ROBOTIC
ASSISTED RADICAL PROSTATECTOMY: SURGICAL TECHNIQUES AND OUTCOMES
(
Download pdf )
JOSE R. COLOMBO JR, BRUNO SANTOS, JASON HAFRON, TROY GIANDUZZO, GEORGES-PASCAL HABER, JIHAD H. KAOUK
Section of Laparoscopic and Robotic Surgery, Glickman Urological Institute, Cleveland Clinic, Cleveland, Ohio, USA
ABSTRACT
Robotic assisted radical prostatectomy (RARP) is gaining acceptance and popularity among urologists all over the world. Early oncologic and functional results are encouraging. In this manuscript, we describe in detail both approaches for RARP and show the results of the robotic surgery program with over 300 RARP performed at our institution.
Key
words: prostate cancer; laparoscopy; robotic surgery; prostatectomy
Int Braz J Urol. 2007; 33: 803-9
INTRODUCTION
Robotic
assisted radical prostatectomy (RARP) provides several advantages such
as precise dissection through improved instrument control with articulating
tips, 3-dimensional vision and magnified view (10x), intuitive eye-hand
coordination, motion scaling and filter of tremor. However, the best benefit
offered by the surgical robotic is minimizing the steep learning curve
set by the laparoscopic approach for radical prostatectomy (1).
Since it was first described in 2001 (2,3)
the robotic assisted radical prostatectomy (RARP) is gaining acceptance
and popularity among urologists all over the world. Our minimally invasive
radical prostatectomy program was initiated in 1999 with over 1000 cases
performed at this time. The robotic program was introduced in 2001 after
a significant experience with the pure laparoscopic approach, with over
350 robotic cases performed up to date. Herein we describe in detail,
the step-by step surgical technique of RARP, using the da Vinci S Surgical
System (Intuitive Surgical, Sunnyvale, California, USA), and also discuss
the perioperative outcomes.
SURGICAL TECHNIQUE
Transperitoneal Approach
Patient
preparation: A minimum period of 6 weeks between the prostate biopsy and
the operation is recommended. Anti-platelet agents are discontinued 2
weeks prior to the surgery and a clear liquid diet is given 18 hrs before
the surgery.
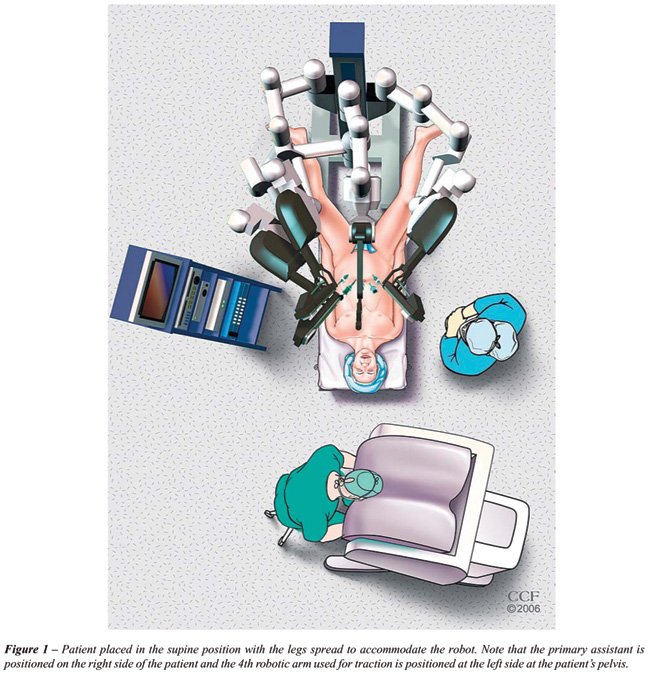
Patient positioning: All patients receive
prophylactic parenteral third generation cephalosporin antibiotics and
compression stockings prior to the procedure. No subcutaneous heparin
is used. After induction of general endotracheal anesthesia, the patient
is positioned in the supine position and is adequately padded at all pressure
points, with arms placed at patient’s side. The legs are separated
in semi flexion (lithotomy position) and a 20F Foley catheter is inserted
into the bladder. The operating table is maintained in a significant Trendelenburg
position for the duration of the procedure (Figure-1).
Pneumoperitoneum: A Veress needle is inserted
at the periumbilical position, the pneumoperitoneum is established initially
at 20 mmHg for adequate port positioning, and then lowered to 12-15 mmHg.
