanning required (3,4,5). In our
study, like many others, we used air-filled bladder for virtual cystoscopy.
If there is already a Foley catheter inside the bladder, the air-filled
bladder method might be preferable. However, when there is no catheter
and a IV contrasted examination has already been planned, the second method
can be used for virtual cystoscopy.
Virtual cystoscopy has several limitations.
A major limitation is that it is unable to depict flat lesions, which
appear as subtle mucosal color changes on conventional cystoscopy. However,
various factors influence the detection of sessile lesions, including
the method used to acquire the CT data, interactive navigational skill
of the operator, attenuation-coefficient ranges used for voxel categorization,
and degree of bladder distention. Sessile lesions usually have an irregular
surface that must be minutely depicted on virtual cystoscopy. So if the
examination parameter is appropriate and distention is adequate, sessile
lesions also could be easily detected. Secondly, the differentiation between
small tumors and inflammatory swelling of the mucosa could be difficult,
especially in patients with unsatisfactory bladder filling. Inflammatory
swelling of the mucosa thus could be misdiagnosed as a tumor, or small
tumors could be missed on virtual cystoscopy. Insufficient distention
of the bladder may also cause the mucosa to wrinkle. Third, mucosal thickening
secondary to fibrosis cannot be distinguished from a neoplasm. Of course,
one faces a similar problem on conventional cystoscopy because biopsy
is often required to determine whether a bladder lesion is inflammatory,
fibrotic, or neoplastic. A fourth disadvantage of virtual cystoscopy is
that it lacks the ability to provide tissue for histologic evaluation,
an ability that is possible on conventional cystoscopy and biopsy. Fifth,
it is difficult to visualize the lumen of the urethra as is routinely
done with conventional cystoscopy. However, it was reported that urethra
could also be evaluated by virtual cystoscopy (24).
In conclusion, virtual CT cystoscopy is
a promising technique for tumor and some other bladder lesions, such as
diverticula. Virtual CT cystoscopy is likely superior to demonstrate the
interior part of the diverticulum. Adequate bladder distention and analysis
of virtual images are required for optimal evaluation. This minimally
invasive method can be of value for screening, primary diagnosis and surveillance
of bladder lesions. Virtual CT cystoscopy may be indicated as a clinical
routine when conventional cystoscopy is contraindicated or restricted
in feasibility and interpretation or there is risk of hemorrhage, perforation,
or pain especially in young patients. In the future, it may be possible
or even advantageous to incorporate into the imaging algorithm for evaluation
of bladder lesion through continued development and advancement of hardware
and software. To determine the clinical value of virtual CT cystoscopy
in the different bladder pathology, however, larger prospective studies
in the general patient population are necessary.
REFERENCES
- Carter HB: Basic Instrumentation and Cystoscopy. Walsh PC, Retik BA,Vaughan ED, Wein AJ (eds.). Campbell’s Urology, Saunders, Philadelphia. 8 ed., 2002; vol. 1, pp. 111-21.
- Bernhardt TM, Schmidl H, Philipp C, Allhoff EP, Rapp-Bernhardt U: Diagnostic potential of virtual cystoscopy of the bladder: MRI vs CT. Preliminary report. Eur Radiol. 2003; 13: 305-12.
- Kim JK, Ahn JH, Park T, Ahn HJ, Kim CS, Cho KS: Virtual cystoscopy of the contrast material-filled bladder in patients with gross hematuria. AJR Am J Roentgenol. 2002; 179: 763-8.
- Vining DJ, Zagoria RJ, Liu K, Stelts D: CT cystoscopy: an innovation in bladder imaging. AJR Am J Roentgenol. 1996; 166: 409-10.
- Song JH, Francis IR, Platt JF, Cohan RH, Mohsin J, Kielb SJ, et al.: Bladder tumor detection at virtual cystoscopy. Radiology. 2001; 218: 95-100.
- Lammle M, Beer A, Settles M, Hannig C, Schwaibold H, Drews C: Reliability of MR imaging-based virtual cystoscopy in the diagnosis of cancer of the urinary bladder. AJR Am J Roentgenol. 2002; 178: 1483-8.
- Zantl N, Beer A, van Randenborgh H, Hartung R: Virtual endoscopy of the urinary tract. Urologe A. 2002; 41: 552-8.
- Sakamoto Y, Tanaka H, Kawabata G: Inflammatory pseudotumor of the urinary bladder diagnosed using 3D-CT cystoscopy. Hinyokika Kiyo. 2003; 49: 587-90.
- Durfee SM, Schwartz LH, Panicek DM, Russo P: MR imaging of carcinoma within urinary bladder diverticulum. Clin Imaging. 1997; 21: 290-2.
- Stephenson WT, Holmes FF, Noble MJ, Gerald KB: Analysis of bladder carcinoma by subsite. Cystoscopic location may have prognostic value. Cancer. 1990; 66: 1630-5.
