ALTERED
MALE PHYSIOLOGIC FUNCTION AFTER SURGERY FOR PROSTATE CANCER: COUPLE PERSPECTIVE
(
Download pdf )
doi: 10.1590/S1677-55382009000600008
MATVEY TSIVIAN, JANICE M. MAYES, TRACEY L. KRUPSKI, VLADIMIR MOURAVIEV, CRAIG F. DONATUCCI, THOMAS J. POLASCIK
Division of Urology, Department of Surgery and the Duke Prostate Center, Duke University Medical Center, Durham, North Carolina, USA
ABSTRACT
Purpose:
Both the diagnosis of prostate cancer (PCa) and the physiologic outcomes
of surgical treatment impact the male’s psychological sphere. However,
current research advocates a refocusing of outcomes directed to the PCa
“couple”. Herein we acquire insight into perspective and concordance
regarding male physiological function from the standpoint of a couple
recovering from PCa surgery.
Materials and Methods: Couples whereby the
male partner had undergone primary surgical treatment for PCa were mailed
a Retrospective Sexual Survey (RSS) packet consisting of male and female
partner questionnaires. RSS questions surveyed physiological changes in
libido, foreplay, erection and arousal, orgasm and ejaculation in addition
to perceived psychological impact. Patients’ and partners’
scores were evaluated to determine the concordance of both individual
items as well as domain sums.
Results: Twenty-eight couples completed
the questionnaires. Only about 40% of men and women were happy with their
levels of sexual interest with 82% concordance. Urine loss during orgasm
was reported by 43% of men; the majority of participants were bothered
by it. Ejaculation changes were observed by 96% of men (concordance 96%)
with most reporting anejaculation. A change in orgasm experience was noted
by 86% of men (and 36% of their female partners, p < 0.0001). Despite
the change, the majority of men and women reported being satisfied with
their ability to climax.
Conclusion: Our results indicate that patients
and their female partners may interpret differently the same physiological
outcomes of PCa surgery. This information could be useful to better counsel
the PCa couple and help patients and partners adjust after surgery.
Key
words: prostatic neoplasms; prostatectomy; sexual dysfunction,
physiological; couples therapy
Int Braz J Urol. 2009; 35: 673-82
INTRODUCTION
Prostate
cancer (PCa) is the second most lethal cancer for adult men in the United
States (1). Many of the patients diagnosed with PCa choose to undergo
surgical treatment. The anxiety of cancer diagnosis coupled with the side
effect profile associated with surgical treatment impact the male’s
psychological state (2,3). Prostate cancer surgery will result in variable
degrees of impaired urinary control and sexual dysfunction. Research suggests
that not only is the patient affected by these events but also the partner
(4,5). When men are in a stable relationship, the couple’s perspective
becomes an important issue and necessitates a refocusing of outcomes directed
to the prostate cancer “couple” (5). Although sexual dysfunction
has been shown to be related to psychological impairment in males (2),
this aspect has not been yet addressed from a couple perspective.
In this study we acquired insight into the couples’ perspective
and concordance regarding the physiological male function from a psychological
view of the couple recovering from primary surgical treatment for PCa.
MATERIALS AND METHODS
A
total of 246 couples whereby the male partner had previously undergone
primary surgical treatment for PCa at the Duke University Medical Center
by a single surgeon (TJP) between 2002 and 2007 were mailed a Retrospective
Sexual Survey (RSS) packet consisting of a specific Institutional Review
Board approved informed consent form and male and female questionnaires.
Only heterosexual couples being together before and after treatment were
enrolled. Male partners received a patient RSS and International Index
of Erectile Function (IIEF); female partners received a partner RSS and
Female Sexual Function Index (FSFI). The IIEF and FSFI are validated instruments
(6,7), while patient and partner RSS are a series of hypotheses generating
questions. The RSS consists of 47 items, most assessed in a binary fashion
or on a 1 to 5 Likert scale (Appendix 1 and 2 - see on-line Journal http://www.brazjurol.com.br/november_december_2009/Tsivian_673_682_appendix.pdf
for details). In this study we focused on RSS questions that surveyed
physiological changes in libido, foreplay, erection and arousal, orgasm
and ejaculation in addition to psychological burden of postoperative changes
on both the patient and his partner.
