RADICAL
NEPHRECTOMY AND NEPHROURETERECTOMY IN PATIENTS OVER 80 YEARS OLD
(
Download
pdf )
doi: 10.1590/S1677-55382010000200003
APOSTOLOS P. LABANARIS, VAHUDIN ZUGOR, AGAPI P. LABANARIS, POLYKANDRIOTIS ELIAS, REINHARD KÜHN
Department of Urology (APL, RK), Martha Maria Medical Center, Nuremberg, Department of Urology (VZ), St Antonius Hospital, Gronau, Department of Psychiatry (APL), Europakanal Medical Center, Erlangen, Department of Plastic and Hand Surgery (PE), University of Erlangen Medical Center, Erlangen, Germany
ABSTRACT
Purpose:
The aim of this study was to discover if elderly patients exhibit comparable
outcomes and survival benefits to those achieved in younger patients.
Materials and Methods: We assessed 35 patients over 80 years old treated
by radical nephrectomy or nephroureterectomy for malignant and inflammatory
conditions within the previous 4 years. A multivariate analysis regarding
survival and recovery was conducted and included various preoperative
parameters. The subjective opinion of patients or patient’s relatives
(in cases where the patient had past away) was estimated by answering
the following questions: (a) are you satisfied with your decision to undergo
the operation? (b) would you undergo it once more if needed? (c) would
you advise it to a patient your age?
Results: The median age was 83.5 years. Radical nephrectomy with a flank
approach was performed in 65.7% of cases and nephroureterectomy with a
transabdominal approach in 34.3% of cases. The median recovery was 13
weeks. During a median follow-up of 31 months (range 12 to 53), 80% of
patients were disease free. The remaining 20% passed away demonstrating
a median survival of 25 months (range 13-38). Eighty-eight percent of
patients were satisfied with their decision to undergo the operation,
91.4% would undergo it once more if needed and 91.4% would advise it to
a patient their age.
Conclusions: Radical nephrectomy and nephroureterectomy are safe and effective
in well-selected patients over 80 years old. Elderly patients exhibit
comparable preoperative outcomes and survival benefits to those achieved
in younger patients. Various preoperative clinical variables that effect
the survival of patients but not their recovery could be identified.
Key
words: renal neoplasms; morbidity; mortality; prognosis; convalescence;
patient satisfaction
Int Braz J Urol. 2010; 36: 141-50
INTRODUCTION
Improvements
in the healthcare delivery system and of medical interventions have resulted
in a significant increase of the average life span. As the population
ages, urologists are faced with the need to counsel older patients on
the risks and benefits of surgical procedures. Although the elderly present
with unique health-care challenges, currently available data indicate
that well-selected elderly patients do not have a significantly higher
risk of morbidity or mortality from major urologic surgery in comparison
to younger patients and can potentially gain survival benefits from surgery
(1). Nevertheless, three critical questions that arise are (a) are there
any preoperative clinical variables that effect survival? (b) are the
any preoperative clinical variables that could reveal the length of time
required in order for patients to resume usual physical activities? and
(c) do the patients themselves believe that they truly benefit from surgery?
The aim of the present study was to find answers to these questions and
additionally to do discover if elderly patients exhibit comparable preoperative
outcomes and survival benefits to those achieved in younger patients,
by analyzing a contemporary series of 35 patients over 80 years old treated
by radical nephrectomy or nephroureterectomy at our institution within
the previous 4 years.
MATERIALS AND METHODS
Between
April 2004 and September 2008, 35 consecutive patients over 80 years old
underwent radical nephrectomy or nephroureterectomy for inflammatory and
malignant conditions at our institution within the last 4 years. Patient
demographics as well as preoperative and postoperative data were recorded
in a computer database. The data were collected by chart review and telephone
interviews. The parameters assessed included: age, gender, reason of surgery
(curative or palliative treatment), type of surgery (radical nephrectomy
or radical nephroureterectomy with lymph node dissection), surgical approach
(flank or transabdominal), size of renal mass, symptoms (macrohematuria/pain/fever),
co-existing diseases (hypertension/diabetes/hypo or hyperthyroidism),
laboratory findings (anemia/leucocytosis/increase in serum creatinine
levels), median operative time, complication rates (intraoperative and
perioperative within 30 days), operative mortality (death within 30 days
of surgery), the length of hospital stay, survival, type of renal disease,
preoperative American Society of Anesthesiologists (ASA) score (2), preoperative
Karnofsky score (3), present Karnofsky score, length of time required
in order for patients to resume usual physical activities, and the subjective
opinion of patients or patient’s relatives (in patients who past
away) regarding the operation.
