MAGNETIC
RESONANCE IMAGING IN THE DIAGNOSIS OF PELVIC FLOOR DISORDERS
(
Download pdf )
FERNANDO G. DE ALMEIDA, LARISSA V. RODRÍGUEZ, SHLOMO RAZ
Department of Urology, University of California Los Angeles (UCLA), Los Angeles, California, USA
ABSTRACT
Vaginal prolapse due to pelvic floor dysfunction occurs frequently in postmenopausal women. The disease usually involves all compartments of the vagina, so that isolated defects are uncommon. In advanced disease, it can be difficult to identify which organs are prolapsed, owing to the large bulge in vaginal area. Accurate diagnosis of pelvic floor defects, actual prolapsed organs, and presence of any coexisting abnormalities are essential to correctly plan surgical reconstruction and minimize the risk of recurrence. In this review, we discuss the existing imaging modalities available to evaluate pelvic prolapse, emphasizing the role of dynamic magnetic resonance imaging.
Key words:
pelvis; prolapse; magnetic resonance imaging
Int Braz J Urol. 2002; 28: 553-9
INTRODUCTION
Female
pelvic floor dysfunctions are a relatively usual problem, and their clinical
manifestations include cystocele, sigmoid prolapse and/or rectocele, uterine
prolapse and enterocele. The alterations found in female pelvic floor
dysfunctions affects the whole region, so in more advanced stages, usually
a combination of these structures is observed (1). In general, evaluation
of pelvic floor prolapses is performed only by physical examination; however,
in more complex cases, and with many prolapsed structures, physical examination
alone has low specificity and sensibility (2-4). In these cases, it is
known that success of treatment is directly related to a thorough preoperative
evaluation, with accurate identification of prolapsed organs, and staging
of the pelvic floor dysfunction (5).
All physicians who treat patients with pelvic
floor dysfunction must understand clearly the anatomy, as well as be capable
to establish a net relation among multiple anatomic structures in pelvic
region. In patients with a prolapse regional anatomy is altered; thus,
for surgical planning, frequently image exams are necessary.
Formerly, since it does not use ionizing
radiation and is not invasive, ultrasonography was considered the exam
of choice for female pelvis evaluation (6). Later, fluoroscopy was applied
to evaluate the rectum and the urinary bladder, to detect rectocele and
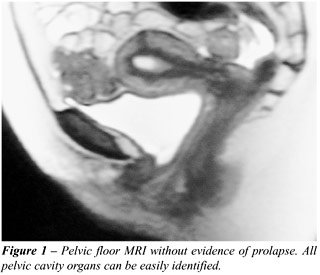
cystocele, respectively (2,3,7). Recently, magnetic resonance imaging
has been used to evaluate and diagnose pelvic floor dysfunctions (Figure-1),
for it is a non-invasive procedure that provides detailed images of all
pelvic cavity structures in just one and prompt exam, it doesn’t
expose the patient to ionizing radiation, and doesn’t need contrast
(8-17). In this review, we present a critical analysis of imaging methods
available for pelvic prolapse evaluation, emphasizing the role of the
magnetic resonance imaging (MRI).
ENTEROCELE
One
can differentiate enteroceles in simple and complex. Simple enteroceles
are those where vaginal cupula does not present defects of support. Complex
enteroceles present an association with vaginal cupula prolapse, and tend
to coexist with anterior and posterior vaginal walls prolapses. Symptomatic
enteroceles can cause vaginal pressure, dyspareunia and lumbosacral pain;
occasionally patients complain of severe constipation, sensation of incomplete
evacuation and symptoms of intestinal obstruction (18). When there is
prolapse of more than one vaginal wall, or more than one organ, it becomes
difficult to evaluate all compartments just by physical examination (6).
Additionally, it is very difficult to accurately differentiate an enterocele
from a high rectocele (6). Formerly, defecography was the only method
available to help in enterocele diagnosis. Nowadays, cystocolpoproctography
with fluoroscopy has been used. However, these exams are highly invasive,
exposing the patient to ionizing radiation; and because of the need to
contrast bladder, rectum, bowel, and vagina, it takes too much time to
carry out. In addition to all these inconveniences, it still presents
20% failure in detecting enteroceles (3,9-24).
