HEMATURIA
IN A PATIENT WITH PERSISTENT LEFT CARDINAL VEIN CROSSING RETROAORTIC TO
THE RIGHT CARDINAL VEIN (INFERIOR VENA CAVA)
(
Download pdf )
ERICH K. LANG, QUAN D. NGUYEN
Department of Imaging (EKL), Johns Hopkins Medical Institutions, Baltimore, Maryland, USA and Department of Radiology (EKL, QDN), SUNY Downstate Medical School, Brooklyn, New York, USA
Radiology Page
Vol. 36 (6):
759-760, November - December, 2010
doi: 10.1590/S1677-55382010000600015
This
52-year-old Caucasian male presented with microscopic hematuria and bouts
of gross hematuria increasing in frequency. Four prior urologic work-ups,
consisting of cystoscopy, IVUs, ultrasound examinations, urinalysis performed
during the last 15 years had failed to identify a cause for the hematuria.
At admission, a well nourished male, with
essentially normal laboratory findings, Hb 14.8 gm, Hct 41, RBC 5.1 mil,
WBC 5800, BUN 18 mg/dl, potassium 4.6 mEq/L, creatinine 0.9 mg/dl, glucose
92 mg/dl, alk ptas 108 U/l, however, showed abnormal urinanalysis 8-10
RBC / hpf, 1-2 WBC / hpf, spec grav 1014.
Physical examination revealed mild edema of the lower extremities, and
minimal venous distension of both right and left dorsal pedal veins. Otherwise,
no abnormalities were noted. Once again cystoscopy was unremarkable.
A contrast enhanced multi-detector computed
tomography discovered major abnormalities of the inferior vena cava (IVC)
and renal veins.
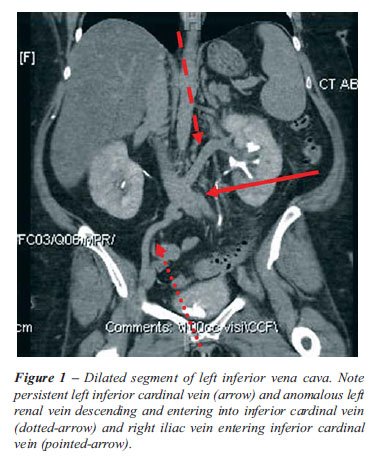
The right and left common iliac vein joined to form a left inferior vena
cava, (persistent left cardinal vein) and ascended to the left of the
aorta (Figure-1). The left renal vein descended steeply and then emptied
into the left IVC. The left IVC then crossed under the aorta to continue
on the right side after receiving flow from the right renal vein (1).
The left IVC prior to its passage under the aorta appears to be distended
(Figure-2).

Left retroaortic renal vein and compression
of the left renal vein in its passage between superior mesenteric artery
and aorta are a well recognized cause for hematuria (2), resultant increased
pressure in the left renal vein causes bleeding. The compression of the
left inferior cardinal vein at its passage under the aorta similarly increased
pressure, which because of the location of the left renal vein in our
patient was transmitted to the left renal vein (1,2). The striking dilatation
of the left cardinal vein attests to the hemodynamic significance.
REFERENCES
- Natsis K, Apostolidis S, Noussios G, Papathanasiou E, Kyriazidou A, Vyzas V: Duplication of the inferior vena cava: anatomy, embryology and classification proposal. Anat Sci Int. 2010; 85: 56-60.
- Gupta A, Naik N, Gulati GS: Mesoaortic entrapment of a left inferior vena cava. Indian J Radiol Imaging. 2010; 20: 63-5.
_______________________
Correspondence
address:
Dr. Erich K. Lang
Department of Radiology
SUNY Downstate College of Medicine
450 Clarkson Avenue
Box 1198, Brooklyn, NY, 11231, USA
Fax: + 1 718-270-3848
E-mail: erich.lang@downstate.edu