Validation of the Brazilian version of the Expanded Prostate Cancer Index Composite (EPIC) for patients submitted to radical prostatectomy
(Download pdf)
doi: 10.1590/S1677-5538.IBJU.2013.06.12
Suelen Costa, João P. M. Carvalho, Waldemar S. Costa, Luiz E. M. Cardoso, Francisco J. B. Sampaio, Luciano Alves Favorito
Urogenital Research Unit of Rio de Janeiro State University, RJ, Brazil
Original Article
Vol. 39 (6): 853-860, November - December, 2013
ABSTRACT
Purpose: The objective of this paper is to analyze the structure of the ureter in normal and anencephalic human fetuses.
Materials and Methods: We studied 16 ureters from 8 human fetuses without congenital anomalies aged 16 to 27 weeks post-conception (WPC) and 14 ureters from 7 anencephalic fetuses aged 19 to 33 WPC. The ureters were dissected and embedded in paraffin, from which 5 µm thick sections were obtained and stained with Masson trichrome, to quantify smooth muscle cells (SMC) and to determine the ureteral lumen area, thickness and ureteral diameter. The samples were also stained with Weigert Resorcin Fucsin (to study elastic fibers) and Picro-Sirius Red with polarization and immunohistochemistry analysis of the collagen type III fibers to study collagen. Stereological analysis of collagen, elastic system fibers and SMC were performed on the sections. Data were expressed as volumetric density (Vv-%). The images were captured with an Olympus BX51 microscope and Olympus DP70 camera. The stereological analysis was done using the Image Pro and Image J programs. For biochemical analysis, samples were fixed in acetone, and collagen concentrations were expressed as micrograms of hydroxyproline per mg of dry tissue. Means were statistically compared using the unpaired t-test (p < 0.05).
Results: The ureteral epithelium was well preserved in the anencephalic and control groups. We did not observe differences in the transitional epithelium in the anencephalic and control groups. There was no difference in elastic fibers and total collagen distribution in normal and anencephalic fetuses. SMC concentration did not differ significantly (p = 0.1215) in the anencephalic and control group. The ureteral lumen area (p = 0.0047), diameter (p = 0.0024) and thickness (p = 0.0144) were significantly smaller in anencephalic fetuses.
Conclusions: Fetuses with anencephaly showed smaller diameter, area and thickness. These differences could indicate that anencephalic fetal ureters tend to have significant structural alterations, probably due to cerebral lesions with consequent brain control damage of ureter nerves.
Key words: Anencephaly; Ureter; Embryology; Humans
INTRODUCTION
Neural tube defects are one of the most common congenital malformations of the central nervous system, with an average prevalence at birth of 1 per 1000 (1). Anencephaly is the most severe fetal neural tube defect, resulting from failure of the neural tube to close at the base of the skull in the third or fourth week (day 26 to 28) after conception, leaving the skull bones that usually surround the head unformed.
Despite ethical conflicts, the literature shows some reports about the use of anencephalic fetus organs for transplantation (2-5). The organ structure of anencephalic fetuses and children is virtually unknown. Recently the structure of anencephalic fetal kidneys (6), bladder (7) and penis (8) has been studied. The bladder of anencephalic fetuses had gross histological alterations when compared to normal fetuses (7). Carvalho (8) showed no differences in the structure of the genitalia from anencephalic fetuses compared to normal ones.
In the future, ureter tissue from anencephalic fetuses could be used as engineering models in the pediatric population (9). Tissue from kidneys, ureters and bladder could also be used in the future as an alternative to complex reconstructive surgeries (10).
There are few reports of the morphology of ureters during the human fetal period (11), and there are no studies of the ureter in anencephalic fetuses. The objective of our study is to analyze the ureter structure in anencephalic human fetuses.
MATHERIALS AND METHODS
The present work received approval from the institutional review committee and parents. This work was carried out in accordance to the ethical standards of the institutional committee on human experimentation.