More recently, MRI has been effectively
used to evaluate pelvic floor morphological alterations. Just as other
exams to evaluate a perineal region prolapse, in MRI images are obtained
at rest and with straining. In a study comparing physical examination,
surgical findings and MRI in women with and without a prolapse, it was
observed that MRI presents a sensibility of 87%, and a positive predictive
value of 91% compared to surgical findings, as well as being significantly
superior in detecting enterocele when compared to physical examination
(15). In the same way, Lienemann et al., using MRI with organ opacification,
showed that MRI has a greater sensibility in detecting enterocele than
physical examination and dynamic cystoproctography (24). Another advantage
of the MRI is to distinguish enteroceles according to their contents (small
and large intestine, rectosigmoidocele, or mesenteric fat), making surgical
planning easier and more reliable (14,15,24,25). Until recently, fluoroscopic
multiphasic cystocolpoproctography was considered the best radiologic
exam for detecting pelvic prolapse. A study comparing MRI multiphasic
and cystoproctography multiphasic fluoroscopic showed similar rates in
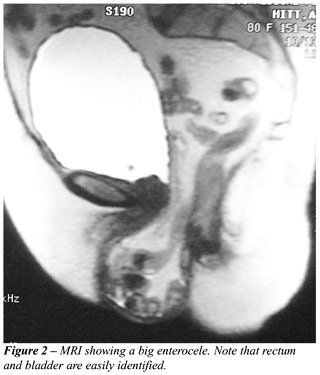
detecting enterocele (20). In our practice, we observed that it is possible
to obtain excellent images with MRI (Figure-2), without needing oral opacifiers
to contrast the bowel and without the need of rectal contrast to the rectum.
We also noticed that the gain with the invasive examination is minimum
to warrant its use instead of an exam completely unaggressive to the patient
(15,20,24). In general, dynamic MRI is a non-invasive exam, and superior
to any other in diagnosing enterocele.
CYSTOCELES
Cystoceles
can be traditionally classified according to the severity of vesical prolapse
(grades I, II, III, and IV), or by the type of anatomic defect (central,
lateral, or both) (26). The majority of cystoceles grades I and II are
usually asymptomatic, and may be associated with urethral hypermobility
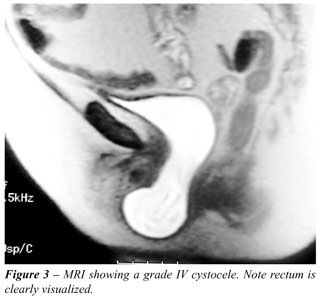
and urinary stress incontinence. The vesical prolapses of higher grades
(grade III and IV cystoceles) are commonly symptomatic and associated
to other types of prolapse (Figure-3). Usual manifestations include vaginal
mass, vaginal pressure, dyspareunia, urinary infection, urinary tract
obstructive symptoms, including urinary retention and hydroureteronephrosis.
The lack of identification of all types of prolapse can lead to an incomplete
surgical correction with resulting recurrence (1,13,14). Physical examination
limits individualization and identification of all prolapsed structures
when a great vaginal mass is present (2-4). Additionally, isolated repair
of a cystocele without any regard to the remaining pelvic floor predispose
to an increase in the incidence of de novo enterocele, rectocele, and
uterine prolapse, due to a vaginal axis alteration (15). Higher grades
cystoceles may mask urinary stress incontinence and urethral hypermobility.
Surgical results in the treatment of urinary incontinence tend to be better
with complete restoration of pelvic floor anatomy. Due to all reasons
mentioned above, we observed that it is essential that prolapsed structures
are clearly identified before any pelvic floor procedure.
Optimal image method for cystoceles evaluation
should provide information about other types of prolapse; about presence
or absence of infravesical and ureteral obstruction; and about presence
or absence of urethral hypermobility, as well as evaluate the presence
of urinary stress incontinence. Videourodynamics and voiding cystography
have been utilized in cystocele evaluation. These studies are done in
upright position during abdominal straining and at rest, being useful
in determining the severity of cystocele, urethral hypermobility evaluation,
and urinary stress incontinence, as well as documenting the postvoid residue
(7). Unfortunately, these studies do not provide information related to
pelvic floor dysfunctions altogether. Cystocolpoproctography, as discussed
before, presents a high ionizing radiation exposition, is time-consuming
and needs invasive contrast application (3, 19 - 24). Perineal ultrasonography
may be utilized to urethral hypermobility and vaginal prolapse evaluation;
however, there are few studies reported, its efficiency is operator and
device dependent, and the method doesn’t provide adequate visualization
of the planes between the tissues (27).
