EARLY
EXPERIENCE WITH TARGETED THERAPY AND DENDRITIC CELL VACCINE IN METASTATIC
RENAL CELL CARCINOMA AFTER NEPHRECTOMY
(
Download pdf )
MARCOS F. DALL’OGLIO, JULIANA M. SOUSA-CANAVEZ, FABIO Y. TANNO, BRUNO C. TISEO, ALEXANDRE CRIPPA, SABRINA T. DOS REIS, KATIA R. M. LEITE, MIGUEL SROUGI
Division of Urology (MFDO, FYT, BCT, STR, KRML, MS), Medical School, University of Sao Paulo, Sao Paulo, Brazil, Genoa Biotechnology (JMSC), Sao Paulo, Brazil and Institute of Cancer of Sao Paulo (AC), ICESP, Sao Paulo, Brazil
Clinical Urology
Vol. 37 (2):
180-186, March - April, 2011
doi: 10.1590/S1677-55382011000200004
ABSTRACT
Purpose:
Metastatic renal cell carcinoma (RCC) is one of the most treatment-resistant
malignancies and nephrectomy, isolated or combined with systemic chemotherapy
typically has limited or no effectiveness. We report our initial results
in patients treated with the association of molecular targeted therapy,
nephrectomy, and hybrid dendritic-tumor cell (DC) vaccine.
Materials and Methods: Two male patients
diagnosed with metastatic RCC were selected for the study. They were treated
with the triple strategy, in which sunitinib (50 mg per day) was given
for 4 weeks, followed by radical nephrectomy after two weeks. DC vaccine
was initiated immediately after surgery and repeated monthly. Sunitinib
was restarted daily after 2 to 3 weeks of surgery with a 7-day interval
every 4 weeks.
Results: Both patients had complete adherence
to the proposed treatment with DC vaccine therapy combined with sunitinib.
Follow-up in these patients at 9 and 10 months demonstrated a stable disease
in both, as shown by imaging and clinical findings, with no further treatment
required.
Conclusion: The immune response obtained
with DC vaccine combined with the antiangiogenic effect of sunitinib and
the potential benefits of cytoreductive nephrectomy in advanced disease
could represent a new option in the treatment of metastatic RCC. Further
prospective trials are needed not only to elucidate the ideal dosing and
schedule, but also to better define the proof-of-concept proposed in this
report and its role in clinical practice.
Key
words: renal cell carcinoma, dendritic cells, neoplasm metastasis
Int Braz J Urol. 2011; 37: 180-6
INTRODUCTION
Renal
cell carcinoma (RCC), the most common type of kidney cancer, is commonly
asymptomatic in its early stages. Consequently, 25-30% of patients are
diagnosed with metastatic disease at initial presentation. The incidence
of RCC has grown at a rate of 3.7% in recent years (1). The etiology of
RCC is still widely unknown and the disease primarily affects men and
women in the fifth and sixth decades of life (2). It is characterized
by a lack of early warning signs and diverse clinical manifestations.
RCC has historically been a difficult malignancy to diagnose and also
to treat, because it remains clinically occult for most of its course.
It is often diagnosed incidentally following radiologic studies. In advanced
stages, treatment results are extremely poor, with response rates for
treated patients remaining between 5% to 10% and overall median survival
of less than one year (3). The US National Cancer Institute has estimated
approximately 15.7 years of life lost per-person dying (4). The cytoreductive
surgery (nephrectomy) and/or systemic treatment with cytotoxic chemotherapy
typically have limited or no effectiveness (5).
Recently, less-toxic molecular targeted
therapies have been the subject of clinical trials of advanced RCC, including
sorafenib and sunitinib, which have shown survival benefits for patients
with metastatic RCC. This strategy has become an important therapy option
with promising results, such as extending life and bringing quality of
life to these patients (6).
Dendritic cells (DC) are potent antigen-presenting
cells and effective initiators of an invasive response (7). The recent
development of DC in vitro has opened new possibilities for cancer therapy.
Kugler et al. were the first to demonstrate the possibility of DC to become
a tumor vaccine for metastatic RCC (8). More recently, significant responses
were reported in this disease stage with vaccines based on DC hybridized
with cells from the tumor itself (9,10). However, trials evaluating vaccine-based
therapies are still awaited. The use of vaccines in cancer, nonetheless,
will initially only be possible in a combined approach, in which current
strategies, surgery as a cytoreductive enhancer, and novel agents are
included (11).