RSS, IIEF and FSFI scores were recorded.
IIEF scores based on a 15-item questionnaire were additionally recalculated
to fit a shorter 5-question version, the IIEF-5 (8) which is more familiar
to clinicians. RSS responses were compared between patients and partners
using Chi-squared or Fisher’s exact test as appropriate. Descriptive
statistics were generated. Patients’ and partners’ scores
were evaluated in a paired manner to determine the concordance in different
RSS questionnaire items and domains to more specifically address couple
perspective. Concordance was computed based on each couple responses on
each single item. Whenever both the patient and his partner gave the same
response it was considered concordant on the particular item. For items
graded on a Likert scale, deviation of ± 1 grade was deemed concordant.
In calculating concordance rates we excluded couples whenever one of the
members did not respond. For Likert scale items, distributions were analyzed
and average scores computed. Statistical analysis was performed using
SAS software v9 (SAS Institute Inc., Cary, NC). The study was Institutional
Review Board approved.
RESULTS
A
total of 28 couples completed the questionnaires (response rate of 11.4%)
and were enrolled in this study. The patients surveyed were treated between
2002 and 2007 with an average mean follow-up of 28 months after surgery.
Patients’ median age was 62 years (range 48-75); 82% were Caucasians,
14% African Americans and 4% Native Americans.
Surgical interventions were distributed as follows: 18% cryoablation (20%
nerve sparing), 21% robotic radical prostatectomy (0% nerve sparing) and
61% retropubic radical prostatectomy (71% nerve sparing). Male patients
had a median IIEF score of 52.5 (range 5-74), corresponding to a shortened
IIEF-5 median score of 18 (5-25) after surgery. Of note 10 patients (42%)
scored 21 or more on the IIEF-5, indicating good erectile function in
our cohort of patients following surgical treatment. Detailed IIEF results
are reported in Table-1. A summary of the female partners’ FSFI
scores is reported in Table-2.
RSS questionnaires evaluated the physiological
domains of foreplay, libido, erection and arousal, ejaculation and orgasm;
detailed description of the results and the respective concordance rates
are reported in Table-3.
No statistically significant differences (p > 0.05) we recorded between
male patients and their female partners’ responses in libido and
foreplay domains. There was a > 80% concordance on use and helpfulness
of foreplay. While > 70% of pairs stated they utilized more or the
same foreplay after PCa treatment, the concordance was only 48%. In the
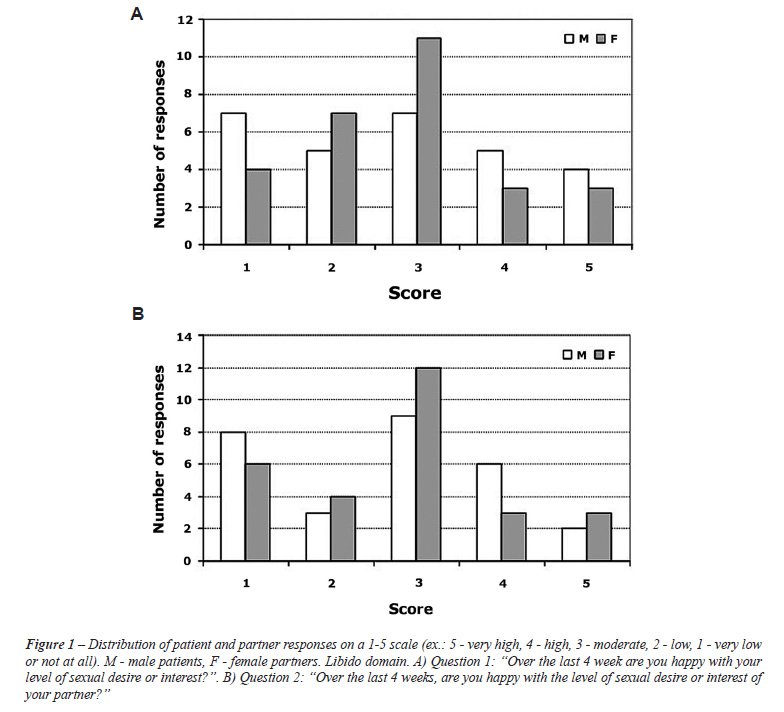
libido domain, only 43% of men and 39% of women reported being happy with
their level of sexual interest (82% concordance), although the average
score was identical (3.21) between patients and partners, response distribution
differed between the two sexes; among women “moderate” was
the most common response while among men the responses were widely distributed
between the different options (Figure-1 A). Out of all men and women,
< 40% declared being happy with their partner’s level of desire
with 86% concordance and similar distribution of responses (Figure-1 B)
with an average score of 3.32 and 3.29 for male and female responders,
respectively.
