TRANSOBTURATOR
MALE SLING TOMSTM FOR THE TREATMENT OF STRESS POST-PROSTATECTOMY INCONTINENCE,
INITIAL EXPERIENCE AND RESULTS WITH ONE YEAR’S EXPERIENCE
(
Download pdf )
doi: 10.1590/S1677-55382009000600009
PHILIPPE GRISE, MARC GERAUD, JEAN LIENHART, BENOIT LE PORTZ, MICHAEL BUBENHEIM, PIERRE COSTA
Department of Urology (PG) and Department of Biostatistics (MB), Rouen University Hospital, Rouen, France, Department of Urology (MG), Polyclinique Saint Come, Compiegne, France, Department of Urology (JL), Clinique Trenel, Sainte Colombe, France, Department of Urology (BP), Clinique Oceane, Vannes, France, Department of Urology (PC), Nimes University Hospital, Nimes, France
ABSTRACT
Purpose:
Post-prostatectomy incontinence remains a problem, even in minor or moderate
degrees. In order to minimize surgical morbidity and costs, sling procedures
have been proposed. The authors have developed a new transobturator male
sling procedure and report their results after one-year experience.
Materials and Methods: A prospective multicenter
study was conducted in 50 patients with minor or moderate post-prostatectomy
incontinence. Evaluation of TOMSTM two arms bulbar sling was based on
clinical form assessment, The International Consultation on Incontinence
Questionnaire (ICIQ) and short-form (SF) 36 questionnaire pre and postoperatively
and at 3, 6, 9 and 12 months.
Results: The surgical procedure was considered
easy to perform and no post-surgery complication was reported except for
one retention. The median number of pads per day decreased significantly
from 2 pads before surgery (95% CI: 2 - 3) to 1 during the follow-up period
(95% CI: 0 - 2 at 360 days), and at 3 months patients using none or one
pad per day were 30% and 32% respectively. The SF 36 continence and quality
of life score improved from a median of 100 (95% CI: 83 - 133) to 300
(95% CI: 167 - 375), and the median ICIQ incontinence and quality of life
score decreased from 15 (95% CI: 14 - 16) to 8 (95% CI: 5 - 12) one year
after surgery.
Conclusion: The transobturator perineal
male sling TOMSTM is an attractive simple sling technique for moderate
or minor post-prostatectomy stress incontinence and offers an improvement
in the quality of life.
Key
words: urinary incontinence; male; urinary sphincter; prostatectomy;
surgery, sling
Int Braz J Urol. 2009; 35: 706-15
INTRODUCTION
Despite
improvement in surgical technique of radical prostatectomy, incontinence
remains a bothersome problem. The prevalence of post-prostatectomy depends
on the definition of incontinence and evaluation methods; however, studies
indicate that 5% to 55% of patients are concerned (1). Even only one pad
a day affects the quality of life (2).
For major stress urinary incontinence (SUI),
the artificial sphincter remains the gold standard technique despite a
risk of erosion or infection. As regards urethral bulking agents, they
are often disappointing even with re-injections.
In order to minimize surgical morbidity
and cost, bulbar sling procedures have been proposed of which the most
common sling used is bone-anchor fixation. Good results without significant
obstruction were obtained but concern remains regarding perineal pain
and infection of the material. Based on our experience of the female transobturator
polypropylene sling (3) we developed a new transobturator bulbar male
sling (TOMSTM) (4) in order to minimize the adverse effects of bulbar
slings. Other male transobturator slings (5-8) have also recently been
reported in the bulbar location (5,7,8) or in membranous location (6).
The benefits and our clinical results were studied in a prospective multicenter
series. The results with one year’s experience are reported.
MATERIALS AND METHODS
In a preliminary study (4) on six male cadavers in the lithotomy position,
the surgical technique was performed using a vertical perineal incision.
The bulbospongiosus muscle was dissected, then the ischiocavernous muscles,
in order to expose the perineal aponeurosis close to the ischiopubic ramus
bone and the obturator foramen situated just above the ramus. The surgical
procedure was evaluated concerning outside-inside and inside-outside transobturator
puncture in male pelvis using respectively Hemet and helical needle.
