NEPHROBRONCHIAL
FISTULA SECONDARY TO XANTOGRANULOMATOUS PYELONEPHRITIS
(
Download pdf )
JOSE R. DE SOUZA, JULIANA A. ROSA, NEY C. B. BARBOSA
Goiânia General Hospital, Goiânia, Goiás, Brazil
ABSTRACT
Introduction:
Nephrobronchial fistula is a rare complication of xanthogranulomatous
pyelonephritis, a disease that can fistulize to lungs, skin, colon and
other organs.
Case Report: A 37-year old patient presented
a chronic history of lumbar pain and thoracic symptoms such as cough,
dyspnea and oral elimination of pus. Patient went to several services
and was submitted to 2 thorax surgeries before definitive treatment (nephrectomy)
was indicated. After nephrectomy, the patient presented an immediate improvement
with weight gain (8 kg / 1 month) and all his symptoms disappeared.
Conclusion: This clinical case illustrates
the natural history of nephrobronchial fistula, the importance of clinical
history for diagnosis and the relevance of early treatment of renal lithiasis.
Key
words: kidney; xanthogranulomatous pyelonephritis; kidney calculi;
urinary fistula; urinary tract infection; bronchial fistula.
Int Braz J Urol. 2003; 29: 241-2
INTRODUCTION
Xanthogranulomatous pyelonephritis is caused by chronic presence of stones in the excretory system, which evolves with localized infection, renal destruction and systemic impairment. Fistulization is a rare complication (1-3). There are reports of nephrobronchial (1,2), nephrocutaneous (2), colonic (3), gastric, jejunal fistulas, and also fistulas to psoas muscle, flank and gluteal region.
CASE REPORT
VSL,
37 years old, Caucasian, without pathological antecedents. Between 1985
and 1993, the patient presented several crises of renal colic and eliminated
20 calculi. From 1994 to January 1999, he presented a continuous pain
in right lumbar region and medicated himself with analgesic drugs. Early
in 1999, he presented pyuria, 40ºC fever, anorexia and renal stones
that were treated clinically.
After 3 months, he evolved with dyspnea,
being hospitalized several times. In 1999, he sought the General Hospital
due to dyspnea, when 1 liter of pus was drained from his right hemithorax
and he was subjected to antibiotic therapy.
In July 1999 he presented “pus taste
in the mouth”, cough and dyspnea. He sought the hospital where thorax
was drained and surgically debrided. Fifteen days later, still with a
thorax drain, he came back for presenting the initial clinical picture.
By the end of July 1999 a right inferior lobectomy was performed, with
clinical improvement and release from hospital.
After some months cough returned and there
was fistulization with purulent drainage through the right thoracolumbar
wall. Output from lumbar fistula decreased progressively as the patient
began to expel pus by the mouth until the fistula’s closure.
From 2000 to April 2001 patient expelled
pus by the mouth in larger amount during periods of cough, physical efforts
and mainly when he flexed the abdomen over his tights. During this period,
the patient was assessed by several medical teams. According to him, clinical
doctors and urologists thought that the disease was basically renal, but
pneumologists disagreed with this hypothesis.
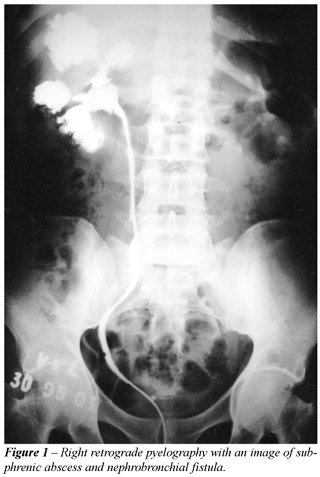
Patient was then seen in General Hospital
and, after urologic assessment and right retrograde pyelography (Figure-1),
a nephrobronchial fistula was suggested and patient underwent a right
nephrectomy with drainage of a subphrenic abscess by mid-2001. He evolved
with immediate improvement, ceasing of cough and oral elimination of pus,
disappearance of anemia and anorexia, recovering 8 kilograms within 1
month post-operatively. The anatomopathological examination evidenced
xanthogranulomatous pyelonephritis.
COMMENTS
Nephrobronchial
fistula are rare complications of renal lithiasis that usually occur following
a long period of disease. Infection by human immunodeficiency virus, association
with diabetes and the presence of untreated renal stones are predisposing
factors (1-3).
The patient in this report presented untreated
renal stone associated with renal colic, renal cavity infection, thoracocutaneous
fistulization, cough, dyspnea, and finally purulent expectoration.
Treatment in advanced cases should be nephrectomy
with drainage of the abscess and the fistula (3).
This case illustrates the natural history
of nephrobronchial fistula, the significance of clinical history for diagnosis
and the relevance of early treatment of renal lithiasis.
REFERENCES
- Caberwal D, Katz J, Reid R, Newman HR: A case of nephrobronchial and colonobronchial fistula presenting as lung abscess. J Urol. 1977; 117:371-3.
- Calvo Quintero JE, Alcover Garcia J, Gutierrez del Pozo R, Pedemonte Vives J, Romero Martin JA, Corominas Estrella S, et al.: Fistulization in xanthogranulomatous pyelonephritis. Presentation of 6 clinical cases and review of the literature. Actas Urol Esp. 1989; 13:363-7.
- Rao MS, Bapna BC, Rajendran LJ, Shrikhande VV, Prasanna A, Subudhi CL, et al.: Operative management problems in nephrobronchial fistula. Urology 1981; 17:362-3.
_________________________
Received: November 25, 2002
Accepted after revision: April 2, 2003
_______________________
Correspondence address:
Dr. Jose Rosa de Souza
Hospital do Rim de Goiânia
Alameda das Rosas, 2041
Goiânia,GO, 74125-010, Brazil
Fax: + 55 62 291-2030
E-mail: joserosasouza@aol.com