Although 43% of patients reported urine
loss during orgasm, only 32% of women noticed this (concordance 75%),
58% of men and 60% of their female partners reported being bothered by
it. More than one-half of patients and partners reported that the appearance
of the patient’s penis had changed (71% concordance), of those 29%
of men and 14% of women are bothered by the change.
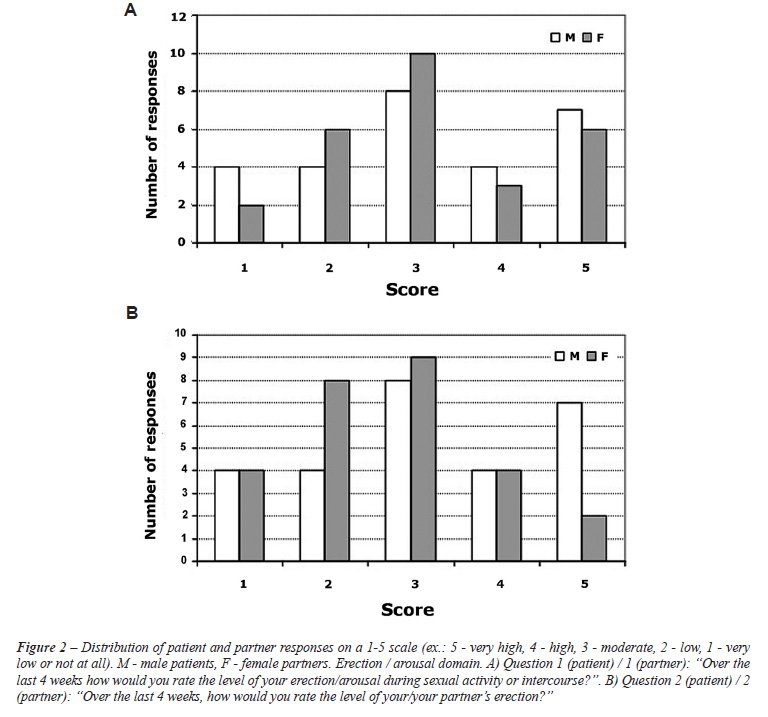
Regarding the erection/arousal domain, couples
reported a sensible drop in the number of times sex was initiated after
surgery: 50% of men and 39% of women replied 0-2 times in the last 4 weeks
(18% and 14% gave the same response when asked about this before surgery).
The concordance rates dropped from 93% on initiating sex before surgery
to 80% on the item after surgery. Response distribution regarding erection/arousal
levels was similar in patients and partners (Figure 2 A and B). Interestingly,
68% of men considered themselves at least partially potent (and so did
61% of women), but the concordance rate was only 59%. Of note, 32% of
men reported using medications to improve erections, compared to 85% of
women who stated their partner had used medications (p < 0.0001). On
this question, a 50% concordance rate was registered.