Therefore, a prospective multicenter clinical
study was conducted from May 2006 to August 2007 on 50 male patients suffering
from post prostatectomy incontinence and after a failure of physiotherapy.
Our study received Institutional Ethics Committee approval.
All surgeons were experienced in transobturator
procedure for female stress incontinence and followed the same instructions
for surgery. The number of surgeons involved was ten and their first patients
were included in this series.
A total of 50 patients were included with
minimal 12 months follow-up. Exclusion criteria were pre or post-surgery
radiation, less than one year before surgery, bladder outlet obstruction
from anastomotic or urethral stricture, bladder overactivity or bladder
hypocompliance. Only minor or moderate SUI patients according to the Stamey
definition were enrolled based on the urologist’s evaluation and
5 or less pads per day.
Pre-surgery assessments included previous
medical history, physical examination, clinical study questionnaire for
urological symptoms and number of pads per day, urodynamics (urethrocystometry,
uroflowmetry, post-void residual urine) according to the recommendations
of the International Continence Society, and cystourethroscopy to rule
out any anatomical abnormality.
The patients completed the International
Consultation on Incontinence Questionnaire – Short Form (ICIQ-SF)
(9) and the Short-Form (SF) 36 (10) questionnaire, and a visual analog
pain scale (VAS) before and after surgery.
The physician recorded post-surgery evaluations
at 1, 3, 6 and 12 months using the same evaluation except for urethrocystometry.
As regards safety assessments, potential per and post-operative hazards
were recorded on a case report form.
The sling was a monofilament polypropylene,
with macropores over 75 micrometers, non-extensible, 45 cm long x 1.4
cm large, developed by CL Medical (4). The sling is attached at each end
to a clip in order to connect it to a specific needle. Hemet or helical
needle was used according to the surgeon’s preference.
The surgical technique was performed under
spinal or general anesthesia, and a 16F Foley urethral catheter was inserted.
The patients were placed in the lithotomy position and a 6 cm median vertical
perineal incision below the inferior border of the pubic symphysis was
carried out in order to expose the bulbospongiosus muscle, then to expose
the perineal aponeurosis at the top of the triangular space delimited
laterally by each ischiocavernous muscle and medial to the bulbospongiosus.
A short 2 mm incision through the pelvic fascia afforded access to the
obturator muscle just under the ischiopubic ramus bone. A stab incision
was made at the top of the thigh, 4 cm from the median line and 4 cm below
the major adductor longus muscle. The transobturator puncture was an outside
inside with a Hemet needle. The end point of the puncture was the opening
in the pelvic fascia. After sling attachment to the needle, it was pulled
back in order to correctly implant the sling. The same procedure was repeated
on the other side. The sling was sutured to the bulbospongiosus muscle
with non-absorbable sutures, and then pulled firmly from each side in
order to obtain a 2 mm visible mark on the bulbospongiosus muscle. The
perineal body was not dissected, but in cases of rolling of the inferior
edge of the sling on the bulb, the bulb was dissected just enough to apply
it under the sling, then sutured to the sling. No retrograde urethral
pressure adjustment was performed. The incision was closed without drainage
and the urethral catheter left indwelling for 2 days. Before hospital
discharge, an uroflowmetry, a post void residual, and a pelvic pain evaluation
on VAS were obtained.
Statistical analysis - The description of
the population at baseline was done using the median, the first and the
third quartile (Q1 - Q3). As regards the trend over time, the results
of each visit were summarized using the median and a 95% confidence interval
(CI). For the graphical illustration of these trends, box-plots, as described
by Tukey (11), were used. In order to test the hypothesis of no change
between consecutive visits against the alternative that there was a change,
rank based methods were applied. As the power of these tests depends among
others on the proportion of tied observations, Wilcoxon’s test for
dependent samples was used for all tests relating to the same variable
if the first quartile at any visit was larger than zero. For all other
variables, the sign test was used in order to verify whether changes between
consecutive visits were significant. Admitting for each variable a global
level of 0.05 for answering the question whether a change occurred between
any two consecutive visits, Holm’s method was used to control for
the inflation of the risk of a Type-I error.
