MULTIPLE
FOREIGN BODIES IN THE ANTERIOR AND POSTERIOR URETHRA
(
Download pdf )
TROY SUKKARIEH, MARC SMALDONE, BHARAT SHAH
Northport Veterans Affairs Medical Center, Northport, New York, USA
ABSTRACT
Foreign bodies of the urethra and bladder are seen with iatrogenic injury, self-insertion, and rarely migration from adjacent sites. Treatment is focused on foreign body extraction, diagnosing complications, and avoiding compromise of erectile function. With advances in endourology, the majority of cases can now be managed endoscopically. We present a case of a man with multiple foreign bodies located both above and below the urogenital diaphragm. Advancing the posterior objects intravesically and extracting with a stone basket accomplished successful removal.
Key
words: urethra; bladder; foreign body; endoscopy
Int Braz J Urol. 2004; 30: 219-20
INTRODUCTION
Foreign bodies of the urethra and bladder are seen with iatrogenic injury, self-insertion, and rarely migration from adjacent sites. Treatment is focused on foreign body extraction, diagnosing complications, and avoiding compromise of erectile function (1-4).
CASE REPORT
A
59-year-old male presented to the emergency room with dysuria and urinary
dribbling. After questioning, he noted inserting multiple small metal
objects into his urethra. Patient denied any fevers or chills. He was
able to dribble blood tinged urine with straining. The patient reported
a history of major depression, but no history of self-injurious behavior.
His physical examination was significant for a non-distended bladder,
meatal stricture, and multiple palpable foreign bodies from the glans
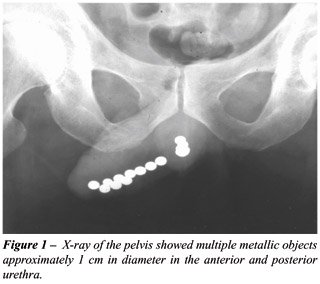
penis to the penoscrotal junction. X-rays of the pelvis showed multiple
metallic objects approximately 1 cm in diameter in the anterior and posterior
urethra (Figure-1).
The patient was taken to the operating room
after receiving pre-operative intravenous antibiotics. After performing
a meatotomy, a total of 10 metallic objects in the anterior urethra were
milked out and delivered from the urethra. A cystoscopic examination was
performed which demonstrated multiple metallic objects in the proximal
urethra. These objects were pushed into the bladder using the cystoscope.
After this, the metallic objects were individually removed using a three-prong
stone basket. An 18F urethral catheter was kept in place for 24 hours.
The patient received a complete inpatient psychiatric evaluation post-operatively.
He was subsequently discharged home after successfully voiding.
COMMENTS
Foreign
bodies are most commonly inserted into the genitourinary tract by psychiatric,
intoxicated, confused, or sexually curious patients. It has also been
documented that well-adjusted patients without concomitant psychiatric
illnesses have attempted to relieve urinary retention or itching by inserting
objects into the urethra.
Co-morbidities reported in patients presenting
with foreign body insertion include exotic impulses most commonly sexual
in nature, mental illness, borderline personality disorder, and intoxication.
Alibadi et al. (4) reported that reasons for self-instrumentation in their
population of 18 patients included auto-eroticism in 6 (33%), overt psychiatric
causes in 2 (11%), to aid in voiding in 7 (39%), and in 3 patients (17%)
no definite reason could be ascertained.
The presenting symptoms reflect irritation
of the lower genitor-urinary tract with the most common being dysuria,
lower abdominal and urethral pain, microscopic or gross hematuria, acute
urinary retention, urethral discharge, and fevers (1-4). Diagnosis can
frequently be determined by clinical history and careful physical examination.
Objects located distal to the urogenital diaphragm can typically be palpated
directly, while objects proximal to the diaphragm are not readily palpable.
If the diagnosis is unclear, radiopaque foreign bodies can be localized
with plain X-ray film examination supported by endoscopic examination,
while excretory urogram or cystograms and ultrasound imaging may reveal
radiolucent objects.
The main objectives of treatment include
diagnosing complications, foreign body extraction, and avoiding compromise
of erectile function. Endoscopic manipulation and extraction utilizing
forceps and snares, balloon-wires, and stone-retrieving baskets have been
documented as successful in the removal of foreign objects located below
the urogenital diaphragm. Due to the high incidence of co-morbid psychiatric
disease, mental retardation, and dementia, it has been suggested that
patients presenting in this manner have routine psychiatric evaluation,
although this had not been universally agreed upon.
REFERENCES
- Gonzalgo ML, Chan DY: Endoscopic basket extraction of a urethral foreign body. Urology. 2003; 62:352.
- van Ophoven A, deKernion JB: Clinical management of foreign bodies of the genitourinary tract. J Urol. 2000;164: 274-87.
- Quin G, McCarthy G: Self insertion of urethral foreign bodies. J Accid Emerg Med. 2000; 17: 231.
- Aliabadi H, Cass AS, Gleich P, Johnson CF: Self-inflicted foreign bodies involving lower urinary tract and male genitals. Urology. 1985; 26: 12-6.
__________________________
Received:
September 29, 2003
Accepted after revision: December 22, 2003
_______________________
Correspondence address:
Dr. Troy Sukkarieh
Department of Urology
Health Sciences Center T-9 Room 040
University Hospital and Medical Center
Stony Brook, NY 11794-8093, USA
Fax: + 1 631 444-7620
E-mail: tsukkarieh@yahoo.com