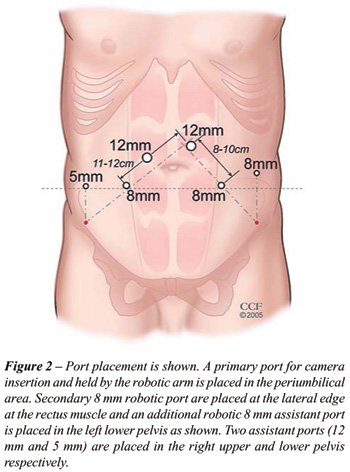
Port placement: The Veress needle is replaced
by a 12 mm port and the laparoscope is introduced for initial abdomen
inspection. Under direct vision, four additional trocars are placed: three
8 mm da Vinci trocars and an extra 12 mm regular port are positioned as
shown in Figure-2.
Bladder mobilization: After a complete inspection
of the abdominal cavity performed using a 30° scope, lysis of adhesions
is performed. After docking the robot, the extraperitoneal space is entered
through an inverted U-shaped incision in the parietal peritoneum is made,
superiorly to include the urachus, and laterally to medial umbilical ligaments.
The third robotic arm, available in the new da Vinci system, is used to
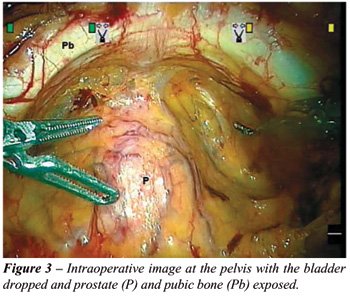
assist in counter traction and exposure. After the medial umbilical ligaments
and urachus are incised, and the Retzius space entered, the pubic bone
and the iliac vessels are identified and exposed (Figure-3).
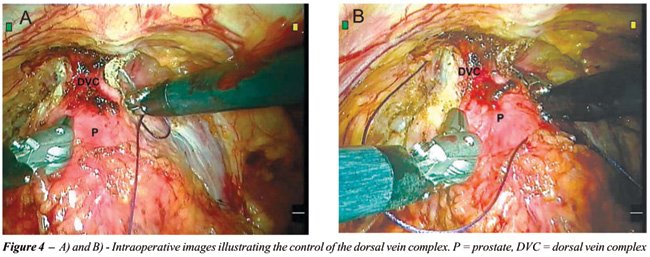
Dorsal vein complex (DVC) control: The fatty
tissue covering the prostate is dissected and the endopelvic fascia and
the anterior surface of the prostate is exposed. The superficial dorsal
vein is precisely coagulated and divided with robotic bipolar cautery.
The endopelvic fascia is then incised bilaterally, using no thermal energy
with the robotic scissors. The DVC complex is then secured with 0-vicryl
on CT-1 needle, and divided at a later stage of surgery with the robotic
J-hook (Figure-4). Urethral metal sound helps keeping the urethra away
from the DVC during suturing. A second stitch is placed towards the prostatic
base and used to control bladder neck vessels and aid in retraction of
the prostate during the dissection of the bladder neck.
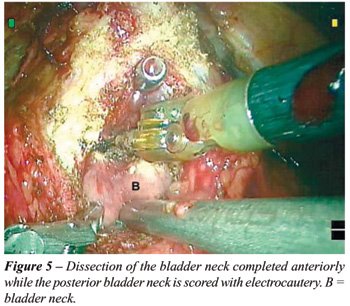
Division of the bladder neck: With the prostate
retracted cephalad, the anterior bladder neck dissection is performed
with the metal sound used to aid identify the bladder neck. An opening
in the bladder neck is created with the robotic J-hook, and then with
the third robotic arm retracting the prostate towards the abdominal wall,
the bladder neck incision is prolonged horizontally. The assistant provides
adequate visualization with suction, and appropriate traction during this
step. The posterior aspect of the bladder neck is identified and dissected
at the prostatovesical junction, starting from the midline and extended
laterally to completely detach the bladder neck of the base of the prostate.
In the presence of a large median lobe, ideally the ureteral meatus should
be identified before initiating the posterior bladder neck incision (Figure-5).