A multivariate analysis was conducted in order to detect possible preoperative
clinical variables that stratify patients likely to exhibit a prolonged
length of time required in order for them to resume usual physical activities
and that effect their survival. The analysis included the following parameters:
preoperative Karnofsky score, ASA score, symptoms, pathologic laboratory
findings, type of surgery (curative or palliative treatment) and type
of renal disease and stage. For comparison between 2 groups of continuous
values the Student-t-student test was used. For comparison between 3 or
more groups the one-way ANOVA with the Tukey correction for multiple comparisons
was used. For comparison of binomial values, the Chi-square test was used.
Simple linear regression was used to test the effect of one continuous
parameter against another. A p value of < 0.05 was considered significant.
The subjective opinion of patients or patient’s relatives regarding
the operation was estimated by answering the following questions: (a)
are you satisfied with your decision to undergo the operation? (b) would
you undergo the operation once more if needed? (c) would you advise such
a therapeutic approach to a patient your age?
RESULTS
Patient characteristics, as well as intraoperative and postoperative data, are presented in Table-1. The median age was 83.5 years (range 80-94). There were 20 male and 15 female patients. A total of 77.2% of patients underwent curative surgery and the remaining 22.8% palliative surgery. Radical nephrectomy with a flank approach was performed in 65.7% of cases and a radical transabdominal nephroureterectomy with a cuff of the bladder wall and lymph node dissection in 34.3% of cases. Lymphadenectomy typically included the para-aortic, paracaval, and interaortocaval nodes from the renal hilum to the bifurcation of the common iliac artery. All patients were routinely treated in an intensive care unit for 24 h after surgery. The median size of the renal mass was 5.2 cm (1.1-13.5 cm). A total of 40% of patients presented with symptoms (51.4% with intractable pain, 45.7 % with severe hemorrhage and 5.7% with signs of urosepsis), 48.5% with pathological laboratory findings and 51.5% presented with co-existing diseases. Para-neoplastic symptoms were not encountered in any of the patients. The median operative time for radical nephrectomy via a flank approach was 75 min. The median operative time for radical abdominal nephroureterectomy with lymph node dissection was 145 min. There were no intraoperative complications observed. Intraoperative blood transfusion was not required in any of the patients in this study. Postoperative complications were encountered in 14.3% of patients (1 case each: ileus, lactacidosis, hyperglycemia, pneumothorax and stroke). Postoperative patients (n = 3) received 2 U of packed red blood cells due to dilutional anemia in view of the patients’ advanced age and limited cardiac reserve. Operative mortality (14 days postoperative due to a stroke) was encountered in 1 patient (2.9%). The median hospitalization time was 14.2 days (8-30 days). No patients were re-hospitalized. The final pathology specimen revealed renal cell carcinoma (RCC) in 48.5% of patients, upper tract transitional cell carcinoma (TCC) in 34.3%, pyonephrosis in 11.4%, adrenal carcinoma in 2.9% and xanthogranulomatus pyelonephritis in 2.9% of patients. Only 1 patient exhibited positive surgical margins. Metastatic disease developed in 7.1% of patients (liver n = 2, lungs n = 2, bladder n = 1 and multiple n = 1). After a median follow-up of 31 months (range 12 to 53), 80% of the patients were still alive. The remaining 20% passed away and had a median survival of 25 months (13-38). A total of 71.5% of these patients died from an underlying oncological disease.

The median length of time required in order
for patients to resume their usual physical activities was 13 weeks (3-48
weeks). A total of 34.2% of patients were able to resume their regular
activities within 3-6 weeks, 34.2% in 8-12 weeks, 28.5% in 16-24 weeks
and 2.8% in 48 weeks.
