UROGENITAL
INVOLVEMENT IN THE KLIPPEL-TRENAUNAY-WEBER SYNDROME. TREATMENT OPTIONS
AND RESULTS
(
Download pdf )
FABIO C. VICENTINI, FRANCISCO T. DENES, CRISTIANO M. GOMES, ALEXANDRE DANILOVIC, FREDERICO A. SILVA, MIGUEL SROUGI
Division of Urology, University of Sao Paulo School of Medicine (USP), Sao Paulo, Brazil
ABSTRACT
Objective:
Klippel-Trenaunay-Weber syndrome (KTWS) is a congenital condition characterized
by vascular malformations of the capillary, venous and lymphatic systems
associated to soft tissue and bone hypertrophy in the affected areas.
This syndrome may involve bladder, kidney, urethra, ureter and genitals.
We report the treatment of 7 KTWS patients with urogenital involvement.
Materials and Methods: From 1995 to 2005,
7 patients with KTWS were evaluated and the charts of these patients were
reviewed.
Results: Patients’ median age was
19-years (range 4 to 46-years) and only 1 was female. The clinical presentation
included genital deformities in 3 cases, hematuria in 2 and urethrorragia
in 2, one of which associated with cryptorchidism and phimosis. Three
patients had an association of pelvic and genital malformations, including
2 patients with hematuria due to vesical lesions and 1 patient with left
ureterohydronephrosis due to a pelvic mass. Two patients had urethral
lesions. Treatment included endoscopic laser coagulation for 1 patient
with recurrent hematuria and 1 patient with urethrorrhagia, pelvic radiotherapy
for 1 patient with hematuria and circumcision in 2 patients with genital
deformities. One patient required placement of a double-J catheter to
relieve obstruction. Hematuria and urethrorragia were safely and effectively
controlled with laser applications. Circumcision was also effective. The
patient treated with radiotherapy developed a contracted bladder and required
a continent urinary diversion.
Conclusions: Urogenital involvement in patients
with KTWS is not rare and must be suspected in the presence of hematuria
or significant cutaneous deformity of the external genitalia. Surgical
treatment may be warranted in selected cases.
Key
words: Klippel-Trenaunay-Weber syndrome; urogenital system; hematuria,
lasers, bladder
Int Braz J Urol. 2006; 32: 697-704
INTRODUCTION
Klippel-Trenaunay-Weber
Syndrome (KTWS) is a rare congenital syndrome characterized by vascular
malformations of the capillary, venous and lymphatic systems associated
to soft tissue and bone hypertrophy of an affected lower limb. These alterations
are frequently misdiagnosed as simple hemangiomas, which have a different
clinical behavior (1).
Historically, Klippel and Trenaunay described
the first case of KTWS in 1900 and in 1907 Weber described similar cases.
They believed that the syndrome was secondary to large congenital arteriovenous
fistulae, causing hypertrophy of the affected limb (2). Recently, Tian
et al. identified an angiogenic factor, termed VG5Q, that when over expressed
due to mutations on its gene, causes increased angiogenesis. This is accepted
as the molecular pathogenic mechanism of KTWS (3).
There is considerable variability in the
terminology for these similar syndromes. The diagnosis of the Klippel-Trenaunay
Syndrome should be applied to cases without arteriovenous fistulae, while
Weber or Parks-Weber Syndrome is more appropriate for cases with arteriovenous
fistulae (4). Since the differentiation between the two conditions is
only possible by means of histopathological, radiological and/or genetic
evaluation, we employ the name Klippel-Trenaunay-Weber Syndrome, as recommended
by other authors (5).
Involvement of genitourinary organs is not
rare in patients with KTWS. The bladder is estimated to be affected in
2.3% to 6% of the cases (1). Hematuria is usually the initial clinical
manifestation (1,2). The urethra, external genitalia, kidney and ureter
may also be involved (1).
