SURGICAL
TREATMENT OF METACHRONOUS METASTASES IN DIFFERENT ORGANS FOLLOWING RADICAL
NEPHRECTOMY
(
Download pdf )
CARLOS M. N. DE JESUS, LUIZ A. CORRÊA, JOSÉ C. S. TRINDADE FILHO
Department of Urology, Botucatu School of Medicine, Paulista State University, Botucatu, São Paulo, Brazil
ABSTRACT
Renal
clear cell carcinoma (RCCC) is a neoplasia resistant to radio and chemotherapy,
with surgical treatment being the procedure that is recognized for its
curative treatment. This case report demonstrates the success of an aggressive
surgical treatment for consecutive and late metachronous metastases following
radical nephrectomy.
Case report: Asymptomatic 50-year old man.
During a routine examination, an incidental mass was found by renal ultrasonography.
He underwent right radical nephrectomy due to RCCC in June 1992. During
the follow-up metastases were evidenced in cerebellum on the seventh year,
and in left lung and pancreas on the eighth year following the radical
nephrectomy, with all of them successfully treated by surgical excision.
Comments: The surgical excision of consecutive
and late metachronous metastases in different organs arising from RCCC
is feasible, being a good therapeutic alternative in selected cases.
Key
words: renal cell carcinoma; metastases; cerebellum; lung; pancreas;
surgery
Int Braz J Urol. 2003; 29: 238-40
INTRODUCTION
Renal clear cell carcinoma (RCCC) is a neoplasia resistant to radio and chemotherapy, with surgical ablation being the recognized method for its treatment with curative purposes. Radical nephrectomy is the gold standard for localized disease with tumors larger than 4 cm, with a 5-year survival ranging from 70 to 90% in theses cases (1). However, in metastatic disease there are few therapeutic alternatives, such as immunotherapy, with low success rates (2). This report presents a rare case with late and consecutive metachronous metastases of RCCC in different organs, successfully treated by surgical excision.
CASE REPORT
A
male, 50-year old, Caucasian, asymptomatic patient, during routine examination
was subjected to abdominal ultrasonography where an heterogeneous renal
mass was found in the superior pole of the right kidney, measuring 7 x
5 cm. An abdominal computerized tomography was performed and detected
a tumoral thrombus in the renal vein.
In June 1992, a right radical nephrectomy
was performed, and the histopathological examination identified a grade
II renal cell carcinoma in the superior pole, measuring 7.5 x 5 cm, with
tumoral thrombus in the renal vein. Ipsilateral perirenal fat, capsule
and suprarenal were free of neoplasia. Patient evolved post-operatively
without intercurrences and was followed in an outpatient basis every 6
months with physical examination, chest RX, and abdominal tomography.
On the seventh year of follow-up, the patient
suffered 2 episodes of syncope. A computerized tomography of the cranium
was performed and detected a 3 cm tumoral mass in the left side of cerebellum.
A craniotomy was indicated for exeresis of the mass with a histopathology
compatible with RCCC.
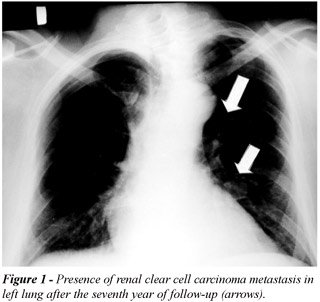
One year after follow-up, 2 nodules of 1
cm were observed in the left lung (Figure-1). Left thoracotomy with wedge
resection was indicated, evidencing grade II RCCC, compatible with previous
histopathological examinations.
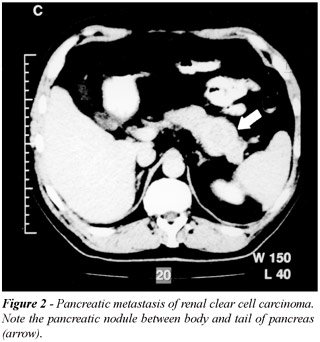
Finally, 6 months following thoracotomy,
in an abdominal ultrasound there was the suspicion of a 2 cm hypoechogenic
nodule in the body of pancreas. An abdominal computerized tomography was
indicated , which confirmed the mass, and during the same procedure a
guided puncture was performed that confirmed RCCC (Figure-2). It was then
performed a body-tail pancreatectomy and splenectomy.
The patient is being followed for 2 years
in an outpatient basis without evidences of neoplasic progression, presenting
an excellent quality of life.
COMMENTS
Among
the total cases of metastatic diseases due to RCCC, there is a subgroup
where the metastatic disease arises as a single lesion in a particular
organ following radical nephrectomy, which corresponds to 3 or 4% in large
series of patients under such conditions. In such cases, the following
are considered as good prognostic factors for treatment: 1) otherwise
healthy patients, 2) age under 60 years, 3) single metastasis in lung,
4) period between nephrectomy and the occurrence of the lesion longer
than 24 months (2,3).
The successful aggressive treatment of consecutive
metachronous metastases in different organs is a theme poorly addressed
in the literature. Despite the controversial management and the short
period of follow-up in this case relative to the exeresis of the last
lesion (24 months) the patient presents an excellent outcome. We believe
that in young, otherwise healthy patients who present a late recurrence
with a single and organ-independent metastasis, the hypothesis of surgical
treatment should be considered as a first line option for this selected
subgroup.
REFERENCES
- de Kernion JB, Ramming KP, Smith RB: The natural history of metastatic renal cell cancer: a computer analysis. J Urol. 1978; 120: 148-52.
- Kozlowski JM: Management of distant solitary recurrence in the patient with renal cancer. Urol Clin North Am. 1994; 21: 601-24.
- Faure JP, Tuech JJ, RicherJP, Pessaux P, Arnaud JP, Carretier M: Pancreatic metastasis of renal cell carcinoma: presentation, treatment and survival. J Urol. 2001; 165: 20-2.
_________________________
Received:
December 27, 2002
Accepted after revision: March 25, 2003
_______________________
Correspondence
address:
Dr. Carlos M. N. de Jesus
Departamento de Urologia
Faculdade de Medicina de Botucatu
Distrito de Rubião Júnior
Botucatu, São Paulo, 18618-970, Brazil
Fax.: + 55 14 6802-6271
E-mail: marcio@fmb.unesp.br