RESULTS
In
the cadaveric procedures, the perineal approach to the bulbar urethra
and the outside-inside or inside-outside puncture of the obturator foramen
were easily performed.
Concerning the clinical study, a total of
50 patients with a median age of 72 years (Q1 - Q3: 64 - 77) underwent
TOMSTM surgery. Incontinence was a problem for all the patients.
At least half of them wore 2 pads per day
(Q1 - Q3: 1 - 3). History of prostatic surgery was radical prostatectomy
for 48 and transurethral prostatectomy for 2 patients, the median time
between prostatectomy and surgery for SUI was 35 months (Q1 - Q3: 22 -
50).
The surgery was considered by the surgeon
as easy to perform in all the cases. The median operative time for the
procedure was 30 minutes (Q1 - Q3: 25 - 45).
No per-surgery complication was reported, and no significant intra-operative
bleeding (> 200 mL) occurred or nerve, bowel or vascular injury.
On the VAS, the median pain value the day
after surgery was 2 (95% CI: 1 - 3), then decreased significantly to 0
(95% CI: 0 - 0) at one month and remained similar for all further visits
until the end of the study.
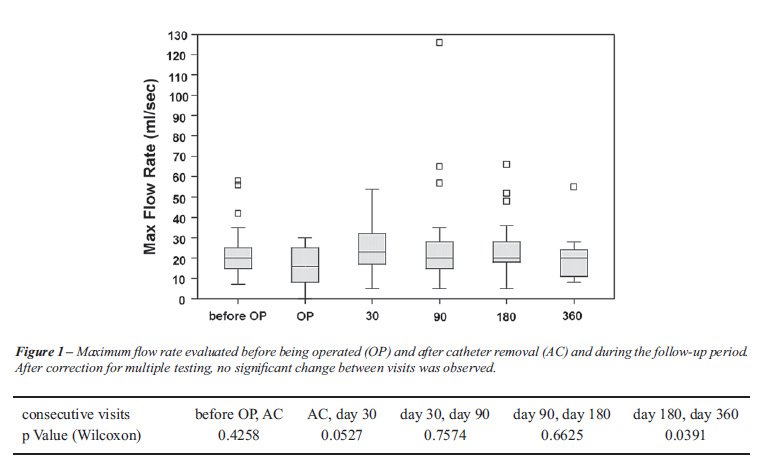
After urethral catheter removal, residual
was less than 100 mL for all the patients except one patient who experienced
urinary retention. This patient was reoperated (day 2) to release the
tension on the tape, and then a good result on micturition and continence
was obtained. A low stream was reported for one patient but this was not
bothersome. Maximal flow rate was 20 mL/sec on the median (95% CI: 17
- 24) before surgery and 16 (95% CI: 8 - 26) when evaluated after catheter
removal; the values (Figure-1) did not change significantly during the
follow-up period.
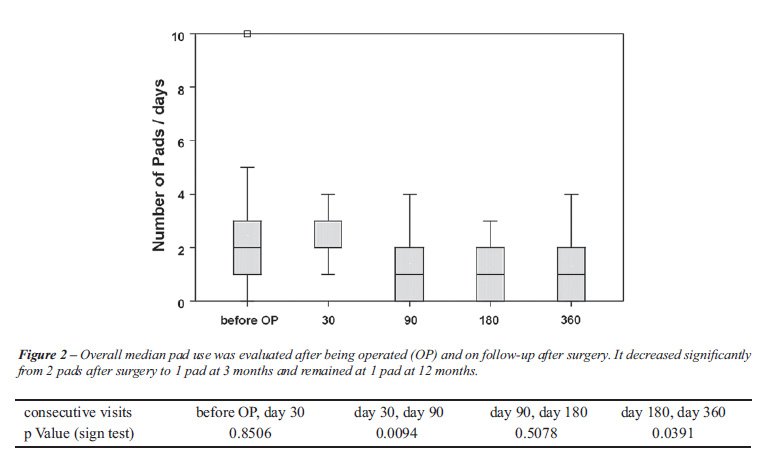
Overall median pad use decreased significantly
(p-value used sign test and is reported in Figure-2) from 2 pads per day
(Q1 - Q3: 2 - 3) before discharge and at one month, to 1 pad for all the
visits thereafter (Figure-2). At three months and during the follow-up
period to 12 months, patients using none or one pad per day were 30% and
32% respectively.
