PURE
ROBOTIC RETROCAVAL URETER REPAIR
(
Download pdf )
ASHOK K. HEMAL, RANJIT RAO, SACHIT SHARMA, RHYS G. E. CLEMENT
Department of Urology (AKH) , Wake Forest University Health Sciences, Winston-Salem, North Carolina, USA and Department of Urology (RR, SS, RGEC), All India Institute of Medical Sciences, New Delhi, India
ABSTRACT
Purpose:
To demonstrate the feasibility of pure robotic retrocaval ureter repair.
Materials and Methods: A 33 year old female
presented with right loin pain and obstruction on intravenous urography
with the classical “fish-hook” appearance. She was counseled
on the various methods of repair and elected to have a robot assisted
repair. The following steps are performed during a pure robotic retrocaval
ureter repair. The patient is placed in a modified flank position, pneumoperitoneum
created and ports inserted. The colon is mobilized to expose the retroperitoneal
structures: inferior vena cava, right gonadal vein, right ureter, and
duodenum. The renal pelvis and ureter are mobilized and the renal pelvis
transected. The ureter is transposed anterior to the inferior vena cava
and a pyelopyelostomy is performed over a JJ stent.
Results: This patient was discharged on
postoperative day 3. The catheter and drain tube were removed on day 1.
Her JJ stent was removed at 6 weeks postoperatively. The postoperative
intravenous urography at 3 months confirmed normal drainage of contrast
medium.
Conclusion: Pure robotic retrocaval ureter
is a feasible procedure; however, there does not appear to be any great
advantage over pure laparoscopy, apart from the ergonomic ease for the
surgeon as well the simpler intracorporeal suturing.
Key
words: ureter; vena cava; abnormalities; laparoscopy; robotics
Int Braz J Urol. 2008; 34: 734-8
INTRODUCTION
Retrocaval
ureter is an unusual urological problem that may require operative repair
(Figure-1). The first case of retrocaval ureter repair was published in
1949 by Anderson and Hynes (1). The classical approach is an open technique
of transposing the ureter anteriorly to the inferior vena cava followed
by ureteroureterostomy. Laparoscopic retrocaval ureter repairs have also
been performed but can be technically challenging. This is the first case
of a pure robotic repair, to our knowledge, performed in an adult. We
present our robotic technique of pure robotic retrocaval ureter repair.

SURGICAL TECHNIQUE
1.
Patient position - The patient is positioned in a modified flank position
over the kidney break at a 45 degree angle. The patient is then adequately
secured with supports and strapping, and all pressure areas are protected.
2. Port position - A Veres needle is used
to create a pneumoperitoneum, then a 10 mm port is inserted for the camera
at the level of the umbilicus just lateral to the rectus abdominis muscle.
Two 8 mm ports are inserted for the robotic arms, one under the costal
margin in the midclavicular line and the other at two thirds of the way
along McBurney’s line (anterior superior iliac spine and umbilicus).
A further 5 mm port is inserted 3 cm below the camera port for the assistant
to perform retraction and suction. The robot is then docked. The whole
process of pneumoperitoneum, port insertion and docking takes 15 minutes.
3. Colon mobilization - The hepatic flexure
and right colon are mobilized medially to provide exposure to the right
retroperitoneal structures.
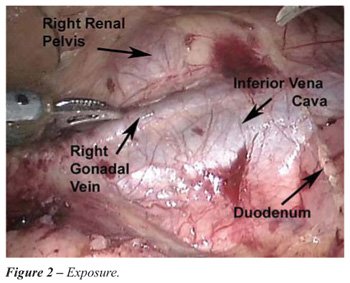
4. Exposure of retroperitoneal structures:
(Figure-2). The right renal pelvis, inferior vena cava, right gonadal
vein, right ureter and duodenum are all identified.
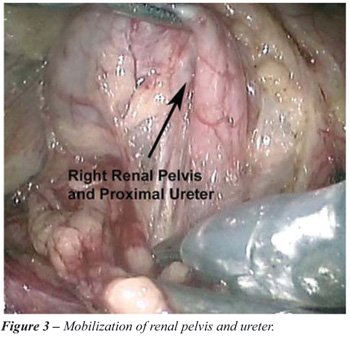
5. Mobilization of renal pelvis and ureter:
(Figure-3). The right renal pelvis is dissected free from its surrounding
fascial layers. The proximal right ureter is dissected free where it can
be seen to disappear superiorly under the inferior vena cava.
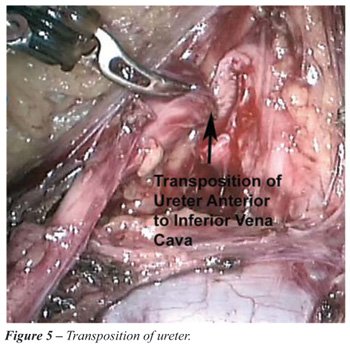
6. Transection of ureteropelvic junction:
(Figure-4). The renal pelvis is transected and the ureteropelvic junction
along with the retrocaval segment are transposed anterior to the inferior
vena cava (Figure-5) in preparation for a pyelopyelostomy. This may not
be possible for lower segment retrocaval ureters in which case ureteroureterostomy
must be performed.