We studied 16 ureters obtained from 8 human fetuses (4 males and 4 females) and 14 ureters from 7 anencephalic human fetuses (4 males and 3 females) that died of causes unrelated to the genitourinary tract. The fetuses were macroscopically well preserved and there was no evidence of congenital malformation. The gestational age of the fetuses was determined in weeks post-conception (WPC), according to the foot-length criterion. This criterion is currently considered the most acceptable parameter to calculate gestational age (12-16). The fetuses were also evaluated regarding crown-rump length and body weight immediately before dissection. All measurements were made by the same observer.
After the measurements, the fetuses were carefully dissected with the aid of a stereoscopic lens with 16/25X magnification. The fetal ureter was carefully removed, together with kidneys and bladder. The ureter was separated from the other structures and the distal portion was fixed in 10% buffered formalin, and routinely processed for paraffin embedding, and 5 µm thick sections were obtained at 200 µm intervals. Smooth muscle cells, connective tissue, elastic system fibers and collagen were studied by histochemical, immunohistochemical and biochemical methods.
Sections were stained with hematoxylin-eosin to assess the integrity of the tissue. We performed the following staining: Masson’s trichrome, in order to quantify SMC and to determine the ureteral lumen area, thickness and ureteral diameter; Weigert Resorcin Fucsin with previous oxidation in order to observe elastic system fibers; and Picro-Sirius Red with polarization for observation of different collagen types. SMC were quantified by the stereological method (17).
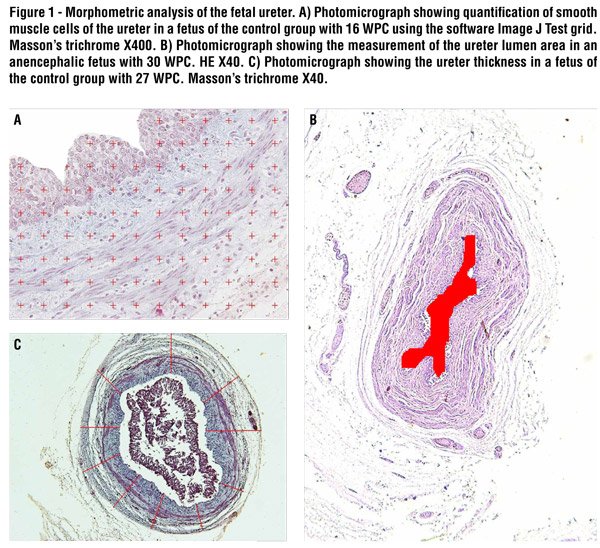
Five sections were stained, and five fields of each section were selected. All selected fields were photographed with an Olympus DP70 camera coupled to an Olympus BX51 microscope. The images were processed using the Image Pro software. The fibers were quantified using the Image J software to determine the volumetric density (Vv) of each component (Figure-1A). The ureter lumen area was determined by the contour of the epithelium (Figure-1B) and the ureter thickness was measured using the program at least five times for each specimen (Figure-1C).
The immunohistochemical analysis of the collagen type III (mouse monoclonal collagen III ABCAM) and collagen type I (mouse monoclonal collagen I ABCAM) fibers used the avidin biotin (ABC) method with positive and negative controls. The immunohistochemical analysis of the elastic system fibers used the Monoclonal Elastin Antibody ab 9519 (Abcam®, Cambridge, MA, United States). The slides were previously treated with poly-L-lysine for better adherence of the sections.
For the biochemical analysis of the collagen, tissue samples were fixed in acetone. The concentration of total collagen in the bladder tissue was determined by a colorimetric hydroxyproline assay. Thus, 5 to 14 mg of dry, defatted ureter tissue was hydrolyzed in 6N HCl for 18 hours at 118 ºC, as previously described (19). The assay was then carried out in the neutralized hydrolysates using the chloramine T method (20). The results were expressed as micrograms of hydroxyproline per milligram of dry, defatted tissue.
Means were statistically compared using the unpaired t-test (p < 0.05) and the Wilcoxon two-sample test with the Graph Pad Prism software.