For isolated cystoceles, a physical examination
and a voiding cystourethrography are adequate. For a high grade cystocele
associated with prolapse of other compartments, we recommend the use of
dynamic MRI associated with videourodynamics. Studying, staging, and determining
pelvic floor relaxation method using MRI was clearly described (14). MRI
provides information about other pelvic compartments with concomitant
evaluation of enterocele, uterine prolapse, and rectocele, as well as
documenting urethral hypermobility, and postvoid urinary residue. An additional
advantage is the evaluation of possible ureteral obstructions due to cystocele,
hydronephrosis, and other pelvic pathologies. Gousse et al. demonstrated
that MRI utilized for cystocele evaluation presented a 100% sensibility,
a 83% specificity, and a 97% positive predictive value compared to surgical
findings (15). The same authors found other types of pelvic pathologies
in 55% of patients, including 3 with bilateral hydroureteronephrosis (15).
MRI presents a high-grade correlation with
cystography in cystocele diagnosis (28). The main concern of MRI is the
fact that the examination is done with patient in supine position, what,
ultimately, would impair the diagnosis or underestimate the prolapse grade.
However, MRI presents many advantages, of which the paramount are: doesn’t
use ionizing radiation, doesn’t require urethral catheterization,
provides details of the 3 pelvic compartments, evaluate concomitant pathologies,
inform about urethral hypermobility, as well as evaluates ureteral obstruction
and postvoid residue (9 - 15, 28).
RECTOCELE
Rectocele
results from a defect in prerectal and pararectal fasciae, and in retrovaginal
septum (26). Rectocele can be present in up to 80% of asymptomatic patients
(13). The symptoms include vaginal pressure, vaginal mass, dyspareunia,
and constipation. Diagnosis generally is by physical examination. As well
as any other kind of pelvic floor relaxation, rectoceles are usually associated
with other types of prolapse. In these cases, due to competition for space
between prolapsed organs, there is a difficulty in diagnosis, and the
possibility of a non-detected rectocele in physical examination (6). The
sensibility of the physical examination alone for the diagnosis of rectocele
varies from 31 to 80% (2-4,6,21,29). Additionally, physical examination
frequently is not capable to distinguish an enterocele from a high rectocele.
For these reasons, imaging exams should be utilized to help identifying
rectoceles.
Traditionally, defecography has been used
for more accurate diagnosis of rectocele. Since rectocele is commonly
associated to other organs prolapses, many authors have used cystocolpoproctography
for its diagnosis (3,19-21,29). The disadvantages of these techniques
are inability to visualize soft tissue of the pelvic floor, invasiveness
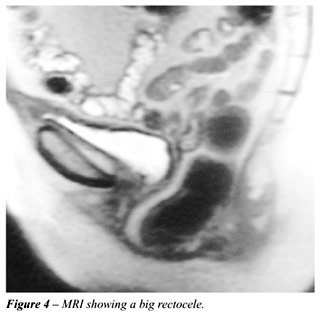
and significant use of ionizing radiation. Some authors have used MRI
in an attempt to better evaluate pelvic structures, pelvic floor muscles
and soft tissue inside pelvic cavity (Figure-4). In a study comparing
MRI in detecting multiple types of vaginal prolapse with surgical findings,
76% sensibility and 96% positive predictive value was observed for rectocele
diagnosis (15). These results are relatively poor when compared to detection
rates of other types of prolapse by MRI. The authors justified that if
the rectum is empty and its walls collapsed, MRI would fail to detect
small rectoceles. There are studies presenting high sensibility and specificity
with 100% of appropriateness in rectocele diagnosis using MRI with rectal
contrast (25). Others showed that dynamic triphasic MRI and fluoroscopic
cystocolpoproctography presented a similar rate of detection (20). One
way to improve detecting rectocele by MRI is through rectal opacification
by introducing gel utilized in ultrasonography. However, this procedure,
besides bringing invasiveness to the method, can generate image artifacts
through the introduction of air along with the gel (15,20).
UTERINE PROLAPSE
Uterosacral
ligament permits the anterior movement of the cervix leading to a progressive
retroversion of the organ, and subsequent prolapse (26). Uterine prolapse
grades I and II are generally asymptomatic, although grades III and IV
present as vaginal masses, dyspareunia, urinary retention, and lumbar
pain. Uterine prolapse grade IV has been associated to chronic and progressive
ureteral obstruction. In surgical planning in this kind of prolapse, is
essential to determine uterus size and discard any uterine or ovarian
pathology, of benign or malign origin. Since it is necessary to evaluate
other prolapse types, and presence of other utero-ovarians pathologies,
MRI is the ideal exam to evaluate uterine prolapse (Figure-5). MRI provides
information about presence or absence of cystocele, rectocele, urethral
hypermobility, and urethral diverticula; information about the size and
possible pathologies of the uterus (tumors, myomas, cysts, etc.); ovarian
pathologies (cysts or masses); and also evaluate ureteral obstruction
(9,10,13-15,28). Gousse et al. reported 83% sensibility, 100% specificity,
and 100% positive predictive value when compared to surgical findings.