In this study, we report our experience
with seven patients with KTWS and urogenital involvement.
MATERIALS AND METHODS
We
retrospectively reviewed the records of seven consecutive patients (6
men and 1 woman) evaluated over a period of 10 years, who were referred
to urological evaluation with a previously established diagnosis of KTWS.
The criteria employed for the KTWS diagnosis were the typical clinical
and physical features.
Urological assessment and management varied
according to the patient’s complaints and affected organs. A focused
history and physical examination was performed in all cases. Laboratorial
and imaging studies were obtained according to clinical presentation.
RESULTS
The
bladder and external genitalia were the most commonly affected organs
in our series. Symptoms presented were penile deformity in three patients,
recurrent gross hematuria in two, urethral bleeding in one and phimosis
and cryptorchidism in one. One patient had both penile deformity and unilateral
hydronephrosis, due to entrapment of the bladder and distal segment of
the left ureter secondary to a large pelvic malformation. The patients’
data, urogenital structures involved and urological management are depicted
in Table-1.

Case 1: A 46-year-old man had a history
of gross hematuria since childhood. He had a typically enlarged right
leg and penile varicosities. He underwent cystoscopy elsewhere at the
age of 21 revealing a large hemangiomatous bladder lesion. He was treated
with external beam radiotherapy, and developed actinic cystitis that evolved
to a contracted bladder with lithiasis. A continent diversion with a sigmoid
segment was performed 11 years later, and he remained free of hematuria
and other symptoms for the following 14 years.
Case 2: A 4-year-old boy presented an enlarged
right leg and a lymphedematous enlarged penis and preputial skin that
caused voiding difficulty. He was previously treated elsewhere by inguinal
lymphatic-venous diversion and circumcision. Penile enlargement and deformity
persisted but the voiding symptoms resolved after the foreskin was partially
removed. He was managed with further surgical reduction of the lymphedematous
tissue of the penis with significant aesthetical improvement.
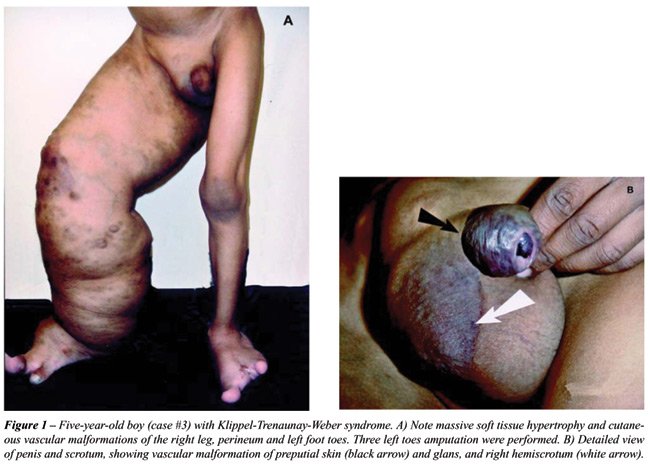
Case 3: A 5-year-old boy with sickle cell
anemia presented an extremely enlarged right leg, penile deformity due
to hemangiomatous varicosities, lymphedema (Figure-1) and a palpable pelvic
mass. Abdominal ultrasound revealed left ureterohydronephrosis and a pelvic
mass involving the bladder. An abdominal CT scan showed a large bladder
lesion extending to the left pelvic wall (Figure-2). Cystoscopy demonstrated
an intensely vascularized bladder lesion that infiltrated most of the
bladder dome and left wall, including the left ureteral orifice. The penile
deformity was managed with surgical removal of the hemangiomatous varicosities
and a double J catheter was placed to drain the left kidney. A laparoscopy
was performed simultaneously to evaluate the pelvic mass, which was shown
to extensively involve the bladder and rectum-sigmoid colon, and was considered
irresectable. The patient has been managed conservatively in the last
two years with periodic changes of the ureteral catheter, but progressive
left renal deterioration occurred due to increasing growth of the pelvic
mass. He has also presented recurrent penile varicosities and urethral
bleeding that has been managed conservatively.