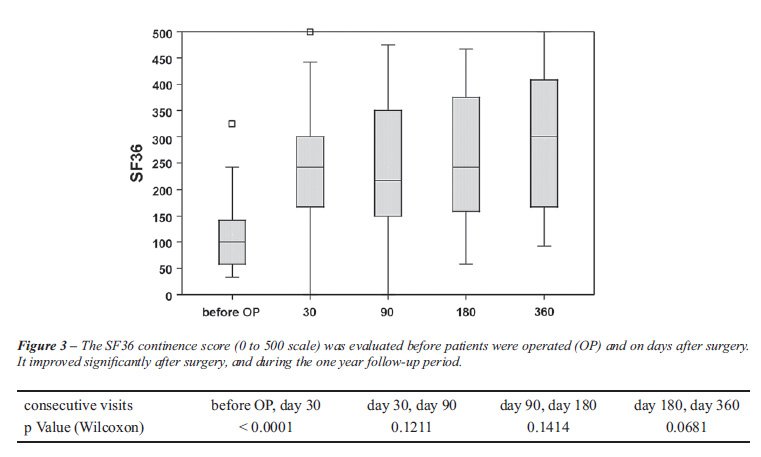
The SF36 continence scores, measured on
a scale ranging from 0 to 500 (Figure-3), improved significantly from
a median score of 100 (95% CI: 83 - 133) to 300 at one year (95% CI: 167
- 375). During the follow-up period, the median scores were 242, 217 and
267 at 1, 3 and 6 months respectively.
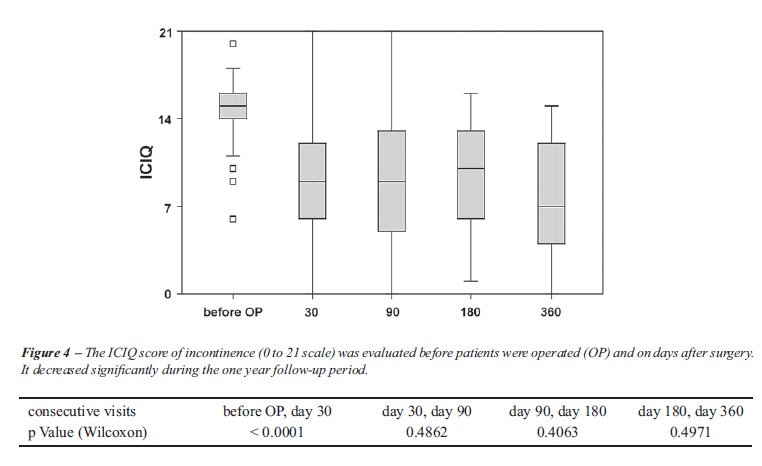
The ICIQ incontinence score (Figure-4) decreased
significantly from 15 (95% CI: 14 - 16) before the TOMS sling to 8 (95%
CI: 5 - 12) at one year, and the median score was 9 for all other visits
at follow-up.
COMMENTS
A number of minimal invasive techniques have been proposed for managing
SUI in male patients but some of them have adverse side effects or minimal
outcome measurements. Among them, the adjustable balloon is an alternative
to the sling procedure based on a mechanism of lateral compression of
the proximal urethra. Patients with none and one pad a day were reported
in 60% (12), but the high rate of per and post-surgery complications and
several adjustments were of some concern.
The artificial sphincter remains the gold
standard technique for severe incontinence due to sphincter deficiency
although the cost, the erosion or infection rate as well the need to press
the pump for each micturition, make many patients reluctant to have this
type of surgery for moderate or minor incontinence.