These findings aren’t different from those found when performing
physical examination (15). However, MRI could define clearly other pelvic
cavity compartments, and diagnosed some concomitant uterine and/or ovarian
pathology in 30% of the patients (15).

FINAL CONSIDERATIONS
Many
studies using MRI of normal patients improved our understanding about
the region normal anatomy (30-32). Additionally, analyses of regional
musculature by MRI have contributed to the understanding of pelvic floor
dysfunctions (33-35). This shows how images provided by MRI are detailed
and allows an accurate study of the pelvic region.
Major concern about the use of MRI is related
to the high cost of the procedure. However, in severe cases of vaginal
prolapses, frequently is necessary the use of ultrasonography, excretory
urography, voiding uretrocystography, and/or defecography, for a more
accurate diagnosis. In these cases, use of MRI may substitute all these
exams, lowering considerably invasiveness to the patient, and making reasonable
the relative toll.
Pelvic floor dysfunction usually leads to
alterations in all compartments of female pelvic cavity. In advanced cases,
with involvement of many compartments, accurate identification of all
organs occupying the vaginal region is essential to surgical planning
and success. In such situations, there is a competition for space in the
vaginal region, making diagnosis difficult only by physical examination.
In this way, we need an exam that provides a wide and simultaneous evaluation
of all pelvic region, and elucidates any doubt that may persist after
physical examination. Due to its non-invasiveness, rapidity, simplicity
and non-exposition of the patient to ionizing radiation, MRI is an image
method very useful to study pelvic floor and identify cystocele, rectocele,
enterocele, and uterine prolapse. Furthermore, it provides high quality
images that allow throughout evaluation of all pelvic cavity components,
including soft tissue, which is not possible with other studies based
on fluoroscopy (10,12-16,25,33).
___________________________
Dr. Fernando G. Almeida holds a
scholarship from CNPq, Brazil
REFERENCES
- Maglinte DD, Kelvin FM, Fitzgerald K: Association of compartment defects in pelvic floor dysfunction. Am J Roentgenol. 1999; 172: 439-44.
- Kelvin FM, Maglinte DD: Dynamic cystoproctography of female pelvic floor defects and their interrelationships. Am J Roentgenol. 1997; 169: 769-74.
- Kelvin FM, Hale DS, Maglinte DD: Female pelvic organ prolapse: diagnostic contribution of dynamic cystoproctography and comparison with physical examination. Am J Roentgenol. 1999; 173: 31-7.
- Stovall DW: Transvaginal ultrasound findings in women with chronic pelvic pain. Obstet Gynecol. 2000; 95 (suppl 1): S57.
- Safir MH, Gousse AE, Rovner ES: 4-Defect repair of grade 4 cystocele. J Urol. 1999, 161: 587-94.
- Siproudhis L, Ropert A, Vilotte J: How accurate is clinical examination in diagnosing and quantifying pelvirectal disorders? A prospective study in a group of 50 patients complaining of defecatory difficulties. Dis Colon Rectum. 1993; 36: 430-38.
- Raz S, Erickson D, Sussman E: Operative repair of rectocele, enterocele and cystocele. Adv Urol. 1992; 5: 121-44.
- Klutke C, Golomb J, Barbaric Z: The anatomy of stress incontinence: magnetic resonance imaging of the female bladder neck and urethra. J Urol. 1990; 143: 563-6.
- Yang A, Mostwin JL, Rosenshein NB, Zerhouni EA: Pelvic floor descent in woman: dynamic evaluation with fast MR imaging and cinematic display. Radiology. 1991; 179: 25-33.
- Goodrich MA, Webb MJ, King BF: Magnetic resonance imaging of pelvic floor relaxation: dynamic analysis and evaluation of patients before and after surgical repair. Obstet Gynecol. 1993; 82: 883-91.
- Strohbehn K, Ellis JH, Strohbehm JA, DeLancey JO: Magnetic resonance imaging of the levator ani with anatomic correlation. Obstet Gynecol. 1996; 87: 277-85.
- Ozasa H, Mori T, Togashi K: Study of uterine prolapse by magnetic resonance imaging: topographical changes involving the levator ani muscle and the vagina. Gynecol Obstet Invest. 1992; 34: 43-8.
- Lienemann A, Anthuber C, Barron A: Dynamic MR colpocystorectography assessing pelvic-floor descent. Eur Radiol. 1997; 7: 1309-17.