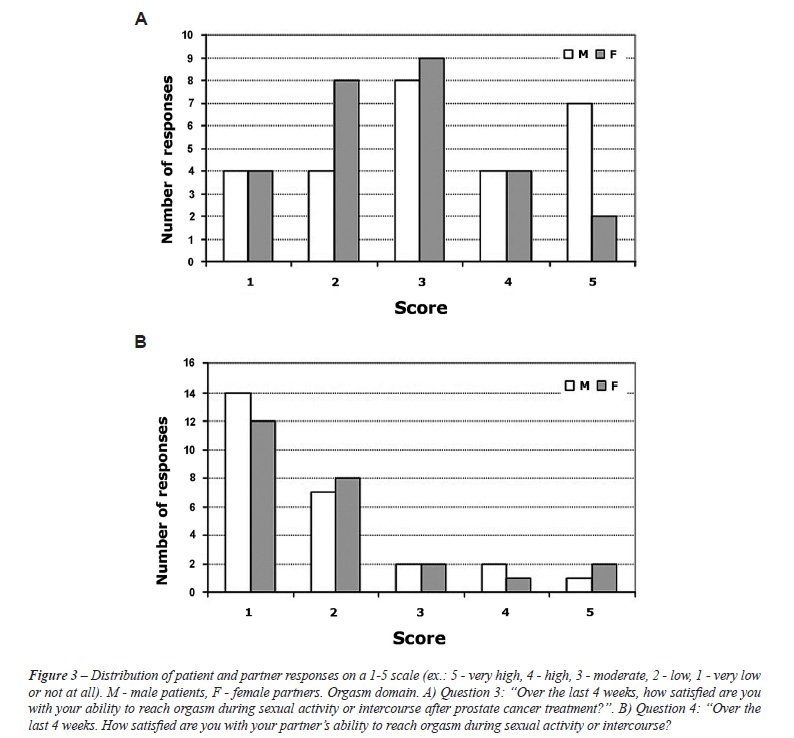
In the orgasm domain, the majority of men
reported a change in their experience of orgasm, compared to 36% of their
partners, p < 0.0001 (concordance 36%). When asked how it changed,
33% of men attributed the change to no ejaculation, 17% said the orgasm
was difficult to reach, and 17% reported the orgasm as less intense. When
asked about their partner’s experience of orgasm, the figures inverted
with significantly more men believing that their partner’s experience
of orgasm had not changed while their partners believed that the patient’s
experience had changed, p < 0.0001 (Figure 3 A and B). Despite the
change, the majority of men and women reported being satisfied with their
ability to reach orgasm. When asked about their partners, the figures
were similar (p = 1). A change in ejaculation was observed by 96% men
and 89% of women (96% concordance) with most men reporting no ejaculation.
However, only 19% of men and 12% of women were bothered by this.
COMMENTS
Recent
research has shown that PCa diagnosis and treatment affects the psychology
of both partners in the couple (5,9). In the case of PCa treatment, erectile
dysfunction has to be specifically addressed as it represents a common
treatment-related outcome. It is agreed that sexual dysfunction impacts
male psychology and quality of life (2,10) but the effects on the couple
are largely unknown. To the best of our knowledge, this is the first study
focusing specifically on couple perspective on sexual function and its
psychological impact after surgery for PCa.
Our cohort of patients had variable degrees of erectile dysfunction after
PCa surgical therapy when evaluated with the IIEF. More than one-half
of the men had some degree of dysfunction reflected in IIEF-5 scores of
less than 20 (11). Similarly, among the female partners, the majority
may have female sexual dysfunction using a proposed FSFI cutoff value
of 26.55 (12). These data suggest that sexual dysfunction following surgery
for PCa impacts both members of the couple, and in the female partner
the dysfunction is most likely due to a psychological rather than physical
impact since only their male partner had undergone surgery. It has been
shown that female partners of men with PCa are more distressed and have
higher depression scores (5,10). This psychological stress may be reflected
in sexual function of those women. It has been previously demonstrated
that the partner’s distress and the difference in distress between
partners impact the quality of life (4), and we suggest that in part this
is due to a negative effect on the sexual sphere.