RESULTS
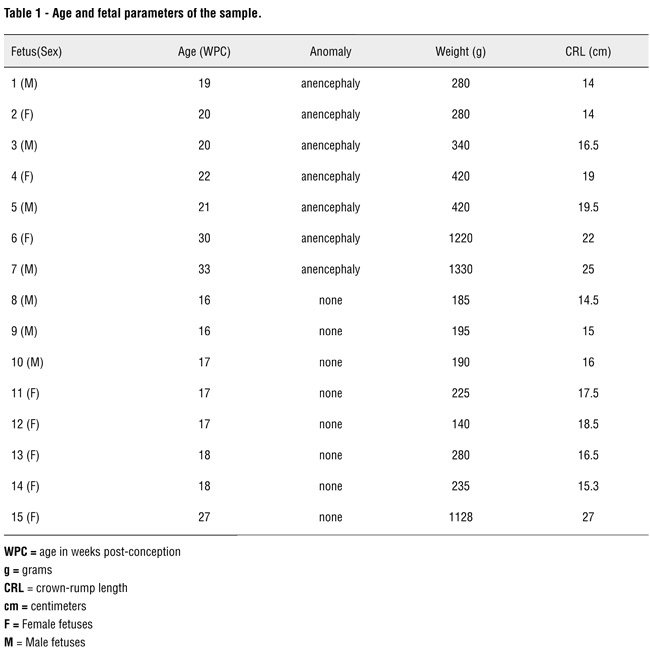
After dissection, we did not observe any macroscopic anomalies in the urogenital system of the anencephalic fetuses. These fetuses ranged in age between 19 and 33 WPC, weighed between 280 and 1330 g, and had crown-rump length between 14 and 25 cm. The fetuses of the control group ranged in age between 16 and 27 WPC, weighed between 185 and 1128 g, and had crown-rump length between 14.5 and 27 cm (Table-1).
The ureteral epithelium was well preserved in the anencephalic and control groups. We did not observe differences in the transitional epithelium in the anencephalic and control groups. The analysis of the ureteral lumen area showed a decrease (p = 0.0047) in anencephalic ureter (6365 ± 1282 µ) compared to the control group (20170 ± 5480 µ). The ureteral diameter was smaller (p = 0.0024) in the anencephalic ureters (166.7 ± 10.99 µ) than in those in the control group (240.0 ± 26.66 µ) and ureteral thickness were also significantly smaller (p = 0.0144) in the anencephalic fetuses (30.57 ± 2.034 µ) as compared to the normal fetuses (47.49 ± 7.453 µ). The statistical data are presented in Table-2.
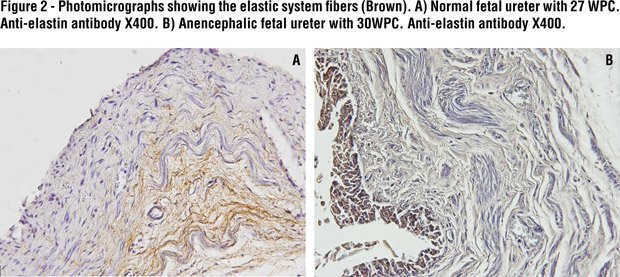
Histochemistry with Weigert’s showed unclear results, so to confirm the presence of elastic system elements, we performed immunolabeling with elastin, which showed positivity only in fetuses from 27th WPC. There was no difference in elastic fiber distribution in the normal and anencephalic fetuses (Figure-2).
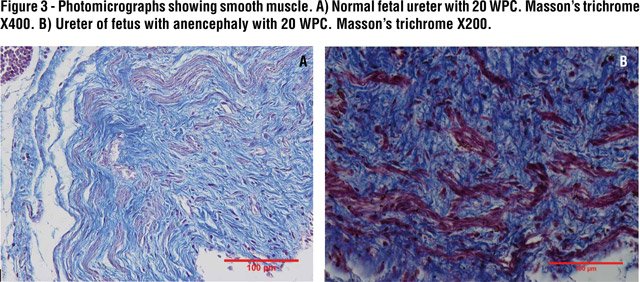
Stereology analysis documented a decrease without significance (p = 0.1215) of SMC in anencephalic ureters (12.00 ± 1.628%) compared to normal organs (13.51 ± 0.9231%). Figure-3 shows the SMC arrangement in normal and anencephalic fetus ureters.
