HYDRONEPHROSIS
SECONDARY TO A SEMINOMA IN ABDOMINAL CRYPTORCHID TESTIS
(
Download pdf )
LUCIANO A. FAVORITO, DAIBES RACHID FILHO, CARLOS H. S. MANNES
Division of Urology, Souza Aguiar Municipal Hospital, Rio de Janeiro, RJ, Brazil
ABSTRACT
The incidence of testicular cancer in cryptorchidism is 30 to 50 times higher than in general population. We present a case of hydronephrosis caused by a seminoma in an abdominal cryptorchid testis. A 22 years old male presented abdominal and right flank pain, and haematuria. Despite the fact that he could not feel right testis since he was 7 years old, he had never looked for treatment. A huge mass was palpable in hypogastric, and IVP and CT Scan demonstrated functional exclusion of the right kidney, and a solid tumor localized at the right iliac fossa, near the bladder wall. The patient was submitted to laparotomy with resection of the mass, and the histopathologic study showed classic seminoma. Abdominal testes have higher incidence of malignancy than those in the inguinal position. The orchiopexy is recommended for abdominal testis after 2 years old to facilitate the investigation and identification of testicular cancer.
Key words:
testis; cryptorchidism; seminoma; hydronephrosis
Int Braz J Urol. 2002; 28: 437-8
INTRODUCTION
Cryptorchidism
is one of most frequent congenital pathologies, affecting from 2 to 5%
of boys. When testis is not found at the usual position, it suffers from
higher temperatures at the inguinal canal and within the abdomen. This
difference in temperature is harmful for germinatif epithelium, and would
also be responsible for malignant degeneration of the organ (1).
Non-palpable
testis responds for approximately 20% of cryptorchid testes. Only 20%
of non-palpable testes are absent, and the remainder are at abdominal
ou high inguinal position (1). Incidence of testicular cancer in cryptorchid
patients is estimated to be 30 to 50 times higher than in general population
(1). Intra-abdominal testes present a higher rate of neoplasia than testes
located at inguinal region.
This
case report aims to present a patient with abdominal cryptorchidism, that
developped a tumor and progressed with hydronephrosis resulting from ureteral
compression by the tumoral mass.
CASE REPORT
MSR,
male, 22 years old, presented pain in low abdominal region and right flank,
initiating 7 days before, colic-like, and severe. He also presented disuria,
haematuria, nausea and vomiting, besides weakness of urinary stream. He
reported absence of fever, bowel habit alterations or other complaints.
In history, the only relevant fact was the presence of right cryptorchidism,
not treated during childhood.
At
physical exam, in spite of the difficulties due to obesity, he presented
a hard and painful mass in hypogastric region, with approximately 8 cm;
rectal examination was normal, left testis was topic, without alterations,
and right testis was not found at scrotum. Dosing of serum tumor markers
was performed, showing increases in beta-HCG (750ng/mL) and in alpha-fetoprotein
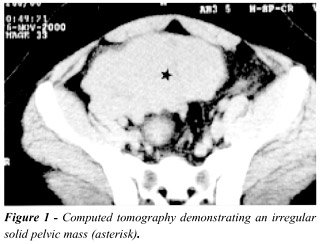
(30ng/mL). Intravenous pielogram demonstrated normal left kidney, and
functional exclusion of right kidney. Computed tomography showed huge
solid tumor, located in pelvis, with irregular contours (Figure-1), and
significant right hydronephrosis.
The
patient underwent an exploratory laparotomy with tumor exeresis. Histopathological
result was classic seminoma. Two weeks after mass excision, the patient
underwent right nephrectomy, after renal scan showing loss of right kidney
function. The patient was submitted to chemotherapy 30 days after the
nephrectomy. We have a 6 months follow-up of this patient, and he is in
good conditions, with no signs of tumoral recurrence.
DISCUSSION
Cryptorchid
testes ought to be treated until the second year of age; after this time,
injuries to the germinative epithelium may be irreversible. Neoplastic
alterations in cryptorchid testes occur independently of the moment this
pathology was corrected (1).
When
testis is located in abdomen and the diagnosis firmed during childhood,
orchiopexy is the technique of choice, and it may be done through autotransplantation,
or Fowler-Stephens surgery, in 1 or 2 steps; however the procedure of
choice is laparoscopic surgery (2). If the diagnosis is made in a more
advanced age, but the testis is viable, there are two options: preventive
excision of the organ, or its preservation at scrotum, what would permit
a better follow-up of its alterations (3). Some authors advocate testis
preservation, when it is viable.
Abdominal
cryptorchid testis present a higher incidence of neoplasia compared to
inguinal (1). Fixation of an abdominal cryptorchid testis, of normal size,
at scrotum after 2 years of age has as main purpose to facilitate its
monitoring (1).
Tumors
in abdominal testis are rare and lead to compression of urinary tract
only in case of huge masses (1). Preserving renal unit in this case would
happen if the diagnosis was done earlier. This case report reinforces
the importance of early diagnosis and treatment in pacients with non-palpable
testis.
REFERENCES
- Batata MA, Whitmore JR WF, Chu FCH, Hilaris BS, Loh J, Grabstald H et al.: Cryptorchidism and testicular cancer. J Urol. 1980; 124:382-7.
- Turek PJ, Ewalt DH, SnykerIII HM, Stampfers D, Blyth B, Huff DS et al.: The absent cryptorchid testis: Surgical findings and their implications for diagnosis and etiology. J Urol. 1994; 151:718-21.
- Rogers E, Teahan S, Gallagher H, Butler MR, Grainger R, Mcdermott ED et al.: The role of orchiectomy in the management of postpubertal cryptorchidism. J Urol. 1998; 159:851-4.
______________________
Received: March 21, 2002
Accepted after revision: October 9, 2002
_______________________
Correspondence address:
Dr. Luciano Alves Favorito
Rua Professor Gabizo 104 / 201
Rio de Janeiro, RJ, 20271-320, Brazil
Fax: + 55 21 3872-8802
E-mail: favorito@uerj.br