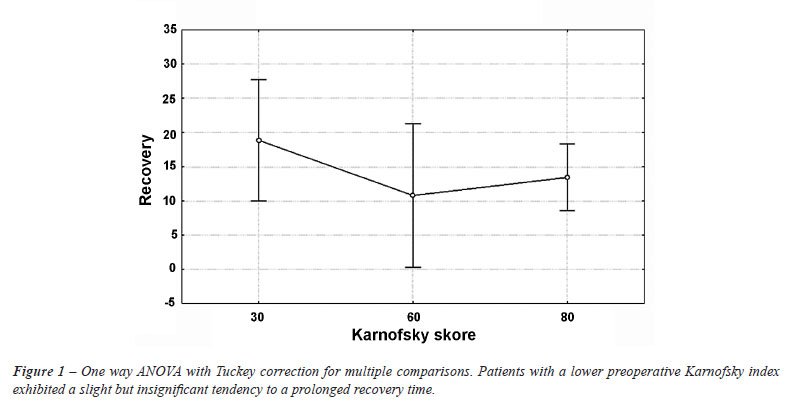
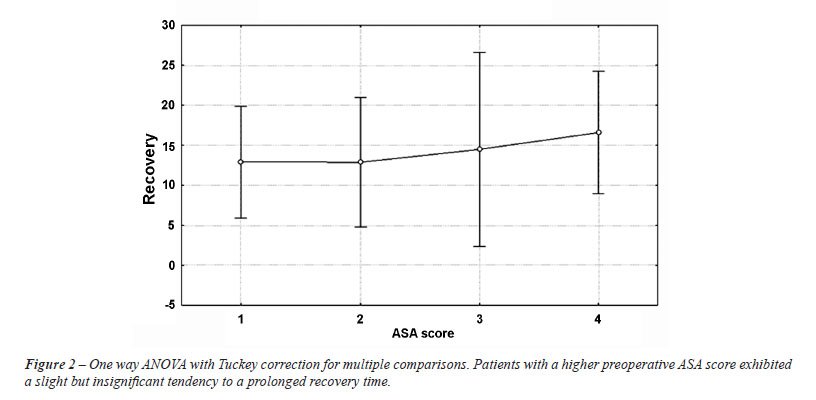
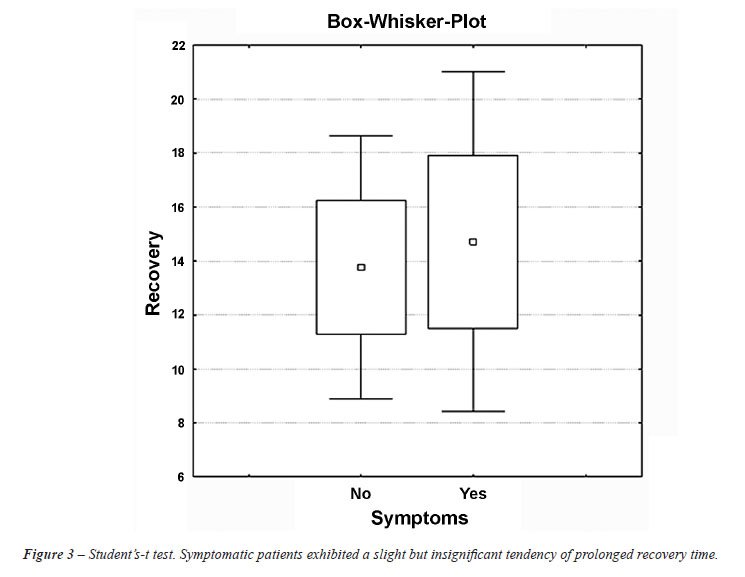
The multivariate analysis conducted in order
to detect possible preoperative clinical variables that stratify patients
likely to exhibit a prolonged length of time required in order for them
to resume usual physical activities demonstrated that: patients with a
preoperative Karnofsky index of 30-60 (Figure-1), patients with an ASA
score > 3 (Figure-2) and symptomatic patients (Figure-3) exhibited
a slight but insignificant tendency to a prolonged recovery time p = 0.19,
p = 0.18 and p = 0.10 respectively. Interestingly, there were no preoperative
clinical variables that significantly influenced the length of time required
in order for patients to resume to their usual physical activities.
The multivariate analysis conducted in order
to detect possible preoperative clinical variables that effect patient’s
survival demonstrated that: (a) patients with a high preoperative Karnofsky
score (80-100) exhibited a highly significant chance of having a prolonged
survival (30-60)-(80-100) p = 0.0001, (60-80)-(80-100) p = 0.016 (b) patients
with lower preoperative ASA score exhibited a highly significant chance
of having a prolonged survival ASA1: ASA3 p = 0.0088, ASA2: ASA3 p = 0.0211
and ASA2: ASA4: p = 0.0135. Asymptomatic patients, patients with non-pathologic
laboratory findings, patients who underwent a curative operation and patients
with a lower tumor stage exhibited a highly significant chance of having
a prolonged survival p = 0.0058, p = 0.0072, p = 0.0014 and p = 0.0028
respectively. There was no significant difference in survival of patients
with inflammatory disease when compared to patients with malignant disease
(Table-2).