Biochemical analysis showed that the concentrations of total collagen in the ureter from normal (mean ± SD, 38.19 ± 16.86 μg hydroxyproline/mg dry tissue) and anencephalic (44.26 ± 7.13 μg hydroxyproline/mg dry tissue) fetuses were not significantly different (p > 0.05).
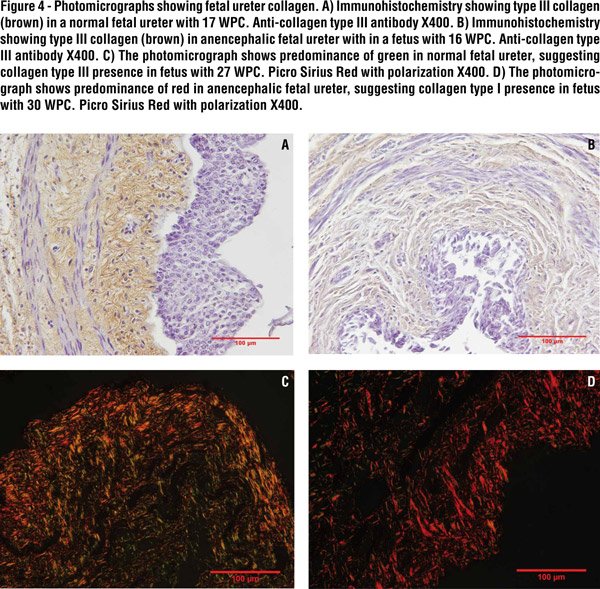
In the qualitative analysis by Immunohistochemistry, type III collagen was observed in both groups, although normal fetus ureters showed a higher quantity (Figure-4A and Figure-4B). Regarding type I collagen, only a small quantity was observed in both groups. Picro Sirius Red with polarization photomicrographs presented a difference in colors between the groups. This difference could suggest changes in the collagen fiber organization of anencephalic fetal ureters. The analysis showed predominance of green in normal fetal ureters, suggesting collagen type III presence and a predominance of red in anencephalic fetal ureters, suggesting collagen type I presence in this group (Figure-4C and Figure-4D).

DISCUSSION
The ureters develop from the caudal portion of the ureteric bud. At the fifth week of development, the ureteric bud arises as a diverticulum from the mesonephric (Wolfian) duct (21). The ureter bud grows cranially and contacts the intermediate mesoderm. As it reaches the mesoderm in the lower lumbar - upper sacral region, a cap of mesoderm cells surrounds it. This cap is called the metanephrogenic blastema. The metanephrogenic blastema forms glomeruli, proximal tubules and distal tubules (21). The ureteric bud divides and branches forming the renal pelvis, calyces, and collecting tubules, which will provide a conduit for urine drainage in the mature kidney. At nine weeks of development, the metanephros, which will become the mature kidney, starts to produce urine (21).
Knowledge of the structure of the ureter in anencephalic fetuses is of great importance, since there are reports of an anencephalic fetus transplant donor with chronic renal failure where the ureter was used to divert urine (22). Such engineered tissue can be useful in the future for ureteral reconstruction. There are some reports of autologous urothelial cell transplantation (23,24) and ureteral reconstruction using autologous tubular grafts in animal models with good results (25,26). Analysis of the ureteral structure in anencephalic fetuses could be important in future studies of tissue engineering.
In our sample we did not observe significant differences in SMC between the anencephalic and normal fetuses. A slight but not significant increase in SMC was observed in the normal fetuses, but there was a significant decrease of lumen area, thickness and diameter in the ureters from anencephalic fetuses. In a recent study, we observed gross histological alterations in the bladder of anencephalic fetuses (7). Lesions in the nervous system with consequent alteration in nerve regulation could be a plausible hypothesis to explain structural changes in the bladder and ureter in patients with neural tube defects.
Anencephalic fetuses have cerebral exposition, usually with spinal cord preservation. Bladder nerves in anencephalic fetuses could be modified due to cerebral lesions with consequent brain control damage in bladder nerves. This could lead to structural alterations in anencephalic fetal bladders and ureters too.