The concept of minimal invasive surgery
with perineal bolsters acting as a sling on the bulbar urethra was described
by Schaeffer et al. (13). Initial success rate was excellent for continence
with no significant outlet obstruction but outcome was complicated with
bolster removal due to pain, infection or erosion. The efficacy was demonstrated
on an average of four years (14) with a 42% cure rate.
In order to improve tolerance, John (15)
reported a bulbourethral composite suspension with porcine dermis and
polypropylene sling through the retropubic space. This author reported
69% continence patient with a 14-month mean follow-up. Using a retropubic
sling made of polyester plus polypropylene Xu et al. (16) achieved successful
treatment in 85% of 26 patients at 28 months.
There is a concern regarding the retropubic
route due to a risk of a bladder puncture or erosion (7), and the adhesions
due to the prostatectomy may increase the risk of using this route.
A new concept of a large perineal sling on the bulbar urethra was subsequently
introduced with the InVanceTM bone anchored male sling made of a large
triangular silicone coated biomaterial. Comiter (17) had 65% cured and
pad free patients at minimum 2 year follow-up with a polypropylene or
polyester mesh using bone anchor fixation, however up to 16 % of patients
reported perineal pain or numbness that persisted during many weeks. These
adverse effects might possibly be due to irritation in the area of the
bone screws or lesion to the perineal nerves (18) during ischiopubic rami
dissection. Moreover, infection of the biomaterial frequently occurred
due to a large silicone coated membrane instead of macroporous mesh tape,
and biomaterial characteristics may explain the morbidity including osteomyelitis
from bone screws.
Different biomaterials have been used for
the sling (allograft, porcine xenograft, synthetic, composite mesh) but
a poor outcome resulted from the non-synthetic graft (19), and the good
tolerance of polypropylene is now widely accepted. The TOMS TM polypropylene
tape is macroporous, non-extensible and the procedure is considered to
be easy. No complication was reported and tolerance was good, particularly
concerning perineal pain.
As other authors during per-surgery we did
not adjust the tension of the sling with the use of urethral pressure
value as this measurement was retrograde, not standardized in technique
and threshold. The sling was not clinically compressive for most of the
patients as confirmed on clinical records, post-void residual and uroflowmetry,
although a pressure-flow study was not conducted to document a possible
urodynamic compressive effect. Urodynamic study in 22 men by Comiter (17)
revealed that the bulbar urethral sling had no significant effects on
voiding function. Nevertheless, in our series, one patient experienced
postoperative complete retention possibly due to excess in tension or
to an acontractility bladder reflex. The decision between immediate reoperation
to release the tension on the tape, or after few days of self-catheterization
should be discussed with the patient.
The data on continence confirmed the interesting
results of the other retropubic and bone anchor bulbar urethral male slings.
As in the reported series, about 60% of the patients used none and one
pad per day at three months and during the follow-up period to 12 months.
An explanation why pad use did not change
at 30 days follow-up could be that the patients were still anxious about
leakage and used a safety pad.
Evaluation based on SF 36 scale and ICI-Q
scale showed that the continence and the quality of life improvement was
significant on both scales, and the results were maintained at one year.
Radiation was an exclusion criterion in
order to present a homogenous series as this factor adversely affects
male sling outcomes.
The transobturator route in male was initially
reported by Bauer et al. (5) in a three male cadaver study using a helical
puncture, our study confirmed this approach and added the feasibility
of oustside-inside puncture. In male patients, the transobturator tape
was reported either on membranous urethra (6) using Advance sling, or
on bulbar urethra using Argus sling (7) or De Leval sling (8) or TOMSTM
sling (4). Argus sling (7) is made of silicone and is an adjustable sling.
De Leval and Waltremy (8) used a polypropylene transobturator sling at
the same position as our sling on the bulbar urethra; they obtained continence
in 45% of their patients at 6 months. The difference between our techniques
is that they performed an additional subcutaneous lateral dissection to
tie the two lateral arms to each other, but more biomaterial and a larger
dissection were risk factors for a potential infection or perineal pain.