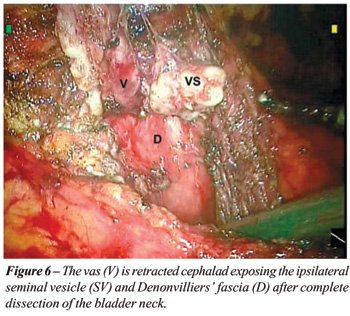
Vas deferens and seminal vesicles dissection:
After completing the dissection of the prostate base, both vas deferens
are identified and cut, keeping a long stump of vas for retraction. The
dissection continues by pulling the vas cephalad away from the rectum
thus exposing the seminal vesicles that are located lateral to the vas
on each side. Dissection is done mainly by blunt dissection with robotic
scissors. When necessary 5 mm Hem-o-lock clips (Weck Closure Systems,
Research Triangle Park, NC, USA), or harmonic scalpel are applied to control
the seminal vesicular and vasal arteries. After a complete release of
seminal vesicles and vas, the third robotic arm is used to pull up both
seminal vesicles, while the assistant provides help with adequate suction,
to expose the prostate lateral pedicle. The lateral prostatic pedicle
is clipped or cut with harmonic scalpel (Figure-6).
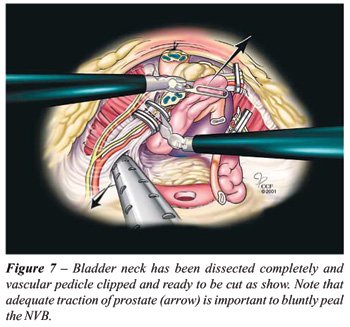
Neurovascular bundle (NVB) dissection (nerve
sparing): This step is performed under the view of a 0° laparoscope
lens, without employing any thermal energy to optimize the NVB preservation.
The NVB is released from the posterolateral aspect of the prostate using
a combination of sharp and blunt dissection, using robotic scissors and
prograsper. Using robotic scissors, the superficial prostatic fascia is
incised and the neurovascular bundle is peeled bluntly. This dissection
is extended laterally and distally towards the prostate apex (Figure-7).
Prostate apex and urethral dissection: This
step is crucial for postoperative continence and oncological control.
The prostate is retracted cephalad out of the pelvis, and the prostate
apex is bluntly dissected without compromise the NVB integrity with any
thermal injury. The previously ligated DVC is cut using J hook cautery.
The urethra is incised with robotic scissors anteriorly and then completely
divided. A 10 mm Endocatch bag (US Surgical, Norwalk, CT, USA) is used
for specimen store and retrieval at the end of the procedure.
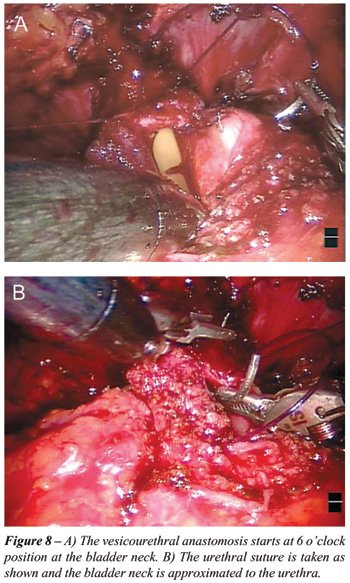
Vesicourethral anastomosis: Two monocryl
2-0 sutures on a UR-6 needle are used to complete the vesicourethral anastomosis
then the two sutures are tied to each other. The van Velthoven running
suture technique is used, starting at 6 o’clock position in the
posterior bladder neck, progressing towards 12 o’clock, one in a
clockwise and the other in an anti-clockwise fashion. The bladder is firstly
brought close to the urethra when the anastomosis reaches 9 and 3 o’clock
positions respectively, then a 20 Fr Foley catheter is inserted (Figures-8A
and 8B).
Ports closure: The retrieval of the laparoscopic
bag with the intact specimen is made through the extension of the periumbilical
12 mm port site. A Jackson-Pratt drain is placed in the vicinity of the
vesicourethral anastomosis through a lateral 5 mm port site. The Carter
Thomason device is used to close the 12 mm port sites.
Extraperitoneal Approach
Patient
positioning: During this approach, the patient is positioned in supine
position, with arms along the body in a similar fashion to the transperitoneal
approach. The legs are separated in semi flexion (lithotomy position)
with a 20F Foley catheter inserted into the bladder. The operating table
is maintained in a slight Trendelenburg position for this approach.
Pneumoperitoneum: Using a 2 cm midline incision
made 1 cm inferior to the umbilicus, the subcutaneous layer is divided
deep to the anterior rectus fascia, which is incised transversally and
separated in the linea alba. A limited extraperitoneal space is initially
developed bluntly with index finger dissection along the posterior rectus
sheath. This space is bordered caudally by the arcuate line of Douglas,
posteriorly by the posterior rectus sheath, anteriorly by the posterior
fibers of the rectus muscle. A balloon dissector (US surgical) is then
introduced through the developed space and inflated gradually up to 400
cc of air then deflated and removed.