Since the mechanism by which DC therapy
strongly stimulates the patient’s immunologic system greatly differs
from that of the targeted-drug by anti-angiogenic effect, we attempted
to assess the possible added or synergic combination of those two therapies.
We report on our initial experience with
patients treated with a multi-modality approach, in which we combined
a molecular targeted drug, cytoreductive nephrectomy, and hybrid DC vaccine.
MATERIALS AND METHODS
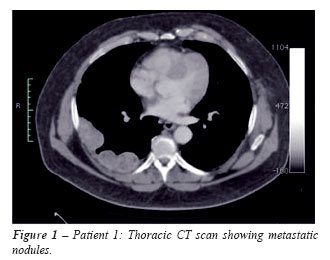
Two
male patients presenting renal masses and systemic metastasis at first
assessment were included in this analysis (Table-1).
By the time of diagnosis, the patients already had several distant metastatic
masses and bulky renal tumors on imaging studies (Figure-1). The treatment
was initiated with sunitinib (50 mg per day) before surgery for 30 days.
After two weeks, patients underwent radical nephrectomy. DC vaccine was
administered just after the surgery and monthly thereafter. The use of
sunitinib was restarted after 2 to 3 weeks of surgery (Table-1).
The DC vaccine was prepared and obtained
as previously described (9,10). In summary, peripheral blood mononuclear
cells were collected from healthy unrelated volunteers through apheresis,
after informed consent of donors. Mononuclear cells were separated further
with a density gradient, resuspended, and seeded in culture flasks in
RPMI 1640 culture medium. Then, flasks were incubated at 37ºC for
a period of 4 h, when nonadherent cells were removed, and the RPMI medium
was replaced by a serum-free medium containing GM-CSF (50 ng/mL; R&D,
Minneapolis, MN, USA) and interleukin 4 (50 ng/mL; R&D, Minneapolis,
MN, USA). After 5 days in culture, TNF-a (50 ng/mL; R&D, Minneapolis,
MN, USA) was added to the cultures for DC activation. After 2 further
days in culture, cells were harvested and used for the generation of the
dendritic-tumor hybrid vaccine. At the last day of DC cultures, DCs were
harvested, washed, and resuspended in a sterile 5% glucose solution at
a concentration of 1 107 cells/mL. Tumor cells were thawed, washed, and
also resuspended in a sterile 5% glucose solution at a concentration of
1 107 cells/mL. These two cell suspensions were mixed at equal volumes,
and cells were fused by an electric pulse. Shortly after fusion, all cells
stained with trypan blue. The hybrid cell preparation was centrifuged,
resuspended in 1-2 mL of sterile phosphate-buffered saline (pH 7.2) and,
after irradiation (200 Gy), injected in the patients. At this moment,
cell viability ranged from 60 to 80% of the initial tumor cell viability.
Vaccine injections were intradermic.
RESULTS
In
both patients, we observed stabilization of the lesions after sunitinib
was given. After radical nephrectomy, no surgical complications were observed
and complete wound healing occurred.
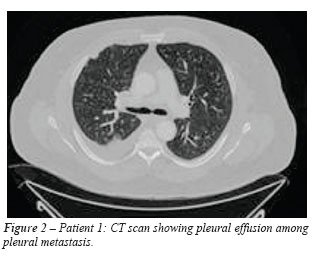
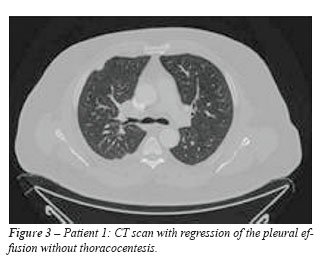
Patient 1 - Sixty days after surgery, we
observed a major decrease of pleural effusion and stabilization of lung
lesions (Figures 2 and 3). A 120-day control test repeated those findings
and showed a reduction of the right lung and pleural lesions. Complete
disappearance of the small left lung lesions was observed. The patient
continued clinical follow-up with stabilized lesions until the last visit,
with no new symptoms.