As far as the subjective opinion of patients
or patient’s relatives regarding the operation, 88.5% were satisfied
with their decision to undergo the operation, 91.4% would undergo the
operation once more if needed and 91.4% would advise such an operation
to a patient their age.
COMMENTS
Elderly
patients have traditionally been viewed as poor candidates for urologic
surgery. However, a review of the literature regarding renal, prostate,
and bladder cancer supports what most urologists know intuitively: properly
selected elderly patients can safely undergo surgery and can, thereby,
potentially gain survival benefits (4).
Patients over 80 years old present with
unique health-care challenges, since they suffer from a higher incidence
of comorbid medical conditions, which make them less tolerant to perioperative
anesthetic, surgical stress, blood loss and postoperative complications
(5,6). Despite the risk of major surgery in these patients, radical nephrectomy
still remains the treatment of choice in many cases. Under inflammatory
conditions, surgical resection of the involved tissue and systemic antibiotic
administration are the primary mainstays of therapy regardless of age.
In advanced malignant disease nephrectomy is not only of palliative benefit,
to overcome pain, hemorrhage and paraneoplastic syndromes, but also has
the potential to increase overall survival (7).
The basic question is if radical nephrectomy
can be used as a curative treatment for malignant conditions in asymptomatic
patients over 80 years old. Considering the fair life expectancy of the
elderly and the excellent 5-year survival rates for local-stage RCC and
upper tract TCC, patients are likely to benefit from surgical treatment
regardless of their age (8). Lamb et al. (9), demonstrated the natural
history of RCC in the elderly by reporting on 36 patients medically unsuitable
for nephrectomy, with a median age of 76 years and a median tumor size
of 6.0 cm. None of the 13 patients who died during follow-up had deterioration
of the RCC, but in most cases the cause of death remained unclear. In
our patient group the median size of the renal mass was 5.2 cm, and the
average age was of 83.5 years. During a median follow-up of 31 months
only 20% (n = 7 patients) passed away and despite their tumor stage (T3-T4),
high ASA score (3-4) and low Karnofsky score (30-70) demonstrated a median
survival of 25 months.
Several recent studies showed that complications
of cancer surgery are no more common in the elderly than in younger patients
(10-16). Indeed, as demonstrated, postoperative complications were encountered
in 14.3% of patients with an operative mortality (14 days postoperative
due to a stroke) encountered in n = 1 patient (2.9%). Therefore, despite
the advanced age of the patients and high median ASA score (median score
3), the study group tolerated the procedure just as well as younger patients.
A critical consideration when contemplating major cancer surgery in the
elderly patient is often the length of time it would take for the patient
to resume usual physical activities (8). Valid concerns about the possible
adverse squeal of a prolonged period of convalescence and physical inactivity
on the suboptimal cardiovascular and musculoskeletal status of the elderly
are often arguments against performing major open cancer surgery in this
patient population (1). This was as well noted in the aforementioned patients.
The median length of time required in order for them to resume their usual
physical activities was 13 weeks (3-48 weeks). Interestingly, there were
no preoperative clinical variables that significantly influenced the length
of time required in order for patients to resume to their usual physical
activities. This can be partly explained due to the fact that 40% of patients
presented with symptoms and 22.8% underwent a palliative operation.
Although recovery time is a notable end
point, it should not minimize the importance of certain other needs of
elderly patients, including those who psychologically need to have their
cancers surgically removed. Most of the patients, even those who were
asymptomatic and demonstrated small lesions, had a strong desire to have
their tumors removed, as they did not wish to wait until progression that
might lead to a clinically significant disease.
The importance of age and comorbidity in
treatment decisions and survival outcomes has long been recognized in
oncology. However, tumor stage and grade remain the only variables on
which treatment decisions and outcome research are based. The aging process
is not uniform and patients show variable declines in organ function.
Some people at 75 years old might be as fit, if not more so, than others
at age 60 years (17). Although changes in some physiologic variables are
predictable, it is well recognized that there is more heterogeneity in
the elderly than in younger individuals (18). Thus, age is highly heterogeneous
from a clinical perspective and poorly reflected by chronological age.