Case 4: A 15-year-old boy presented an enlarged
left leg and buttock and a history of intermittent urethral bleeding.
Urinary tract sonography was normal. Cystoscopy revealed active bleeding
from distal urethral varicose veins, but no bladder lesions. He was treated
with Holmium laser application in the urethral varicosities. The laser
was used with 6 W and a 400 nm fiber. Laser was applied in contact with
the urethral mucosa until vascular sclerosis was achieved. A urethral
catheter was left for 7 days. After 14 months follow-up, the patient remained
free of urethral bleeding.
Case 5: A 25-year-old woman had a diagnosis
of KTWS since the age of five. Her medical history included left colectomy
at the age of 15, due to life-threatening enterorrhagia caused by a large
pericolonic vascular malformation. She also had a history of sporadic
episodes of gross hematuria that were treated conservatively with bladder
irrigation, endovenous epsilon amino–caproic acid and occasional
blood transfusions. She was referred to our hospital after unsuccessful
treatment of recurrent massive hematuria requiring multiple blood transfusions.
Physical examination revealed hemangiomas and hypertrophy of the perineum
and entire left inferior limb. A suprapubic mass was palpable. Abdominal
CT scan revealed diffuse pelvic vascular lesions, involving bladder wall,
peri-rectal and paravesical spaces. Cystoscopy revealed a large, elevated
and irregular lesion with hemangiomatous features that involved 60% of
the bladder surface on the left, posterior, anterior and dome walls, with
well-defined borders and many bleeding sites. The lesion was treated with
a continuous pulse Nd:YAG laser, using a 0.6 mm fiber. The tip of the
fiber was positioned 5 mm from the bladder surface. Total energy delivery
was 3,0000 joules in 90 minutes. Bleeding ceased immediately and the bladder
catheter was removed on the first postoperative day. After a follow-up
period of 14 months, the patient remained free of hematuria.
Case 6: A 5-year-old boy presented enlargement
of both hands and left lower limb. He had right cryptorchidism, phimosis
and a history of a single episode of urethrorrhagia. The testicle was
palpable on the inguinal canal. Many small veins could be seen under the
penile skin. Orchiopexy and circumcision were effective, but subcutaneous
veins made the dissection of the preputial skin more difficult, requiring
ligation of veins and the use of a compressive dressing. At urethrocystoscopy
a small vascular malformation was found in the prostatic urethra, with
no signs of recent bleeding.
Case 7: A 5-year-old boy was referred for
evaluation due to a mild penile and scrotal enlargement associated with
a significant enlargement of the left leg. He was otherwise asymptomatic.
His pelvic CT scan showed an infiltrating mass in the left buttock, posterior
perineum and genital area. The bladder and urethra were not affected and
he was managed conservatively.
COMMENTS
Urogenital
involvement in patients with KTWS is not uncommon and may present with
different manifestations. Bladder involvement is estimated to occur in
2.3% to 6% of the patients, penoescrotal vascular malformations in 8.5%
and vaginal or vulvar in 9.5% of the patients (1). Cases of kidney, renal
artery and ureteral involvement have rarely been reported (1,6-8). Our
series is in accordance with these numbers, with a prevalence of bladder
and genital involvement and one patient with ureteral obstruction associated
with a massive pelvic vascular malformation.
In cases of extensive cutaneous lesions
of the genitals, lower extremities and buttocks, retroperitoneal and urinary
tract involvement should be suspected and radiological evaluation with
CT scan or MRI is recommended (1). Hematuria and urethral bleeding are
also indications for urological evaluation. Bladder and urethral lesions
may be confirmed with cystoscopy. In the bladder, they are usually reddish-blue
and may be pedunculated, sessile, lobulated or flattened, and are frequently
located at the anterior wall or dome (1). Biopsies can lead to massive
bleeding and are not recommended.