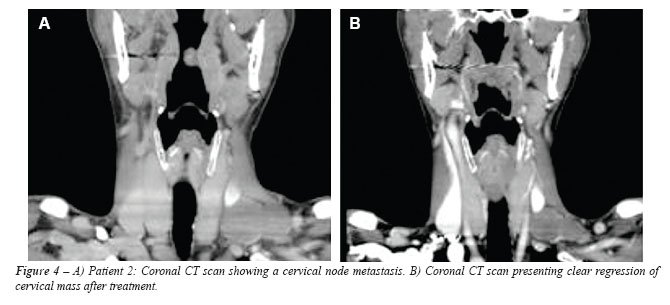
Patient 2 - We observed a partial regression
of the lung lesions as well as a significant and continuous decrease of
the cervical mass, as shown in Figure-4.
Until their last follow-up, both patients were kept on treatment with
DC vaccine therapy and the use of sunitinib daily, with a 7-day interval
every 4 weeks, with an apparent stable disease.
COMMENTS
Futures
strategies for the treatment of metastatic RCC will try to aggregate several
drug therapies to act on different pathways.
This treatment with DC has the advantage
of presenting minimum adverse events, providing a better quality of life
for patients, in contrast to the usual therapy with cytokines that, in
spite of presenting objective responses, is associated with serious side
effects, which can lead to poor quality of life or even death. DC initiates
an immune response and, nowadays, we can generate these cells in the laboratory,
providing a cancer therapy (7). Kugler et al. have published good results
with stabilization of renal metastatic lesions after the association of
surgical treatment with DC vaccines for metastatic RCC (8). A study with
DC vaccine alone, published by Barbuto et al. (10), for the treatment
of metastatic RCC showed stabilization of the disease in 71% of the patients
in median 6.7 months of follow-up (5-21 months).
The safety and effectiveness of these targeted
drugs are well documented in current literature with metastatic RCC stabilization
for about 5.5 to 11 months with sorafenib (12) and sunitinib (13), respectively.
The use of DC vaccine has also shown promising results in some reported
cases in the literature (9).
The use of DC vaccine in association with
targeted drugs is controversial and was first assumed that it could be
used with sunitinib alone, (14) although it could also be used with sorafenib
as demonstrated by Alfaro et al. (15).
The use of targeted therapy with DC vaccine
after nephrectomy in metastatic RCC disease has not yet been published.
It shows a possible synergy by those two approaches, leading to a more
promising anti-tumoral control using two distinct mechanisms of action,
in combination with a cytoreductive surgery.
Even though these multi-drug therapies for
metastatic RCC disease were a good and reasonable possibility, the combination
of sunitinib with sorafenib failed to prove its effectiveness (16). Despite
important progress in metastatic RCC after the introduction of targeted
therapy, clinically significant benefit is limited. Several issues still
remain unclear, lacking proper prospective clinical trials for an evidence-based
guideline (17).
Sunitinib is a tirosine kinase inhibitor with double action: antiproliferative
and antiangiogenic, (12) Bevacizumab is another inhibitor of angiogenesis
(18) and tensirolimus a specific inhibitor of the mammalian target of
rapamycin kinase (19). Apparently, any of these drugs could be used in
association with DC vaccine based on the Alfaro et al. study (15).
Cytoreductive nephrectomy in metastatic
RCC has shown benefits in a significant number of patients improving disease-specific
survival (20). These newly developed targeted-drug therapies may bring
new expectations for these patients with a poor life expectancy.
Until now, at ten months follow-up, we could
observe a regression of metastatic lesions and stabilization of the disease
in imaging tests with DC vaccine combined to a targeted-drug therapy.
This may represent a new and promising strategy of treatment for clinical
use, since median life expectancy for metastatic RCC using sunitinib alone
or interferon was 5.3 and 4 months, respectively, as reported by Motzer
et al. (21,22). Novel insights into immunology and biology of the tumor
have accelerated research on vaccines, which demonstrated significant
efficacy as antitumoral agents (23).
The immune response obtained with DC vaccine
associated with the antiangiogenic effect of sunitinib appear to present
a new horizon in the therapy of metastatic RCC pointing towards a new
option for treatment of a potential lethal disease as demonstrated in
this small series of cases.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ: Cancer statistics, 2009. CA Cancer J Clin. 2009; 59: 225-49.
- Murai M, Oya M: Renal cell carcinoma: etiology, incidence and epidemiology. Curr Opin Urol. 2004; 14: 229-33.
- Lam JS, Leppert JT, Belldegrun AS, Figlin RA: Novel approaches in the therapy of metastatic renal cell carcinoma. World J Urol. 2005; 23: 202-12.