Consequently, it is important to distinguish between fit and frail elderly
patients and not to judge solely based on chronological age when considering
suitability for cancer therapy (19). Indeed, the multivariate analysis
conducted in order to detect possible preoperative clinical variables
that effect patient’s survival demonstrated that patients with a
high preoperative Karnofsky score and a low preoperative ASA score exhibited
a highly significant chance of having a prolonged survival despite the
fact that their median age was 83.5 years old. This could somewhat justify
the fact that there was no significant difference of the survival of patients
with inflammatory disease when compared to patients with malignant disease.
Conservative management such as monitoring is of course an accepted treatment
alternative that has often been chosen for the elderly patient with associated
significant comorbidity. However, conservative treatments not infrequently
result in progressive local and systemic symptoms, which require repeated
hospitalization and ancillary procedures for palliation. Such a management
strategy may significantly compromise the quality of life of an 80-year-old
patient who could reasonably be expected to have 5 to 8 years of an active
lifestyle.
CONCLUSIONS
Radical nephrectomy and nephroureterectomy are safe and effective in well-selected patients over 80 years old. Although the delayed recovery time is an end point, it should not minimize the importance that patients themselves believe that they truly benefit from surgery since most of them are satisfied with their decision to have undergone the operation, would repeat it if necessary and would advise it to a patient their age.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Hsu TH, Gill IS, Fazeli-Matin S, Soble JJ, Sung GT, Schweizer D, et al.: Radical nephrectomy and nephroureterectomy in the octogenarian and nonagenarian: comparison of laparoscopic and open approaches. Urology. 1999; 53: 1121-5.
- American Society of Anesthesiologists: New classification of physical status. Anesthesiology 1963; 24: 111-4.
- Karnofsky DA, Burchenal JH: The clinical evaluation of chemotherapeutic agents in cancer. In: Macleod CM, (ed.), Evaluation of Chemotherapeutic Agents. 1st ed. New York, Columbia University Press. 1949: pp. 191-205.
- Liguori G, Trombetta C, Pomara G, Amodeo A, Bucci S, Garaffa G, et al.: Major invasive surgery for urologic cancer in octogenarians with comorbid medical conditions. Eur Urol. 2007; 51: 1600-4; discussion 1605.
- Tagle FM, Lavergne J, Barkin JS, Unger SW: Laparoscopic cholecystectomy in the elderly. Surg Endosc. 1997; 11: 636-8.
- Fried GM, Clas D, Meakins JL: Minimally invasive surgery in the elderly patient. Surg Clin North Am. 1994; 74: 375-87.
- Flanigan RC, Mickisch G, Sylvester R, Tangen C, Van Poppel H, Crawford ED: Cytoreductive nephrectomy in patients with metastatic renal cancer: a combined analysis. J Urol. 2004; 171: 1071-6.
- Orihuela E, Cubelli V: Management and results in elderly patients with urologic cancer. Semin Urol. 1987; 5: 134-40.
- Lamb GW, Bromwich EJ, Vasey P, Aitchison M: Management of renal masses in patients medically unsuitable for nephrectomy--natural history, complications, and outcome. Urology. 2004; 64: 909-13.
- Kashtan H, Werbin N, Wasserman I, Stadler Y, Wiznitzer T: Colorectal cancer in patients over 70 years old. A prospective study of operative results. Isr J Med Sci. 1992; 28: 861-4.
- Novotny V, Berdjis N, Hakenberg O, Leike S, Manseck A, Wirth M: Comparison of perioperative complications of diverse urinary diversions after radical cystectomy in elderly patients. EAU congress 2004; Abstract 597.
- Kingston RD, Jeacock J, Walsh S, Keeling F: The outcome of surgery for colorectal cancer in the elderly: a 12-year review from the Trafford Database. Eur J Surg Oncol. 1995; 21: 514-6.
- Paksoy M, Ipek T, Colak T, Cebeci H: Influence of age on prognosis and management of patients with colorectal carcinoma. Eur J Surg. 1999; 165: 55-9.
- Matin SF, Abreu S, Ramani A, Steinberg AP, Desai M, Strzempkowski B, et al.: Evaluation of age and comorbidity as risk factors after laparoscopic urological surgery. J Urol. 2003; 170: 1115-20.
- Ellis FH Jr, Williamson WA, Heatley GJ: Cancer of the esophagus and cardia: does age influence treatment selection and surgical outcomes? J Am Coll Surg. 1998; 187: 345-51.
- al-Sharaf K, Andrén-Sandberg A, Ihse I: Subtotal pancreatectomy for cancer can be safe in the elderly. Eur J Surg. 1999; 165: 230-5.