- Comiter CV, Vasavada SP, Barbaric ZL: Grading pelvic floor prolapse and pelvic floor relaxation using dynamic magnetic resonance imaging. Urology. 1999; 54: 454-7.
- Gousse AE, Barbaric ZL, Safir MH: Dynamic half Fourier acquisition single shot turbo spin-echo magnetic resonance imaging for evaluating the female pelvis. J Urol. 2000; 164: 1606-13.
- Rouanet JP, Mares P, Courtieu C, Maubon A: Static and dynamic MRI of the normal and pathological female pelvic floor. J Gynecol Obstet Biol Reprod. 2000; 164: 1606-13.
- Lienemann A, Sprenger D, Jansen U: Functional MRI of the pelvic floor: the methods and reference values (in German). Radiologie. 2000; 45: 458-64.
- Shull BL: Clinical evaluation of women with pelvic support defects. Clin Obstet Gynecol. 1993; 36: 936-51.
- Takano M, Hamada A: Evaluation of pelvic descent disorders by dynamic contrast reontography. Dis Colon Rectum. 2000; 43: 205-12.
- Kelvin FM, Maglinte DDT, Hale DS, Benson JT: Female pelvic organ prolapse: a comparison of triphasic dynamic MR imaging and triphasic fluoroscopic cystocolpoproctography. Am J Roentgenol. 2000; 174: 81-4.
- Altringer WE, Saclarides TJ, Dominguez JM: Four-contrast defecography: pelvic ‘floor-oscopy’. Dis Colon Rectum. 1995; 38: 695-9.
- Brubaker L, Retzky S, Smith C, Saclarides T: Pelvic floor evaluation with dynamic fluoroscopy. Obstet Gynecol, 82: 863-868, 1993.
- Hock D, Lombard R, Jehaes C: Colpocystodefecography. Dis Colon Rectum. 1993 36: 1015-21.
- Lienemann A, Anthuber C, Baron A, Reuser M: Diagnosing enteroceles using dynamic magnetic resonance imaging. Dis Colon Rectum. 2000; 43: 205-12.
- Tunn R, Paris S, Taupitz M: MR imaging in posthysterectomy vaginal prolapse. Int Urogynecol J Pelvic Floor Dysfunct. 2000; 11: 87-92.
- Raz S, Stothers L, Chopra A: Vaginal Rconstructive Srgery for Icontinence and Polapse. In: Walsh PC, Retik AB, Vaughan ED, Wein AJ (eds.), Campbell’s Urology. Philadelphia, WB Saunders Co, 2nd ed., 1998, pp.1059–94.
- Mouritsen L: Techniques for imaging bladder support. Acta Obstet Gynecol Scand. 1997; Suppl 166: 48-9.
- Gufler H, DeGreforio G, Allman KH: Comparison of cystourethrography and dynamic MRI in bladder neck descent. J Comput Assist Tomogr. 2000; 24: 382-8.
- Cundiff GW, Nygaard I, Bland DR, Versi E: Proceedings of the American Urogynecologic Society Multidisciplinary Symposium on Defecatory Disorders. Am J Obstet Gynecol. 2000; 182: S1-S10.
- Fielding JR, Dimanli H, Schreyer AG: MR-based three-dimensional modeling of the normal pelvic floor in women: quantification of muscle mass. Am J Roentgenol. 2000; 174: 657-60.
- Goh V, Halligan S, Kaplan G: Dynamic MR imaging of the pelvic floor in asymptomatic subjects. Am J Roentgenol. 2000; 174: 661-6.
- Myers RP, Cahill DR, Kay PA: Puboperineales: muscular boundaries of the male urogenital hiatus in 3D from magnetic resonance imaging. J Urol. 2000; 164: 1412-5.
- Healy JC, Halligan S, Reznek RH: Patterns of prolapse in women with symptoms of pelvic floor weakness: assessment with MR imaging. Radiology. 1997; 203: 77-81.
- Hjartardottir S, Nilsson J, Petersen C, Lingman G: The female pelvic floor: a dome – not a basin. Acta Obstet Gynecol Scand. 1997; 76: 567-71.
- Tan IL, Stoker J, Zwamborn AW: Female pelvic floor: endovaginal MR imaging of normal anatomy. Radiology. 1998, 206: 777-83.
Received: June 14, 2002
Accepted: July 17, 2002
_______________________
Correspondence address:
Dr. Larissa V. Rodríguez
924 Westwood Blvd. Suite 520
Los Angeles, California, 90024, USA
Fax: + 1 310 794-0206
E-mail: lrodriguez@mednet.ucla.edu