- Ries LAG, Melbert D, Krapcho M, Mariotto A, Miller BA, Feuer EJ, et al.: Editors. SEER Cancer Statistics Review, 1975-2004. National Cancer Institute. Bethesda, MD, 2007. [Cited nov 2006]. Available at: http://seer.cancer.gov/csr/1975_2004.
- Motzer RJ, Russo P: Systemic therapy for renal cell carcinoma. J Urol. 2000; 163: 408-17.
- Rini BI, Campbell SC, Escudier B: Renal cell carcinoma. Lancet. 2009; 373: 1119-32.
- Banchereau J, Steinman RM: Dendritic cells and the control of immunity. Nature. 1998; 392: 245-52.
- Kugler A, Stuhler G, Walden P, Zöller G, Zobywalski A, Brossart P, et al.: Regression of human metastatic renal cell carcinoma after vaccination with tumor cell-dendritic cell hybrids. Nat Med. 2000; 6: 332-6. Retraction in: Kugler A, Stuhler G, Walden P, Zöller G, Zobywalski A, Brossart P, Trefzer U, Ullrich S, Müller CA, Becker V, Gross AJ, Hemmerlein B, Kanz L, Müller GA, Ringert RH. Nat Med. 2003; 9: 1221.
- Dall’Oglio M, Srougi M, Barbuto JA: Complete response of metastatic renal cancer with dendritic cell vaccine. Int Braz J Urol. 2003; 29: 517-9.
- Barbuto JA, Ensina LF, Neves AR, Bergami-Santos P, Leite KR, Marques R, et al.: Dendritic cell-tumor cell hybrid vaccination for metastatic cancer. Cancer Immunol Immunother. 2004; 53: 1111-8.
- de Reijke TM, Bellmunt J, van Poppel H, Marreaud S, Aapro M: EORTC-GU group expert opinion on metastatic renal cell cancer. Eur J Cancer. 2009; 45: 765-73.
- Hipp MM, Hilf N, Walter S, Werth D, Brauer KM, Radsak MP, et al.: Sorafenib, but not sunitinib, affects function of dendritic cells and induction of primary immune responses. Blood. 2008; 111: 5610-20.
- Escudier B, Eisen T, Stadler WM, Szczylik C, Oudard S, Siebels M, et al.: Sorafenib in advanced clear-cell renal-cell carcinoma. N Engl J Med. 2007; 356: 125-34. Erratum in: N Engl J Med. 2007; 357: 203.
- Motzer RJ, Hutson TE, Tomczak P, Michaelson MD, Bukowski RM, Rixe O, et al.: Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med. 2007; 356: 115-24.
- Alfaro C, Suarez N, Gonzalez A, Solano S, Erro L, Dubrot J, et al.: Influence of bevacizumab, sunitinib and sorafenib as single agents or in combination on the inhibitory effects of VEGF on human dendritic cell differentiation from monocytes. Br J Cancer. 2009; 100: 1111-9.
- Vogelzang NJ: Treatment options in metastatic renal carcinoma: an embarrassment of riches. J Clin Oncol. 2006; 24: 1-3.
- Heldwein FL, Escudier B, Smyth G, Souto CA, Vallancien G: Metastatic renal cell carcinoma management. Int Braz J Urol. 2009; 35: 256-70.
- Yang JC, Haworth L, Sherry RM, Hwu P, Schwartzentruber DJ, Topalian SL, et al.: A randomized trial of bevacizumab, an anti-vascular endothelial growth factor antibody, for metastatic renal cancer. N Engl J Med. 2003; 349: 427-34.
- Hudes G, Carducci M, Tomczak P, Dutcher J, Figlin R, Kapoor A, et al.: Temsirolimus, interferon alfa, or both for advanced renal-cell carcinoma. N Engl J Med. 2007; 356: 2271-81.
- Pierorazio PM, McKiernan JM, McCann TR, Mohile S, Petrylak D, Benson MC: Outcome after cytoreductive nephrectomy for metastatic renal cell carcinoma is predicted by fractional percentage of tumour volume removed. BJU Int. 2007; 100: 755-9.
- Motzer RJ, Bacik J, Murphy BA, Russo P, Mazumdar M: Interferon-alfa as a comparative treatment for clinical trials of new therapies against advanced renal cell carcinoma. J Clin Oncol. 2002; 20: 289-96.
- Motzer RJ, Hutson TE, Tomczak P, Michaelson MD, Bukowski RM, Oudard S, et al.: Overall survival and updated results for sunitinib compared with interferon alfa in patients with metastatic renal cell carcinoma. J Clin Oncol. 2009; 27: 3584-90.