Port placement: A special trocar (12 mm)
with 30 cc balloon mounted tip (US Surgical) is placed at the initial
umbilical incision. Under direct vision, four additional trocar are placed:
three 8 mm da Vinci trocars and an extra 12 mm regular port are positioned.
The Retzius space is opened and the prevesical space is developed laterally.
The anterior aspect of the bladder, the pubic arch and the external iliac
vessels are visualized. The procedure is continued in a similar fashion
as in the transperitoneal approach as describe above.
RESULTS
A
prospective data collection at 250 RARP has been completed. The mean age
of the patients was 60.5 ± 6.9 years, with BMI of 28.7 ±
3.7, mean preoperative PSA of 6.2 ± 3.4 ng/mL, and median Gleason
score on the preoperative prostate biopsy of 6 (IQR 6,7). Overall, 9%
of the patients had a previous abdominal surgery, with a median ASA score
was 2 (IQR 2,3).
The mean operative time was 200 ±
61 min; of these, vesicourethral anastomosis took 24 ± 11 min to
perform. The estimated blood loss was 250 mL (IQR 150,350), with blood
transfusion rate of 1.9%, perioperative complication rate of 1.2%, and
overall positive margin rate of 12%. Mean hospital stay was 1.8 ±
1.1 days since the admittance.
No significant difference was noted between
the transperitoneal and the extraperitoneal approaches as regards blood
loss, blood transfusion rate, operative time, intraoperative urine output,
urethrovesical anastomosis time, positive margins, and complications.
COMMENTS
Since
the introduction of the AESOP (Computer Motion, Goleta, California, USA)
in 1994 and the da Vinci Surgical System in 1997, the introduction of
surgical robots is growing in a fast pace. Over 150 hospitals in United
States and Europe are currently performing robotic assisted surgery and
this trend is growing (4).
The major drawback for robotic surgery is
high cost, including the robotic system, disposable instruments, operating
room facilities, training personnel, and maintenance. The multidisplinary
use and marketing strategies are the main allies of the surgeon at the
initiation of a robotic program, which depends on surgical volume and
indirect referrals to the health center. Urology, gynecology, general
surgery, and cardiothoracic surgery are currently using robotic assisted
procedures regularly.
The minimally invasive approach offers less
morbidity compared to open radical prostatectomy, and available data shows
comparable results between the robotic assisted and pure laparoscopic
techniques, with the former presenting a reduced learning curve for technically
demanding operations, mainly due to three dimensional visualization and
enhanced surgical dexterity (5-7). Improvement in available surgical robots
will further enhance the wide spread use of robotics.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Menon M, Tewari A, Peabody JO, Shrivastava A, Kaul S, Bhandari A, et al.: Vattikuti Institute prostatectomy, a technique of robotic radical prostatectomy for management of localized carcinoma of the prostate: experience of over 1100 cases. Urol Clin North Am. 2004; 31: 701-17.
- Abbou CC, Hoznek A, Salomon L, Olsson LE, Lobontiu A, Saint F, et al.: Laparoscopic radical prostatectomy with a remote controlled robot. J Urol. 2001; 165: 1964-6.
- Pasticier G, Rietbergen JB, Guillonneau B, Fromont G, Menon M, Vallancien G: Robotically assisted laparoscopic radical prostatectomy: feasibility study in men. Eur Urol. 2001; 40: 70-4.
- Steers WD, LeBeau S, Cardella J, Fulmer B: Establishing a robotics program. Urol Clin North Am. 2004; 31: 773-80.
- Bentas W, Wolfram M, Jones J, Brautigam R, Kramer W, Binder J: Robotic technology and the translation of open radical prostatectomy to laparoscopy: the early Frankfurt experience with robotic radical prostatectomy and one year follow-up. Eur Urol. 2003; 44: 175-81.
- Ahlering TE, Skarecky D, Lee D, Clayman RV: Successful transfer of open surgical skills to a laparoscopic environment using a robotic interface: initial experience with laparoscopic radical prostatectomy. J Urol. 2003; 170: 1738-41.
- Menon M, Tewari A, Baize B, Guillonneau B, Vallancien G: Prospective comparison of radical retropubic prostatectomy and robot-assisted anatomic prostatectomy: the Vattikuti Urology Institute experience. Urology. 2002; 60: 864-8.
________
Accepted:
June 25, 2007
_______________________
Correspondence address:
Dr. Jihad H Kaouk
Section of Laparoscopic and Robotic Surgery
Glickman Urological Institute, Cleveland Clinic
9500 Euclid Av, A100
Cleveland, OH 44195
Fax: + 1 216 445-2267
E-mail: kaoukj@ccf.org