However, attachment of each arm to each other was probably stronger than
to rely only on the transobturator route.
The mechanism of action may need further
studies on the precise location and degree of male urethral mobility.
The AdVanceTM male sling system (6) is located more proximally on the
bulbar-membranous urethra in order to modify the mobility and to act as
a hammock-like support of the posterior sphincter complex, but tension
is also applied on the sling. A proximal dissection close to the sphincter
is a potential risk for a major deficiency; moreover, the membranous urethra
is thin and more fragile which may explain a reported case (20) of urethral
erosion.
These results using TOMSTM sling remain
encouraging but the continence results should be improved and a study
is currently ongoing with a four arm larger sling using the same biomaterial
and transobturator route.
CONCLUSION
The transobturator perineal male sling TOMSTM is an attractive technique for moderate or minor post-prostatectomy stress incontinence. The implanted biomaterial is non-mechanical, and easy to insert and well tolerated. Most of the patients were improved or continent with a one year follow-up.
CONFLICT OF INTEREST
Philippe Grise is the main investigator of the TOMSTM study (CL medical company). No financial support was provided for the study and the authors received no funding for the study. Philippe Grise received funding as an invited speaker at a symposium by Ipsen and from CL Medical companies.
ACKNOWLEDGEMENTS
The
authors are most grateful to the following researchers: Christian Saussine
(Strasbourg), Jacques Vannier (Tours), Olivier Delbos (Montpellier), Renaud
Vautherin (Sainte Colombe), François Bouchou (Tours), Denis Dupuy
(Toulouse), Patrice Lille (Moulin), Ibrahim Bah-Closel (Guilherand Granges),
Jean-Luc Hoepffner (Bordeaux), Clément Darcq (Besançon).
We also thank Richard Medeiros, Rouen University Hospital Medical Editor,
for editing the manuscript.
REFERENCES
- Lepor H, Kaci L: The impact of open radical retropubic prostatectomy on continence and lower urinary tract symptoms: a prospective assessment using validated self-administered outcome instruments. J Urol. 2004; 171: 1216-9.
- Cooperberg MR, Master VA, Carroll PR: Health related quality of life significance of single pad urinary incontinence following radical prostatectomy. J Urol. 2003; 170: 512-5.
- Grise P, Droupy S, Saussine C, Ballanger P, Monneins F, Hermieu JF, et al.: Transobturator tape sling for female stress incontinence with polypropylene tape and outside-in procedure: prospective study with 1 year of minimal follow-up and review of transobturator tape sling. Urology. 2006; 68: 759-63.
- Grise P: Incontinence after prostatectomy, The transobturator I-Stop male sling as a new treatment option. In: European Renal and Genito-Urinary Disease. Issue II. 2006; pp. 69-70.
- Bauer W, Karik M, Schramek P: The self-anchoring transobturator male sling to treat stress urinary incontinence in men: a new sling, a surgical approach and anatomical findings in a cadaveric study. BJU Int. 2005; 95: 1364-6.
- Gozzi C, Becker AJ, Bauer R, Bastian PJ: Early results of transobturator sling suspension for male urinary incontinence following radical prostatectomy. Eur Urol. 2008; 54: 960-1.
- Romano SV, Metrebian SE, Vaz F, Muller V, D’Ancona CA, Costa DE Souza EA, et al.: An adjustable male sling for treating urinary incontinence after prostatectomy: a phase III multicentre trial. BJU Int. 2006; 97: 533-9.
- de Leval J, Waltregny D: The inside-out trans-obturator sling: a novel surgical technique for the treatment of male urinary incontinence. Eur Urol. 2008; 54: 1051-65.
- Abrams P, Avery K, Gardener N, Donovan J; ICIQ Advisory Board: The International Consultation on Incontinence Modular Questionnaire: www.iciq.net. J Urol. 2006; 175: 1063-6; discussion 1066.
- Litwin MS, Lubeck DP, Henning JM, Carroll PR: Differences in urologist and patient assessments of health related quality of life in men with prostate cancer: results of the CaPSURE database. J Urol. 1998; 159: 1988-92.