- Baniel J, Vishna T: Primary transitional cell carcinoma in vesical diverticula. Urology. 1997; 50: 697-9.
- Bavetta S, Olsha O, Fenely J: Spreading sepsis by cystoscopy. Postgrad Med J. 1990; 66: 734-5.
- Mosbah A, Kane A, Zhani R, Hattab C: Iatrogenic urethral strictures of the male urethra. Acta Urol Belg. 1990; 58: 87-93.
- Golomb J, Waizbard E, Iellin A, Merimsky E: Recurrent bladder perforation in chronic irradiation cystitis. J Urol. 1986; 92: 47-8.
- Blezek DJ, Robb RA: Evaluating virtual endoscopy for clinical use. J Digit Imaging. 1997; 10(Suppl 1): 51-5.
- Rubin GD, Beaulieu CF, Argiro V, Ringl H, Norbash AM, Feller JF, et al.: Perspective volume rendering of CT and MR images: applications for endoscopic imaging. Radiology. 1996; 199: 321-30.
- Calhoun PS, Kuszyk BS, Heath DG, Carley JC, Fishman EK: Three-dimensional volume rendering of spiral CT data: theory and method. Radiographics. 1999; 19: 745-64.
- Yazgan C, Fitoz S, Atasoy C, Turkolmez K, Yagci C, Akyar S: Virtual cystoscopy in the evaluation of bladder tumors. Clin Imaging. 2004; 28: 138-42.
- Hopper KD, Iyriboz AT, Wise SW, Neuman JD, Mauger DT, Kasales CJ: Mucosal detail at CT virtual reality: surface versus volume rendering. Radiology. 2000; 214: 517-22.
- Hara AK, Johnson CD, Reed JE, Ahlquist DA, Nelson H, MacCarty RL, et al.: Detection of colorectal polyps with CT colography: initial assessment of sensitivity and specificity. Radiology. 1997; 205: 59-65.
- Chen SC, Lu DS, Hecht JR, Kadell BM: CT colonography: value of scanning in both the supine and prone positions. AJR Am J Roentgenol. 1999; 172: 595-9.
- Kim JK, Park SY, Kim HS, Kim SH, Cho KS: Comparison of virtual cystoscopy, multiplanar reformation, and source CT images with contrast material-filled bladder for detecting lesions. AJR Am J Roentgenol. 2005; 185: 689-96.
- Prando A: CT-virtual endoscopy of the urinary tract. Int Braz J Urol. 2002; 28: 317-22.
- Chou CP, Huang JS, Wu MT, Pan HB, Huang FD, Yu CC, et al.: CT voiding urethrography and virtual urethroscopy: preliminary study with 16-MDCT. AJR Am J Roentgenol. 2005; 184: 1882-8.
____________________
Accepted after revision:
January 25, 2006
_______________________
Correspondence address:
Dr. Halil Arslan
YYÜ Týp Fakültesi Hastanesi
Radyoloji Anabilim Dalý
Maras. Cad, 65200, Van, TURKEY
Fax: + 90 432-2167519
E-mail: drhalilarslan@hotmail.com
CT-cystoscopy
has been shown to be a very accurate technique since it is able to detect
lesions larger than 0.5 cm and is able to show mucosal abnormalities as
small as 2 mm.
CT-cystoscopy
can be obtained either with gas-filled bladder or with contrast-material-filled
bladder. Usually the sensitivity of this technique is higher for the detection
of polypoid lesions in comparison with sessile lesions. In our institution
we routinely evaluate the axial images together with virtual images since
this combination, allows a significant increase in the overall sensitivity
of this technique.
Virtual
cystoscopy can also be obtained using magnetic resonance imaging (MR-cystoscopy).
MR-cystoscopy has some advantages over CT-cystoscopy since there is no
need for bladder catheterization or intravenous injection of contrast
material, but has lower spatial resolution (better for lesions larger
than 1 cm in diameter).
In
this report, 18 patients with bladder pathologies were evaluated by CT-cystoscopy
using distension of the bladder with gas after bladder catheterization.
All patients were evaluated in both prone and supine position. The size
of detected lesions ranged from 0.4 to 7.0 cm in diameter and there were
no false-positive findings.
Bladder
tumors can be noninvasively diagnosed using CT-cystoscopy or MR-cystoscopy,
since both give comparable views to conventional cystoscopy. Virtual cystoscopy
is helpful in cases where conventional cystoscopy is inconclusive or cannot
be performed. One of the strengths of this technique is to add diagnostic
information to conventional cystoscopy in the evaluation of bladder diverticula.
Tumor within bladder diverticulum with narrow lumen can be easily demonstrated
by virtual endoscopy.
Our
goal for the future is to improve spatial resolution of CT-cystoscopy,
reduce the radiation dose to the patient and provide useful information
in order to allow conventional cystoscopy guided by the ct-cystoscopic
findings.
_________________
Dr. Adilson Prando
Department of Radiology
Vera Cruz Hospital
Campinas, Sao Paulo, Brazil