Initial treatment of gross hematuria in
these patients is conservative, with bladder irrigation. Anti-fibrinolytic
agents as epsilon amino–caproic or tranexamic acid can be used (9).
In one of our patients (case 5), epsilon was ineffective. Recurrent or
life-threatening hematuria demands specific treatment. Partial cystectomy
used to be the standard treatment but carries significant morbidity (10,11).
Selective embolization of the internal iliac arteries may also be employed,
but recurrence due to rapid development of collateral circulation and
bladder or prostate infarction has been described (12). Radiotherapy is
another therapeutic modality, but only temporary beneficial results are
expected, while the morbidity can be excessive (13). In Case 1, radiotherapy
resulted in actinic cystitis and loss of a functional bladder, requiring
urinary diversion.
The first report of Nd:YAG laser treatment
of bladder hemangiomas associated with KTWS was made by Smith and Dixon
in 1984 (14). Since then, a few cases have been described, with good results
(12,13,15,16). In 1990, Smith reported 13 cases of patients with bladder
hemangiomas who underwent treatment with Nd:YAG laser, 6 of whom with
KTWS (2). Since then, endoscopic treatment with Nd:YAG laser has been
advocated as the gold standard procedure for bladder hemangiomas. In Case
5, the endoscopic approach was used with some technical aspects differing
from those described in the literature. We used saline solution to fill
the bladder as opposed to CO2 utilized by Kato (12). Since the lesion
was very large, our strategy was to initially coagulate the margins of
the lesions, in order to decrease blood supply to the bleeding sites.
Next, we applied the laser directly to the central areas with large veins,
which resulted in bleeding that was easily controlled by applications
in the base of the veins. The immediate and mid-term results were excellent,
without recurrence of bleeding for more than one year.
The trigone and bladder neck are reported
to be rarely involved, but two of our patients (cases 3 and 5) had involvement
of the posterior bladder wall and trigone, including obstruction of the
left ureteral orifice in Case 3. This is the fourth reported case of KTWS
causing hydronephrosis (1,8). Furness et al. described the treatment of
one of such cases with ureterolysis. In this case, due to extensive vesical,
retroperitoneal and pelvic involvement, the patient was managed conservatively
with insertion of a ureteral Double-J catheter to preserve the renal function.
Urethral bleeding is extremely rare in patients
with KTWS. We found only one case in the literature, which was treated
with excision of the affected urethral segment and full-thickness skin
graft. Other cases of urethral bleeding caused by hemangiomas or vascular
malformations and not associated to KTWS were treated by excision, Nd:YAG
or KTP laser (17,18). Three of our cases had episodes of urethral bleeding.
In Case 4, it was controlled with Holmium laser applications on the varicose
veins, which to our knowledge represents the first successful report of
such treatment. Case 6 had only one self-limited episode of urethral bleeding,
and urethrocystoscopy revealed a small prostatic urethra lesion that was
not treated. In case 3, the episodes have been mild and sporadic, and
no therapy was needed.
Genital lesions are usually managed conservatively.
Ulcerations or small bleeding areas are treated with topical antibiotics
and compressive dressings. Significant deformity of the penis can be managed
with postectomy when necessary. It is usually a safe procedure but may
require surgical revision, as occurred in Case 2. Since vascular malformations
are not hemangiomas, treatments with steroids, sclerotherapy and radiation
are not indicated (1). Phimosis can be managed by circumcision. However,
careful dissection is necessary, due to the possibility of anomalous enlarged
subcutaneous veins, as seen in case 6.
KTWS lesions are not malignant but can have
a malignant behavior according to their size and location, as seen in
Case 3. Life expectancy for patients with KTWS is not determined in the
literature, but adulthood can be reached and many cases of successful
pregnancy and delivery have been reported (19). Patients with KTWS must
have adequate support and treatment. Vascular and plastic surgeries can
ameliorate aesthetical aspects, improving quality of life (17,20). Urologists
can have an important role in the care of these patients and must be prepared
for that.