Collagen and elastin are important components of the ureter wall, which affect ureter contraction. Collagen provides tensile strength although over-accumulation may inhibit ureteral contractility and the conduction of electrical impulses through the wall. Elastin provides tissue elasticity and could help compliance (27).
Elastic system fiber alterations are involved in fibrotic tissue formation. However, in our samples we only observed the presence of elastic fibers in fetuses with more than 25 WPC and we did not observe differences in elastic system fibers in either the anencephalic or control group. This might indicate that this extracellular matrix component appears only in the third gestational trimester in the fetal ureter. Previous studies have described the elastic system fibers in other human fetal genitourinary organs (28).
In our study, we did not observe significant differences between elastic fibers and total collagen in normal and anencephalic ureters, although we did observe a small increase of type I collagen in anencephalic fetal ureters. In a previous study of anencephalic bladders we observed a predominance of type III collagen. Collagen increases in chronic bladder obstruction in human adults. The abnormally large amount of collagen found in obstructed bladders is also believed to decrease muscle contractility, in addition to affecting bladder compliance and subsequent high intra-vesicle pressure, which results in changes in ureteral contraction and leads to histological changes in the ureteral wall (27). Previous studies in rabbits have shown that ureteral obstruction causes progressive thickening of the lamina muscularis mucosae with a large increase in collagen, findings not confirmed by our study.
CONCLUSIONS
The concentrations of total collagen in the ureter from normal and anencephalic fetuses are not significantly different. Fetuses with anencephaly showed smaller diameter, area and thickness. These differences could indicate that anencephalic fetal ureters have significant structural alterations, probably due to cerebral lesions with consequent brain control damage in ureter nerves.
Abbreviations:
WPC = weeks post-conception
Vv = volumetric density
SMC = Smooth Muscle Cells
ACKNOWLEDGEMENTS
Supported by grants from the National Council for Scientific and Technological Development (CNPQ - Brazil) and Rio de Janeiro State Research Foundation (FAPERJ), Brazil
CONFLICT OF INTEREST
None declared.
REFERENCES
- Blatter BM, van der Star M, Roeleveld N: Review of neural tube defects: risk factors in parental occupation and the environment. Environ Health Perspect. 1994; 102: 140-5.
- Davis A: The status of anencephalic babies: should their bodies be used as donor banks? J Med Ethics. 1988; 14: 150-3.
- Salaman JR: Anencephalic organ donors. BMJ. 1989; 298: 622-3.
- [No authors listed]: Use of anencephalic newborns as organ donors. Paediatr Child Health. 2005; 10: 335-7.
- FIGO Committee for the Ethical Aspects of Human Reproduction and Women's Health: Anencephaly and organ transplantation. Int J Gynaecol Obstet. 2008; 102: 99.
- Kalaycioğlu A, Karaca M, Can I, Keleş ON, Uçüncü Y, Gündogdu C, et al.: Anencephalic fetuses can be an alternative for kidney transplantation: a stereological and histological investigation. Histol Histopathol. 2010; 25: 413-22.
- Pazos HM, Lobo ML, Costa WS, Sampaio FJ, Cardoso LE, Favorito LA: Do neural tube defects lead to structural alterations in the human bladder? Histol Histopathol. 2011; 26: 581-8.
- de Carvalho JP, Costa WS, Sampaio FJ, Favorito LA: Anencephaly does not cause structural alterations in the fetal penis. J Sex Med. 2012; 9: 735-42.
- Raya-Rivera A, Esquiliano DR, Yoo JJ, Lopez-Bayghen E, Soker S, Atala A: Tissue-engineered autologous urethras for patients who need reconstruction: an observational study. Lancet. 2011; 377: 1175-82.
- Zhao Z, Yu H, Xiao F, Wang X, Yang S, Li S: Differentiation of adipose-derived stem cells promotes regeneration of smooth muscle for ureteral tissue engineering. J Surg Res. 2012; 178: 55-62.