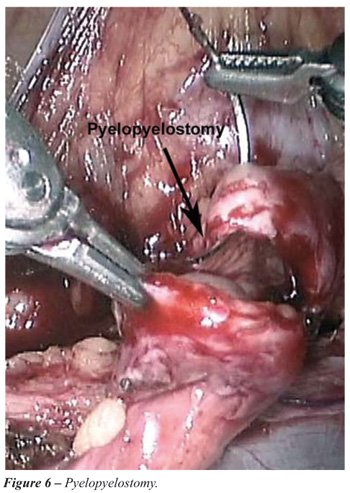
7. Pyelopyelostomy: (Figure-6). Performing
a pyelopyelostomy is easier than a ureteroureterostomy and one is less
likely to produce stricture formation due to the larger caliber structures
as well as the better blood supply as one goes more superiorly. This is
performed with 40 polygalactin suture material in an interrupted fashion.
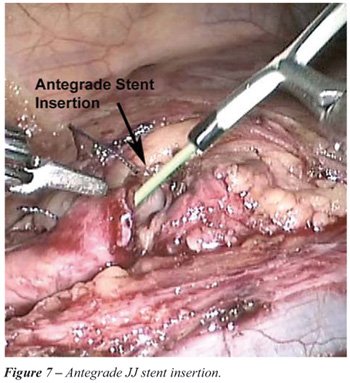
8. Antegrade JJ stent insertion: (Figure-7).
Prior to closing the anastomosis, a 6F JJ stent is inserted in an antegrade
fashion. The stent with the wire is introduced via the 5 mm port. It is
grasped using the robotic needle holder, introduced into the ureter and
passed down to the bladder.
9. Drain tube insertion: The robot is undocked
and a drain tube is inserted via the 5-mm port. The 10 mm port is closed
in standard fashion and an indwelling catheter is left in situ.
RESULTS
This
33 year old female patient was discharged on postoperative day 3. The
catheter and drain tube were removed on day 1. The JJ stent was removed
at 6 weeks post operatively. The post operative IVU at 3 months confirmed
normal drainage of contrast (Figure-8).

COMMENTS
Robotic
technology has become incorporated into certain areas of urology as in
robotic prostatectomy and has become well accepted. Reconstructive urology
represents a challenge for the robotic urologist to offer this technology
safely, with efficacy over proven techniques and without increased morbidity.
Our case demonstrates the feasibility of
a procedure using the robot but does not necessarily justify its use over
other modalities. Though the fundamental surgical principles of a tension
free, well vascularized anastamosis remain the same, patients may now
receive the benefits of a minimally invasive approach, namely: smaller
incision; better cosmetic effect, decreased pain; shorter hospital stay
and a quicker return to normal activities. This holds true for both a
pure laparoscopic or pure robotic approach.
Pure laparoscopic repair of the retrocaval
ureter has been performed both transperitoneally and retroperitoneally
(2). We have previously published our results with retroperitoneal ureterolysis
and retrocaval ureter repair (3). Pure laparoscopic repair remains a technically
challenging procedure, but in experts hands the results are excellent.
The robotic approach to retrocaval ureter
was first published for a pediatric patient by Gundeti et al. in 2006
(4). Pyelopyelostomy with preservation of the retrocaval segment was first
performed for a retrocaval ureter by Simfiroosh et al. in 2006 in a pure
laparoscopic procedure (5). This preservation of the retrocaval segment
does not appear to hinder drainage and it makes the anastamosis far easier
to perform and may lead to a lower stricture rate.
The main advantage of the robotic technology
is the ease of dissection and intracorporeal suturing. Expert laparoscopic
surgeons may argue that there is no need for the robot in such a procedure
in the same way that laparoscopic pyeloplasty can be done without the
robot. This of course is true, however the fact remains that new technologies
emerge and it seems that robotic technology is here to stay. The downside
to the robotic approach is of course the cost.
Since acquiring the da-Vinci-S robot in
2006 we have performed many reconstructive procedures such as megaureter
repair and pyeloplasty with robotic assistance. This is the first retrocaval
ureter repair that we have performed using the robot.
CONCLUSION
We demonstrated in this case that pure robotic retrocaval ureter repair is feasible. Apart from the ergonomic and technical benefits that the robotic approach gives the surgeon, there does not appear to be any other advantage over laparoscopy.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Anderson JC, Hynes W: Retrocaval ureter; a case diagnosed pre-operatively and treated successfully by a plastic operation. Br J Urol. 1949; 21: 209-14.
- Matsuda T, Yasumoto R, Tsujino T: Laparoscopic treatment of a retrocaval ureter. Eur Urol. 1996; 29: 115-118.
- Gupta NP, Hemal AK, Singh I, Khaitan A: Retroperitoneoscopic ureterolysis and reconstruction of retrocaval ureter. J Endourol. 2001; 15: 291-3.
- Gundeti MS, Duffy PG, Mushtaq I: Robotic-assisted laparoscopic correction of pediatric retrocaval ureter. J Laparoendosc Adv Surg Tech A. 2006; 16: 422-4.
- Simforoosh N, Nouri-Mahdavi K, Tabibi A: Laparoscopic pyelopyelostomy for retrocaval ureter without excision of the retrocaval segment: first report of 6 cases. J Urol. 2006; 175: 2166-9; discussion 2169.
____________________
Accepted after revision:
August 28, 2008
_______________________
Correspondence address:
Dr. Ashok K Hemal
Department of Urology
Wake Forest University School of Medicine
Medical Center Boulevard
Winston-Salem, NC, 27157, USA
Fax: + 1 336 716-5711
E-mail: ahemal@wfubmc.edu