CONCLUSIONS
Urogenital involvement in the Klippel-Trenaunay-Weber Syndrome must be suspected when hematuria or urethral bleeding occurs or when extensive cutaneous lesions of the pelvis, genitals, lower extremities and buttocks are present. Imaging studies and urethrocystoscopy confirm the diagnosis. Genital cutaneous malformations may be treated surgically when associated to severe deformity. Hematuria and urethrorrhagia are often managed conservatively, but life-threatening or recurrent episodes should be treated endoscopically. Laser seems to be a good therapeutic option for bleeding vesical or urethral lesions, but the best type of laser for this purpose is yet to be determined.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Furness PD 3rd, Barqawi AZ, Bisignani G, Decter RM: Klippel-Trenaunay syndrome: 2 case reports and a review of genitourinary manifestations. J Urol. 2001; 166: 1418-20.
- Smith JA Jr: Laser treatment of bladder hemangioma. J Urol. 1990; 143: 282-4.
- Tian XL, Kadaba R, You SA, Liu M, Timur AA, Yang L, et al.: Identification of an angiogenic factor that when mutated causes susceptibility to Klippel-Trenaunay syndrome. Nature. 2004; 427: 640-5.
- Ziyeh S, Spreer J, Rossler J, Strecker R, Hochmuth A, Schumacher M, et al.: Parkes Weber or Klippel-Trenaunay syndrome? Non-invasive diagnosis with MR projection angiography. Eur Radiol. 2004; 14: 2025-9.
- Hamsher JB, Farrar T, Moore TD: Congenital vascular tumors and malformations involving urinary tract: diagnosis and surgical management. J Urol. 1958; 80: 299-310.
- Campistol JM, Agusti C, Torras A, Campo E, Abad C, Revert L: Renal hemangioma and renal artery aneurysm in the Klippel-Trenaunay syndrome. J Urol. 1988; 140: 134-6.
- Fligelstone LJ, Campbell F, Ray DK, Rees RW: The Klippel-Trenaunay syndrome: a rare cause of hematuria requiring nephrectomy. J Urol. 1994; 151: 404-5.
- Yildizdas D, Antmen B, Bayram I, Yapicioglu H: Klippel-trenaunay-Weber syndrome with hydronephrosis and vesicoureteral reflux: an unusual association. Turk J Pediatr. 2002; 44: 180-2.
- Katsaros D, Grundfest-Broniatowski S: Successful management of visceral Klippel-Trenaunay-Weber syndrome with the antifibrinolytic agent tranexamic acid (cyclocapron): a case report. Am Surg. 1998; 64: 302-4.
- Klein TW, Kaplan GW: Klippel-Trenaunay syndrome associated with urinary tract hemangiomas. J Urol. 1975; 114: 596-600.
- Borrelli M, Glina S, Wroclavski ER, Lucon AM, Denes FT, Goes GM: Vesical haemangioma. Report of two cases. Int Urol Nephrol. 1984; 16: 109-14.
- Kato M, Chiba Y, Sakai K, Orikasa S: Endoscopic neodymium:yttrium aluminium garnet (Nd:YAG) laser irradiation of a bladder hemangioma associated with Klippel-Weber syndrome. Int J Urol. 2000; 7: 145-8.
- Vicente J, Salvador J: Neodymium:YAG laser treatment of bladder hemangiomas. Urology. 1990; 36: 305-8.
- Smith JA Jr, Dixon JA: Neodymium:YAG laser irradiation of bladder hemangioma. Urology. 1984; 24: 134-6.
- Shekarriz B, Upadhyay J, Smith C, Kazmers A, Frontera R: Massive hematuria in adults with Klippel-Trenaunay syndrome associated with vascular malformation of the bladder. Urol Int. 2000; 64: 226-8.