We could appraise that physiological items such as “has the nature
of ejaculation changed following surgery?” or “how many times
on average was sex initiated?” had higher concordance rates than
questions regarding the psychological burden or speculation, as for instance
“if yes, does this bother?” or “has your partner’s
experience changed?”. These results further underline the disparities
between male and female psychology; such differences may be more evident
in stressful situations such as in our setting of couples adjusting to
PCa and its treatment effects. These results support the conclusions of
several studies that emphasized the disparities in psychological perceptions
of PCa couples (4,5,9).
This study highlights several important
points. There is solid concordance among couples that foreplay is helpful
after PCa treatment. It was also concordant among men and women that 50%
suffer from low libido, some of which creates low satisfaction with the
partner’s libido. It was noted that the initiation of sex declined
after surgery. Perhaps this latter observation can in part be explained
by the decline in perceived libido. On these items, no significant differences
were found in the responses between patients and their partners.
Regarding alterations in physiologic function after PCa treatment, over
one-half noticed a change in the appearance of the penis. However, this
bothered twice as many men as the female partners; nevertheless, statistical
significance could not be reached on this item, probably due to small
sample size. Men tended to consider themselves more potent than their
female partner’s perception. Additionally men believe they relied
less on requiring medical assistance to achieve an erection than their
female partners thought.
Regarding orgasm, most men felt that their
experience had changed after PCa treatment with 96% concordance for anejaculation.
The lack of ejaculation after radical prostatectomy is an expected outcome
and most couples were not bothered to experience it. Overall, 75% of men
were satisfied with their ability to climax despite altered physiological
function associated with surgery.
Of interest, nearly one-half of men reported urine loss during orgasm
while the majority of female partners were not aware of this. This frequent
effect of surgical treatment bothered more than two-thirds of the couples
experiencing it. A recent study (13) reported a series of patients suffering
from urine loss during orgasm, however the prevalence of this phenomenon
was not assessed. Based on their study of patients who lose urine during
orgasm, one-half considered this to be a “big social problem”.
These results are in line with our study, underlining the importance of
an increased awareness of this problem as it may impact significantly
the quality of life of both the patient and his partner. The incidence
of ejaculatory urinary incontinence after radical prostatectomy in the
literature ranges from 20% to 93% (14-17) but remains surprisingly underreported
and its burden underestimated. In our study we found that near 50% of
the patients report losing urine during orgasm and the majority of both
patients and their partners are bothered by this phenomenon.
Our survey results may help to better counsel
the prostate cancer couple and aid in adjustment to outcomes of PCa surgery.
Several studies support the need for such an intervention (4,5,9). The
RSS may act as a useful basis for construction and validation of a new
instrument that would assess sexual aspects of the PCa couple as well
as the related psychological impact of the treatment. Thus, healthcare
providers would be able to precisely target psychological interventions
that may aid the couple in adjusting to PCa and in coping with the related
stress.
Our study is not void of limitations and
its results should be evaluated accordingly. First, a low response rate
and consequently a small cohort evaluated at different time points after
surgery limit the strength of the conclusions since it is difficult to
predict the impact of those who did not participate. Second, our study
had only a limited means of comparison between before and after surgery,
although some questions were structured specifically to review the changes
following treatment. An additional limitation is the fact that the RSS
is not a validated tool, however we supported it in this preliminary study
with validated and widely accepted sexual function assessment tools such
as the IIEF and FSFI.
CONCLUSION
In this study, we gained an insight on the intimate sphere of the couple adjusting to PCa treatment outcomes. We were able to highlight several differences in the partners’ perspective related to sexual function. This information could be useful for healthcare providers to better counsel the prostate cancer couple and help patients and partners adjust to their condition.
ACKNOWLEDGMENT
Mary
Duke Biddle and the Trent Foundations provided funding for this research.
CONFLICT OF INTEREST
None declared.
