CYSTADENOMA
OF THE SEMINAL VESICLE
(
Download pdf )
ANTÔNIO O. GIL, LUCAS Y. S. YAMAKAMI, TÉRCIO GENZINI
Oswaldo Cruz Deutch Hospital, São Paulo, SP, Brazil
ABSTRACT
Primary
tumors of the seminal vesicle are extremely rare. Among them, there is
a spectrum of tumors derived from both epithelium and stroma and so classified
as epithelial-stromal tumors.
Herein, we report a case of a cystadenoma in a 49-year-old asymptomatic
man, detected in a routine ultrasonography for liver disease follow-up.
The digital rectal examination detected a large mass anterior to rectum
and posterior to bladder. Computed tomography scan and magnetic resonance
imaging showed a normal prostate and a 9.0 cm cystic tumor, replacing
the left seminal vesicle. The gross appearance and microscopic aspect
was compatible with cystadenoma of seminal vesicle. Patient’s postoperative
recovery was uneventful. He is currently alive, 3 years after the diagnosis,
with no signs of recurrence.
Key
words: seminal vesicle; neoplasms, glandular and epithelial;
cystadenoma
Int Braz J Urol. 2003; 29: 434-6
INTRODUCTION
Primary tumors of the seminal vesicle are extremely rare. Among them, there is a spectrum of tumors derived from both epithelium and stroma (1-3). Herein, we present a patient with an epithelial-stromal tumor in this unusual location.
CASE REPORT
A
49-year-old asymptomatic man with chronic hepatitis-C was at surveillance
after 1 year treatment with interferon, when a routine ultrasonography
demonstrated a pelvic mass. Physical examination was unremarkable except
for digital rectal examination, which detected a large mass anterior to
rectum and posterior to bladder, with a normal prostate. Computed tomography
(CT) scan and magnetic resonance imaging showed a normal prostate and
a 9 cm well-defined expansive tumor, predominantly cystic, with septations,
replacing the left seminal vesicle (Figure-1). No upper tract abnormalities
were seen.

The patient was explored through a midline
abdominal incision and a complex mass posterior to bladder was identified.
A direct approach to the retrovesical space was chosen, and the tumor
was totally dissected from attachments to the bladder anteriorly, rectum
posteriorly and surrounding tissues, and fully removed, without any incision
in bladder or rectum.
The tumor measured 7.0 x 5.0 x 4.5 cm. It
was covered by a gray capsule and there was a remanescent of the seminal
vesicle with 3.5 x 1.2 cm dimensions. Through the external surface, multiple
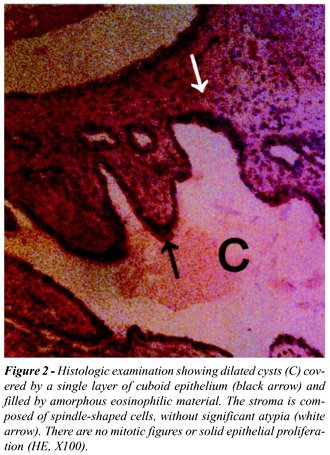
cavities were seen, fulfilled with a clear liquid. Histologic examination
showed dilated cysts, covered by a single layer of cuboidal epithelium,
without atypia (Figure-2). Microscopic aspect was compatible with cystadenoma
of the seminal vesicle.
The patient postoperative recovery was uneventful.
One year after surgery, a CT scan showed no signs of recurrence. He is
currently alive and well, 3 years after the diagnosis.
DISCUSSION
We
reported here a rare case of a cystadenoma of the seminal vesicle. Usually,
these benign tumors have only minor complaints, such as nonspecific lower
abdominal pain or urinary frequency (1-3). Diagnosis should be considered
in the presence of a mass located superior to prostate and posterior to
bladder, protruding the rectal wall (1, 3).
Macroscopically, they are multilocular tumors.
Microscopically, they have epithelial and stromal components combined.
The first delimits cystic areas, lined by a single layer of cuboidal or
columnar epithelium (3). The second is formed by fibrous connective tissue,
which may resemble fibroblasts or smooth muscle cells (3).
Differential diagnosis is made with expansive
injuries of retrovesical space such as carcinomas and cystic tumors. Immunohistochemical
analysis using prostate specific antigen and prostatic acid phosphatase
may be done to exclude prostatic origin (1-3). In the present case, macroscopic
and microscopic appearance was typical of a primary benign epithelial-stromal
tumor of the seminal vesicle and so, more properly called cystadenoma
(3).
There is not large experience on management
of these neoplasms. Marsupialization and aspiration are not indicated
due to their multilocular organization. Because fine needle aspiration
biopsies may be inconclusive (1,2), an exploratory laparotomy is usually
needed and, in this case, it is logical to remove the whole tumor and
involved seminal vesicle. When surgical treatment is successful, prognosis
is invariably good, without recurrence.
REFERENCES
- Mazzucchelli L, Studer UE, Zimmermann A: Cystadenoma of the seminal vesicle: case report and literature review. J Urol. 1992; 147: 1621-4.
- Baschinsky DY, Niemann TH, Maximo CB, Bahnson RR: Seminal vesicle cytadenoma: a case report and literature review. Urology 1998; 51: 840-5.
- Santos LD, Wong CSKC, Killingsworth M: Cystadenoma of the seminal vesicle: report of a case with ultrastructural findings. Pathology 2001; 33: 399-402.
____________________
Received: April 25, 2003
Accepted after revision: June 27, 2003
_______________________
Correspondence
address:
Dr. Antônio Otero Gil
Rua Cotoxó, 611 / 10º andar / 105
São Paulo, SP, 05021-000, Brazil
Fax: + 55 11 3873-5782
E-mail: doctorgil@uol.com.br