- Aapro MS: The frail are not always elderly. J Clin Oncol. 2005; 23: 2121-2.
- Wildiers
H, Highley MS, de Bruijn EA, van Oosterom AT: Pharmacology of anticancer
drugs in the elderly population. Clin Pharmacokinet. 2003; 42: 1213-42.
19. Anderson J, Van Poppel H, Bellmunt J, Miller K, Droz JP, Fitzpatrick JM: Chemotherapy for older patients with prostate cancer. BJU Int. 2007; 99: 269-73.
____________________
Accepted
after revision:
September 24, 2009
_______________________
Correspondence
address:
Dr. Apostolos P. Labanaris
Department of Urology
Martha Maria Medical Center
Stadenstrabe 58
Nürnberg, 90491, Germany
Fax: + 49 911 959-1352
E-mail: labanaris@web.de
EDITORIAL COMMENT
In the paper
by Labanaris et al., the authors evaluate the peri-operative morbidity
of radical nephrectomy and nephroureterectomy in a cohort of 35 patients
over the age of 80. On multivariate analysis, the authors noted that patients
with a pre-operative Karnofsky index of 30 to 60, patients with an ASA
score > 3, and symptomatic patients exhibited a slight but insignificant
tendency to prolonged recovery time. On multivariate analysis of predictors
of survival, pre-operative Karnofsky index, ASA score, absence of symptoms,
curative surgical resection, and normal (i.e. non-pathologic) laboratory
parameters predicted patient survival. Although this study addresses an
important clinical question, which is: should age and of itself preclude
surgical resection? This study is not sufficiently powered to address
this clinical question and the heterogeneity of the study population (including
varied indications for surgery including 4 patients having nephrectomy
for non-cancer related etiologies) is a significant limitation to the
present study. My clinical impression is that patient specific co-morbidities,
complexity of the surgical resection, and pre-operative medical optimization
may be more reflective of expected peri-operative morbidity. Clinicians
have at their disposal many clinical tools such as ASA score, ECOG (or
Karnofsky) performance status, and Charleston index to evaluate patient
surgical risk. The ultimate question in my view is how do these tools
specifically predict outcome in the specific patient population undergoing
renal extirpation surgery? To date, this question remains unanswered.
In conclusion, I caution clinicians using the numerical value of age as
a means of selecting patients suited for surgical resection. A more comprehensive
review of patient, disease, and surgery specific parameters is required
in assessing expected surgical risk and outcome.
Dr.
Philippe E. Spiess
Assistant Professor of Urology
H Lee Moffitt Cancer Center
Tampa, FL, USA
E-mail: Philippe.Spiess@moffitt.org
EDITORIAL COMMENT
The authors are to
be commended for examining this issue of extirpative radical surgery on
patients over the age of 80 years.
One has to be cautioned regarding the inevitable selection bias for this
type of single-center retrospective experience reporting, (as this was
not a prospective series of consecutive patients presenting with renal
cell carcinoma, but rather, this is a series of patients who had already
decided on surgery).
Patients with intractable pain, significant hemorrhage or manifestations
of para-neoplastic syndromes are more likely to be justified for surgery.
Although the authors are to be congratulated for their surgical skills
and efficiency, a routine extended lymphadenectomy in this age group and
clinical setting would not be recommended, in view of the controversial
issue of therapeutic or even diagnostic benefit of the lymphadenectomy.
The conclusion of “survival benefit” cannot be made in the
absence of a randomized trial of “surveillance” versus “intervention”.
In addition to “survival”, one needs to consider subsequent
post-operative “functionality”, physical and nephrologic.
The questionnaire attempts to address the former issue. However, a study
involving patients reporting on their experience needs to be interpreted
carefully because of reporting bias, albeit often inadvertent. Prolonged
recuperation, or exacerbation of any preexisting conditions because of
the surgery and anesthetic, would render radical surgery in this population
much less attractive and perhaps unjustified.
The authors rightly pointed out physiologic age rather than chronologic
age is more important. In addition to patient preference, the decision
to proceed with surgery in this elderly cohort (especially those who are
relatively asymptomatic), needs to take into account medical co-morbidities,
performance status and severity of symptoms.
Dr. Joseph
L. Chin
Professor of Urology & Oncology
Chair, Division of Surgical Oncology
University of Western Ontario
E-mail: Joseph.Chin@lhsc.on.ca