REFERENCES
- American Cancer Society. Cancer Facts and Figures 2008. [pdf] Atlanta: American Cancer Society; 2008 [cited 2008 12/11/08]; Available from: http://www.cancer.org/downloads/STT/2008CAFFfinalsecured.pdf.
- Latini DM, Penson DF, Wallace KL, Lubeck DP, Lue TF: Clinical and psychosocial characteristics of men with erectile dysfunction: baseline data from ExCEED. J Sex Med. 2006; 3: 1059-67.
- Lehto US, Ojanen M, Väkevä A, Aromaa A, Kellokumpu-Lehtinen P: Noncancer life stresses in newly diagnosed cancer.Support Care Cancer. 2008; 16: 1231-41.
- Kim Y, Kashy DA, Wellisch DK, Spillers RL, Kaw CK, Smith TG: Quality of life of couples dealing with cancer: dyadic and individual adjustment among breast and prostate cancer survivors and their spousal caregivers. Ann Behav Med. 2008; 35: 230-8.
- Soloway CT, Soloway MS, Kim SS, Kava BR: Sexual, psychological and dyadic qualities of the prostate cancer ‘couple’. BJU Int. 2005; 95: 780-5.
- Rosen RC, Riley A, Wagner G, Osterloh IH, Kirkpatrick J, Mishra A: The international index of erectile function (IIEF): a multidimensional scale for assessment of erectile dysfunction. Urology. 1997; 49: 822-30.
- Rosen R, Brown C, Heiman J, Leiblum S, Meston C, Shabsigh R, et al.: The Female Sexual Function Index (FSFI): a multidimensional self-report instrument for the assessment of female sexual function. J Sex Marital Ther. 2000; 26: 191-208.
- Rosen RC, Cappelleri JC, Smith MD, Lipsky J, Peña BM: Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int J Impot Res. 1999; 11: 319-26.
- Cliff AM, MacDonagh RP: Psychosocial morbidity in prostate cancer: II. A comparison of patients and partners. BJU Int. 2000; 86: 834-9.
- Crowe H, Costello AJ: Prostate cancer: perspectives on quality of life and impact of treatment on patients and their partners. Urol Nurs. 2003; 23: 279-85.
- Schroeck FR, Donatucci CF, Smathers EC, Sun L, Albala DM, Polascik TJ, et al.: Defining potency: a comparison of the International Index of Erectile Function short version and the Expanded Prostate Cancer Index Composite. Cancer. 2008; 113: 2687-94.
- Wiegel M, Meston C, Rosen R: The female sexual function index (FSFI): cross-validation and development of clinical cutoff scores. J Sex Marital Ther. 2005; 31: 1-20.
- Abouassaly R, Lane BR, Lakin MM, Klein EA, Gill IS: Ejaculatory urine incontinence after radical prostatectomy. Urology. 2006; 68: 1248-52.
- Choi JM, Nelson CJ, Stasi J, Mulhall JP: Orgasm associated incontinence (climacturia) following radical pelvic surgery: rates of occurrence and predictors. J Urol. 2007; 177: 2223-6.
- Barnas JL, Pierpaoli S, Ladd P, Valenzuela R, Aviv N, Parker M, et al.: The prevalence and nature of orgasmic dysfunction after radical prostatectomy. BJU Int. 2004; 94: 603-5.
- Lee J, Hersey K, Lee CT, Fleshner N: Climacturia following radical prostatectomy: prevalence and risk factors. J Urol. 2006; 176: 2562-5; discussion 2565.
- Koeman M, van Driel MF, Schultz WC, Mensink HJ: Orgasm after radical prostatectomy. Br J Urol. 1996; 77: 861-4.
____________________
Accepted after revision:
June 29, 2009
_______________________
Correspondence address:
Dr. Matvey Tsivian
Postdoctoral Associate
Duke University Medical Center
DUMC 2804, Yellow Zone
Durham, NC 27710, USA
Fax: + 1 919 684-5220
E-mail: matvey.tsivian@duke.edu