- Zini L, Amara N, Graziana JP, Villers A, Biserte J, Mazeman E: Klippel-Trenaunay syndrome and multiple vesical hemangiomas: treatment with Neodymium:YAG laser. Prog Urol. 2001; 11: 1282-4.
- Lauvetz RW, Malek RS, Husmann DA: Treatment of extensive urethral hemangioma with KTP/532 laser. Lasers Surg Med. 1996; 18: 92-5.
- Maeda K: A successful case of urethral reconstruction in a child with persistent urethral bleeding due to an extensive cavernous haemangioma. Br J Plast Surg. 1984; 37: 536-8.
- Rebarber A, Roman AS, Roshan D, Blei F: Obstetric management of Klippel-Trenaunay syndrome. Obstet Gynecol. 2004; 104: 1205-8.
- Jacob AG, Driscoll DJ, Shaughnessy WJ, Stanson AW, Clay RP, Gloviczki P: Klippel-Trenaunay syndrome: spectrum and management. Mayo Clin Proc. 1998; 73: 28-36.
____________________
Accepted
after revision:
June 10, 2006
_______________________
Correspondence address:
Dr. Francisco Tibor Dénes
Av. Enéas de Carvalho Aguiar, 255 / sala 710F
São Paulo, SP, 05403-000, Brazil
Fax: + 55 11 3069-8081
E-mail: f.c.denes@br2001.com.br
EDITORIAL COMMENT
The
Klippel-Trenaunay syndrome (KTS) is an unusual congenital anomaly. It
causes symptoms due to genitourinary system involvement in approximately
6% of the cases (1).
The
most feared urological complication is recurrent gross hematuria due to
bladder involvement, which could be quite difficult to manage. The paper
has a substantial number of KTS patients with genitourinary involvement
but in this series none of the patients suffered from recurrent bleeding
following treatment, which may not always be the case. The authors described
2 cases of gross hematuria, one case was initially treated with radiotherapy,
which caused contracted bladder; it is not the recommended treatment in
such patients. In the second case a massive hemangiomatous lesion was
successfully treated with Nd: YAG laser in a single session. Another case,
which had extensive bladder hemangiomatous lesions, did not cause any
bleeding but caused obstruction to the upper tracts. It was managed by
insertion of double J stent through the lesion, which could be technically
demanding and lead to local irritation, and precipitation of hematuria.
The rest of the cases were dealt straightforwardly.
Most
publications regarding genitourinary manifestations in Klippel Trenaunay
syndrome comprise of individual case reports and as the presentation is
variable there is no gold standard in treatment. Amongst many options
available, Nd: YAG laser has been most commonly and successfully employed
as the first line treatment for bleeding from these hemangiomatous lesions.
Recently a newer treatment with systemic alpha-interferon has been used
in a single patient with problematic recurrent hematuria with good short-term
results (2).
These
patients need long term and close follow up. Any benefit of treating bladder
and urethral lesions prophylactically remains to be established. However,
the lesions in Klippel Trenaunay syndrome are not true hemangiomas but
it may be worthwhile to evaluate any long-term role of endothelial cell
growth inhibitors like interferon alpha-2a in preventing bleeding.
REFERENCES
- Furness PD 3rd, Barqawi AZ, Bisignani G, Decter RM: Klippel Trenaunay Syndrome: 2 case reports and a review of genitourinary manifestations. J Urol. 2001; 166: 1418-20.
- Ahmed I, Aslam M, Mahfooz A, Hanash K: Genitourinary manifestations of Klippel- Trenaunay syndrome: report of 2 cases managed with systemic interferon. Scand J Urol Nephrol. 2005; 39: 523-6.
Dr.
I. Ahmed
Department of Urology
King Faisal Specialist Hosp & Research Ctr
Riyadh, Saudi Arabia
E-mail: ahmedirfan2000@hotmail.com