ORTHOTOPIC
URETEROCELE MASQUERADING AS A BLADDER TUMOR IN A WOMAN WITH PELVIC PAIN
(
Download pdf )
DAVID D. THIEL, STEVEN P. PETROU, GREGORY A. BRODERICK
Department of Urology, Mayo Clinic Jacksonville, Jacksonville, Florida, USA
ABSTRACT
Single system orthotopic ureteroceles often present in adulthood are associated with characteristic radiographic findings. We present the case of a 54 year old woman with 8 months of urgency/frequency and pelvic pain that has the cystoscopic appearance of a bladder tumor. Cystoscopic images, radiographs and intraoperative photos demonstrate the work-up, evaluation, and treatment of this unique single system orthotopic ureterocele containing a calculus. This patient demonstrates the need for cystoscopy accompanied by upper tract imaging in patients with new onset pelvic pain, urgency/frequency, and frequent urinary tract infections.
Key
words: bladder; ureterocele; bladder neoplasms; ureteral calculi;
pelvic pain
Int Braz J Urol. 2005; 31: 549-51
CASE REPORT
A
54 year old white female was referred from her gynecologist for a bladder
tumor. The patient had complained of worsening lower abdominal and pelvic
pain accompanied by urinary urgency/frequency for the past 8 months. Treatment
of four separate culture proven E. coli urinary tract infections with
appropriate antibiotics failed to relieve the patient’s symptoms.
Diagnostic cystoscopy was performed to evaluate the complaints and the
patient sent to urologist for the finding of a bladder tumor.
Past medical history was significant for
osteoporosis and carpal tunnel repair. The patient was a hair dresser
with a 30 pack-year smoking history. The patient denied any previous urologic
history including calculi or hematuria. Physical exam revealed a physically
fit female without costo-vertebral tenderness. Laboratory evaluation revealed
only microscopic hematuria with negative urine cytology.
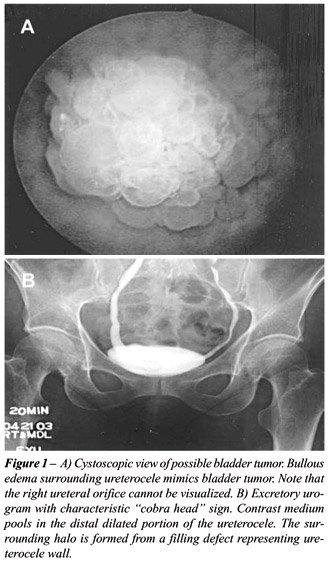
In office cystoscopy was performed that
revealed a papillary bladder tumor present at the right lower posterior
portion of the bladder (Figure-1). The right ureteral orifice could not
be identified. An excretory urogram was performed that revealed a non-obstructing,
single system, distal right ureteral calculus surrounded by a radiolucent
ring (Figure-1). Pelvic CT scan demonstrated what appeared to be a stone
contained in a distal right ureterocele (Figure-2).
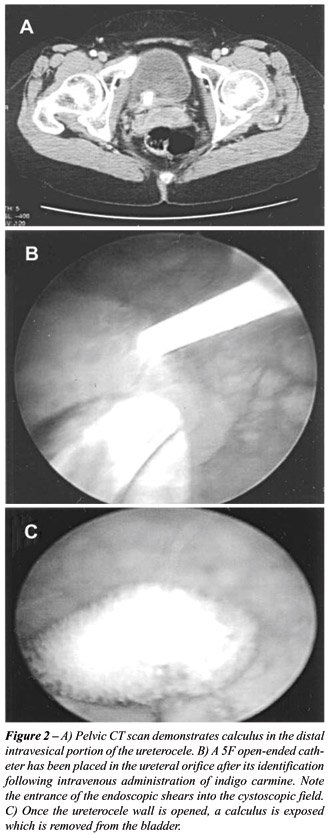
The patient was taken to the operating room
and cystoscopy performed. One ampoule of intravenous indigo carmine solution
was given that eventually was secreted from the ureteral orifices. Once
the opening of the right ureteral orifice was identified via secretion
of the blue dye, a 5F open-ended catheter was placed inside the orifice
into the kidney under fluoroscopic vision (Figure-2). The orifice was
then sliced open utilizing endoscopic shears exposing a large stone (Figure-2).
The stone was removed from the bladder and the ureteral stent removed.
At the six month postoperative visit the
patient noted complete resolution of her voiding symptoms and pelvic discomfort.
She had no further documented urinary tract infections during that time.
A voiding cystourethrogram performed at the 6 month postoperative visit
failed to demonstrate vesico-ureteral reflux.
COMMENTS
Single
system (orthotopic) ureteroceles are usually discovered in adults and
are almost always intravesical (1). Urinary stasis in the dilated distal
segment often lends to urinary infection and stone formation; precluding
the most common presenting symptoms of dysuria, urgency, and recurrent
urinary infections.
Diagnosis is often via excretory urography
demonstration of the characteristic “cobra-head” sign (Figure-1).
The radiolucent halo surrounding the dense filling area is a filling defect
representing the ureterocele wall (1).
Intravesical incision of the ureterocele
is the treatment of choice in adults and has been described utilizing
endoscopic shears and holmium laser technology (2). Vesico-ureter reflux
is seldom a problem following incision (3).
This patient demonstrates the necessity
of cystoscopy accompanied by upper tract imaging in patients presenting
with new onset urinary urgency/frequency or pelvic discomfort. The bullous
edema surrounding an intravesical ureterocele containing calculus such
as this case can mimic bladder tumors and confuse the less experienced
cystoscopist.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Schlussel RN, Retik AB: Ectopic Ureter, Ureterocele, and other Anomalies of the Ureter. In: Walsh PC et al. (eds.), Campbell’s Urology, Philadelphia, WB Saunders. 2002; 8th ed., pp. 2022-34.
- Aron M, Costello AJ: Case report: holmium laser resection and lasertripsy for intravesical ureterocele with calculus. Lasers Surg Med. 2001; 29: 82-4.
- Rich MA, Keating MA, Snyder HM 3rd, Duckett JW: Low transurethral incision of single system intravesical ureteroceles in children. J Urol. 1990; 144: 120-1.
____________________
Received:
May 12, 2005
Accepted after revision: July 25, 2005
_______________________
Correspondence address:
Dr. David D. Thiel
3 East Urology - Davis Building
Mayo Clinic Jacksonville
4500 San Pablo Road
Jacksonville, Florida, 32224, USA
Fax: + 1 904-953-7330
E-mail: thiel.david@mayo.edu