- Tukey JW: Exploratory Data Analysis. Reading (MA), Addison-Wesley. 1977.
- Hübner WA, Schlarp OM: Adjustable continence therapy (ProACT): evolution of the surgical technique and comparison of the original 50 patients with the most recent 50 patients at a single centre. Eur Urol. 2007; 52: 680-6.
- Schaeffer AJ, Clemens JQ, Ferrari M, Stamey TA: The male bulbourethral sling procedure for post-radical prostatectomy incontinence. J Urol. 1998; 159: 1510-5. Erratum in: J Urol. 1998; 160: 136.
- Stern JA, Clemens JQ, Tiplitsky SI, Matschke HM, Jain PM, Schaeffer AJ: Long-term results of the bulbourethral sling procedure. J Urol. 2005; 173 :1654-6.
- John H: Bulbourethral composite suspension: a new operative technique for post-prostatectomy incontinence. J Urol. 2004; 171: 1866-70; discussion 1869-70.
- Xu YM, Zhang XR, Sa YL, Chen R, Fei XF: Bulbourethral composite suspension for treatment of male-acquired urinary incontinence. Eur Urol. 2007; 51: 1709-14; discussion 1715-6.
- Comiter CV: The male perineal sling: intermediate-term results. Neurourol Urodyn. 2005; 24: 648-53.
- Sénéchal C, Limani K, Djeffal C, Paul A, Saint F, Petit J: Perineoscrotal pain after InVance suburethral sling: Cadavre anatomical study. Prog Urol. 2008; 18: 456-61.
- Onur R, Rajpurkar A, Singla A: New perineal bone-anchored male sling: lessons learned. Urology. 2004; 64: 58-61.
- Harris SE, Guralnick ML, O’Connor RC: Urethral erosion of transobturator male sling. Urology. 2009; 73: 443. e19-20.
____________________
Accepted
after revision:
June 26,
2009
_______________________
Correspondence
address:
Dr. Philippe
Grise
Department of Urology
Rouen University Hospital-Charles Nicolle
rue de Germont
76031, Rouen, France
Fax: + 33 2 3288-8205
E-mail: philippe.grise@chu-rouen.fr
EDITORIAL COMMENT
Dr.
Grise and colleagues present an interesting experience using a transobturator
(TO) bulbar sling in the treatment of post-prostatectomy incontinence.
Indeed, the male sling is not a new concept, with the most significant
experience comprising two techniques. The first utilizes urethral compression
bolsters secured over the rectus fascia; the other a periurethral mesh
secured with bone anchors. Despite promising outcomes associated with
these sling types, widespread adoption of the male sling as a first line
surgical therapy has not been seen. More recently, a resurgence has been
seen with the introduction of TO sling types. Importantly, the work of
Dr. Grise and associates contributes to this experience and the 1-year
minimum follow-up is to be commended.
As related series are reported, it is important
that focus is placed on surgical technique as small technical differences
may affect sling efficacy. For example, both published and non-published
description of TO sling techniques detail varying degrees of perineal
body mobilization and, with it, somewhat differing locations of sling
placement along the bulbar urethra. Accordingly, sling placement in a
more proximal position may result in a vector allowing for urethra suspension/elevation,
whereas a distal location can yield a compressive action. How these differing
vectors of support affect outcomes is unknown. Indeed, the anticipated
introduction of a bulbar sling comprising both TO and prepubic arms suggests
that both vectors may be important. Future comparative study to help define
the optimal vector of support and sling position will be important.
Dr.
David Rapp
Co-Director, Virginia Urology Center for
Continence and Pelvic Floor Reconstruction
Virginia Urology Center
Richmond, Virginia, USA
E-mail: derapp@yahoo.com
EDITORIAL COMMENT
Despite
improved surgical techniques, which have led to decreased incontinence
rates, still a significant number of patients are suffering from post-prostatectomy
stress urinary incontinence (SUI) (1). Surgical treatment is the recommended
therapeutic option after non-invasive therapies have failed (2). Since
decades, the established standard for surgical treatment has been the
artificial urinary sphincter. It is, however, very expensive and associated
with high surgical revision rates (3,4). In addition, the patient needs
to have the mental and physical ability to handle the sphincter. Moreover,
minimal-invasive approaches for the treatment of SUI are more and more
demanded by patients (5). Thus, in recent years several minimal-invasive
sling systems have been intensively investigated (6-8).