- Oswald J, Brenner E, Deibl M, Fritsch H, Bartsch G, Radmayr C: Longitudinal and thickness measurement of the normal distal and intravesical ureter in human fetuses. J Urol. 2003; 169: 1501-4.
- Mercer BM, Sklar S, Shariatmadar A, Gillieson MS, D'Alton ME: Fetal foot length as a predictor of gestational age. Am J Obstet Gynecol. 1987; 156: 350-5.
- Hern WM: Correlation of fetal age and measurements between 10 and 26 weeks of gestation. Obstet Gynecol. 1984; 63: 26-32.
- Platt LD, Medearis AL, DeVore GR, Horenstein JM, Carlson DE, Brar HS: Fetal foot length: relationship to menstrual age and fetal measurements in the second trimester. Obstet Gynecol. 1988; 71: 526-31.
- Costa WS, Sampaio FJ, Favorito LA, Cardoso LE: Testicular migration: remodeling of connective tissue and muscle cells in human gubernaculum testis. J Urol. 2002; 167: 2171-6.
- Favorito LA, Cardinot TM, Morais AR, Sampaio FJ: Urogenital anomalies in human male fetuses. Early Hum Dev. 2004; 79: 41-7.
- Cavalcanti AG, Costa WS, Baskin LS, McAninch JA, Sampaio FJ: A morphometric analysis of bulbar urethral strictures. BJU Int. 2007; 100: 397-402.
- Cabral CA, Sampaio FJ, Cardoso LE: Analysis of the modifications in the composition of bladder glycosaminoglycan and collagen as a consequence of changes in sex hormones associated with puberty or oophorectomy in female rats. J Urol. 2003; 170: 2512-6.
- Bergman I, Loxley R: Two improved and simplified methods for the spectrophotometric determination of hydroxyproline. Anal Biochem. 1963; 35: 1961-5.
- Moore KL, Persaud TVN: The developing human. Elsevier Science Health Science 7th ed. 2003.
- Laberge JM: Transplanting organs from anencephalic infants. CMAJ. 1987; 137:437-438.
- Xu Y, Fu W, Li G, Shi J, Tan H, Hu K, et al.: Autologous urothelial cells transplantation onto a prefabricated capsular stent for tissue engineered ureteralreconstruction. J Mater Sci Mater Med. 2012; 23: 1119-28.
- Geutjes P, Roelofs L, Hoogenkamp H, Walraven M, Kortmann B, de Gier R, et al.: Tissue engineered tubular construct for urinary diversion in a preclinical porcine model. J Urol. 2012; 188: 653-60.
- Zhang J, Gu GL, Liu GH, Jiang JT, Xia SJ, Sun J,et al.: Ureteral reconstruction using autologous tubular grafts for the management of ureteral strictures and defects: anexperimental study. Urol Int. 2012; 88: 60-5.
- Fu WJ, Xu YD, Wang ZX, Li G, Shi JG, Cui FZ, et al.: New ureteral scaffold constructed with composite poly(L-lactic acid)-collagen and urothelial cells by new centrifugal seeding system. J Biomed Mater Res A. 2012; 100: 1725-33.
- Kim KM, Kogan BA, Massad CA, Huang YC: Collagen and elastin in the normal fetal bladder. J Urol. 1991; 146: 524-7.
- Bastos AL, Silva EA, Silva Costa W, Sampaio FJ: The concentration of elastic fibres in the male urethra during human fetal development. BJU Int. 2004; 94: 620-3.
- Cheng EY, Maizels M, Chou P, Hartanto V, Shapiro E: Response of the newborn ureteropelvic junction complex to induced and later reversed partial ureteral obstruction in therabbit model. J Urol. 1993; 150: 782-9.
_____________________
Submitted for publication:
June 10, 2013
___________________
Accepted after revision:
July 24, 2013
______________________
Correspondence address:
Dr. Luciano Alves Favorito
Rua Professor Gabizo, 104 / 201
Tijuca, Rio de Janeiro, RJ, 20271-062, Brazil
Fax: + 55 21 3872-8802
E-mail: lufavorito@yahoo.com.br