- Kusmartsev S, Vieweg J: Enhancing the efficacy of cancer vaccines in urologic oncology: new directions. Nat Rev Urol. 2009; 6: 540-9.
____________________
Accepted
after revision:
July 27, 2010
_______________________
Correspondence
address:
Dr. Marcos F. Dall’Oglio
Rua Barata Ribeiro, 398 / 5º. Andar
Fax: + 55 11 3159-3618
São Paulo, SP, 01308-000, Brazil
E-mail: marcosdallogliouro@terra.com.br
EDITORIAL COMMENT
Renal
cell carcinoma is frequently asymptomatic in its early stages. As a consequence,
a high percentage of patients is diagnosed with metastatic disease at
initial presentation. In advanced stages treatment results are extremely
poor with an overall median survival of less than one year. Nephrectomy
and/or systemic treatment with cytotoxic chemotherapy have poor or no
effectiveness.
Recently, the use of molecular targeted
therapies have shown survival benefits for patients with metastatic renal
cell carcinoma. A new possibility is a consequence of the development
of dendritic cells in vitro which are potent antigen-presenting cells.
Some studies have shown significant response in metastatic disease using
vaccines based on dendritic cells hybridized with cells from the tumor
itself.
Dr. Dall’Oglio et al. report a novel
initial experience with two patients treated with multi-modality approach
combining a molecular targeted drug, cytoreductive nephrectomy, and hybrid
dendritic cell vaccine. Follow-up of 9 and 10 months have demonstrated
stable disease in both, as shown by imaging and clinical findings, with
no further treatment required.
This is a very promising result. We hope
that new trials with higher number of patients and longer follow-up confirm
the benefit in the immune response obtained with dendritic cell vaccine
combined with the antiangiogenic effect of sunitinib in the treatment
of metastatic renal cell carcinoma.
Dr. Athanase
Billis
Full-Professor of Pathology
State University of Campinas, Unicamp
Campinas, São Paulo, Brazil
E-mail: athanase@fcm.unicamp.br
EDITORIAL COMMENT
Renal
cell carcinoma (RCC) still is a major health problem and almost half of
the patients have locally advanced or metastatic disease at the time of
the diagnosis. Recently, targeting agents have demonstrated benefits in
progression free-survival and overall survival in patients bearing a metastatic
RCC. Currently, these drugs are recommended as first and second line standard
of care in metastatic RCC (1). But despite proven efficacy, complete response
is rarely seen. Therefore, new strategies and treatment modalities are
required to optimize RCC outcomes.
Several therapeutic strategies are under
investigation in urologic oncology. Urologists are familiar with immunotherapy,
since these interventions have long been utilized for kidney (IL-2, IFN
alfa) and bladder cancer (BCG) treatments. Theoretically, vaccinated patients
could develop an immune surveillance, able to lead either to a postponed
recurrence or prolonged cancer specific-survival. At present, therapeutic
potential of vaccines against metastatic RCC is limited as highlighted
by the authors. Nevertheless, metastatic RCC patients treated with DC
vaccines showed promising results in several phase I/II trials (2). In
an investigative scenario, considerable interest exists in simultaneous
delivery antiangiogenic drugs and vaccines. The tumor immune-suppressive
microenvironment could be a possible explanation to why tumors can evade
the immune system. Tyrosine kinase inhibitors might sinergically contribute
to restore the impaired tumor-mediated immune response and thereby improve
vaccine efficacy.
In the present report, a word of caution
must be emphasized to underline the major limitation of this combined
antitumor strategy. Since both patients received sunitinib, we cannot
confirm if the clinical response presented by these two patients was anyhow
impacted by the concomitant use of DC vaccine. Certainly, this issue can
only be addressed in a future phase 3 clinical trial.
REFERENCES
1.
Ljungberg B, Cowan NC, Hanbury DC, Hora M, Kuczyk MA, Merseburger AS,
et al.: EAU guidelines on renal cell carcinoma: the 2010 update. Eur Urol.
2010; 58: 398-406.
2. Van Poppel H, Joniau S, Van Gool SW:
Vaccine therapy in patients with renal cell carcinoma. Eur Urol. 2009;
55: 1333-42.
Dr. Flavio
L. Heldwein
Discipline of Urology
Univ. do Sul de Santa Catarina (UNISUL)
Florianopolis, SC, Brazil
E-mail: flavio.lobo@gmail.com