In the study presented by Grise et al.,
the authors report about one year results of a new transobturator male
sling. The new sling has to be positioned like the well-known retro-urethral
transobturator sling in the region of the membranous urethra but without
splitting the bulbospongiosus muscle (9). Unfortunately, the reported
initial results are not very convincing. In the present study, a dry rate
of only 30% could be achieved. However, for the reported patient group
with a median daily pad use of 2 pads, a cure rate (no pad use) above
50% would be expected. One reason for the comparably low success rate
may have been the inclusion of the first patients treated with the new
sling system. In addition, the number of surgeons was rather high (five
implantations per surgeon on average). Thus, the study incorporates to
a large degree the surgeons’ learning curve. However, it remains
unclear if the unsatisfying dry rate is caused only by the learning curve
factor. Another limitation of this study is the measurement of urine loss
by means of daily pad use only. For a more reliable comparison of postoperative
results and to allow for a more extensive comparison with other studies,
standardized pad-tests - like the one-hour pad test or the 24-hour pad-test
- would have been desired.
Further studies with a larger patient population
and longer follow-up period will be necessary to fully assess the potential
of this new sling system.
REFERENCES
- Bauer RM, Bastian PJ, Gozzi C, Stief CG: Postprostatectomy Incontinence: All About Diagnosis and Management. Eur Urol 2009;55:322-33.
- Schröder A, Abrams P, Andersson KE, Artibani W, Chapple CR, Drake MJ, et al.: Guidelines on Urinary Incontinence. In Aus G (ed.), Eau Guidelines. Arnheim, European Association of Urology. 2009; pp. 28-34.
- Trigo Rocha F, Gomes CM, Mitre AI, Arap S, Srougi M: A prospective study evaluating the efficacy of the artificial sphincter AMS 800 for the treatment of postradical prostatectomy urinary incontinence and the correlation between preoperative urodynamic and surgical outcomes. Urology. 2008; 71: 85-9.
- Herschorn S TJ, Bruschini H, et al.: Surgical treatment of urinary incontinence in men. In: Abrams P CL, Khoury S, Wein A (ed.), Incontinence: Third International Consultation. Paris, Health Publications Ltd. 2005; pp. 1241-96.
- Kumar A, Litt ER, Ballert KN, Nitti VW: Artificial urinary sphincter versus male sling for post-prostatectomy incontinence--what do patients choose? J Urol. 2009; 181: 1231-5.
- Romano SV, Metrebian SE, Vaz F, Muller V, D’Ancona CA, de Souza EA, et al.: Long-term results of a phase III multicentre trial of the adjustable male sling for treating urinary incontinence after prostatectomy: minimum 3 years. Actas Urol Esp. 2009; 33: 309-14.
- Sousa-Escandón A, Cabrera J, Mantovani F, Moretti M, Ioanidis E, Kondelidis N, et al.: Adjustable suburethral sling (male remeex system) in the treatment of male stress urinary incontinence: a multicentric European study. Eur Urol. 2007; 52: 1473-9.
- Giberti C, Gallo F, Schenone M, Cortese P: The bone-anchor sub-urethral sling for the treatment of iatrogenic male incontinence: subjective and objective assessment after 41 months of mean follow-up. World J Urol. 2008; 26: 173-8.
- Rehder P, Gozzi C: Transobturator sling suspension for male urinary incontinence including post-radical prostatectomy. Eur Urol. 2007; 52: 860-6.
Dr.
Ricarda M. Bauer
Urologische Klinik und Poliklinik
Ludwig-Maximilians-Universität München-Grosshadern
München, Germany
E-mail: Ricarda.Bauer@med.uni-muenchen.de