SOLITARY
FIBROUS TUMOR IN BLADDER WALL
(
Download pdf )
KÁTIA R. M. LEITE, MIGUEL SROUGI, ARI MIOTTO, LUIZ H. CAMARA-LOPES
Laboratory
of Surgical and Molecular Pathology, Syrian Lebanese Hospital, and
Discipline of Urology, Paulista School of Medicine, Federal University
of São Paulo (UNIFESP), São Paulo, SP, Brazil
ABSTRACT
The
solitary fibrous tumor is a rare mesenchymal tumor, occurring preferentially
in pleura, which has recently been described in extrathoracic sites. There
are 6 reports on primary solitary fibrous tumor of bladder. They affect
preferably men with mean age around 57 years, are usually asymptomatic
and, despite eventually presenting morphologic features of malignancy,
tumor resection is considered curative.
We report the seventh case of solitary fibrous
tumor in bladder wall, discussing differential diagnoses, and call the
attention to this rarely occurring entity, which has benign behavior and
should be managed conservatively.
Key
words: bladder; neoplasms, fibrous tissue; surgery
Int Braz J Urol. 2004; 30: 406-9
INTRODUCTION
Solitary
fibrous tumor is a rare mesenchymal neoplasia, primarily described in
visceral pleura, usually presenting benign behavior (1). Differently from
previous beliefs, they do not derive from mesothelium, but rather from
dendritic interstitial cells, which express CD34 and have generalized
distribution in tissues, a feature that helps to recognize it in other
organs (2). The identification of these extrathoracic tumors is important,
since recent reports of aggressive lesions have prompted a discussion
about their behavior, which was previously considered invariably benign
(3).
Cases of solitary fibrous tumor of meningeal
origin, in cerebral ventricle, orbit, nasal cavity and paranasal sinuses,
retroperitoneum, thyroid, major salivary glands, breast, liver, mediastinum
and gastrointestinal tract have been published (4). The urogenital tract
appears in isolated reports, comprising kidney, spermatic cord, seminal
vesicle and prostate. Only 6 cases of solitary fibrous tumor originated
in bladder wall have been published in the literature. We present one
case of primary solitary fibrous tumor in lateral bladder wall and review
other described cases affecting the same region.
CASE DESCRIPTION
Male,
60-year old patient with PSA of 4 ng/mL, with normal digital rectal examination,
was diagnosed with Gleason 6 (3 + 3) prostate adenocarcinoma involving
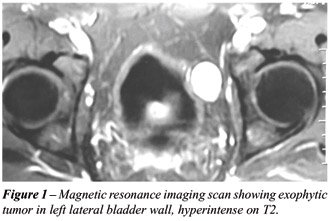
one of the 12 biopsy fragments. He underwent preoperative exams including
magnetic resonance imaging, which identified a tumoral mass close to the
left lateral bladder wall, measuring 3.0 cm, homogeneous, well delimited,
hyperintense in T2 weighted sequences, showing intense enhancement following
injection of contrast agent (Figure-1). This image was initially interpreted
as metastatic adenocarcinoma in iliac lymph node. Due to favorable aspects
of the tumor, normal digital rectal examination, low PSA levels, low Gleason
score and small tumor volume on biopsy, this possibility was discarded
and the patient underwent radical prostatectomy.
During the surgical act, pelvic examination
showed a tumoral mass located in left lateral bladder wall, exophytic
towards the external surface, completely separated from ileum, colon and
peritoneum. The mass was easily resected, and showed to derive from the
external layers of the detrusor muscle.
Eleven months after surgery, patient is
free from disease.
PATHOLOGY
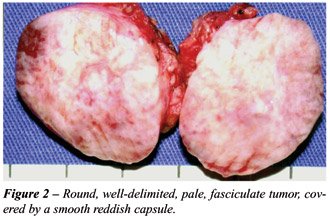
Macroscopic
examination showed a round tumoral mass with 3.2 cm in diameter, completely
involved by a thin smooth and reddish capsule, except in the surface that
contacts the bladder wall, where fragments of the muscularis propria layer
could be viewed. The cut surface revealed a pale, fasciculate, homogeneous
tumor, with elastic consistency, without necrosis or hemorrhage (Figure-2).
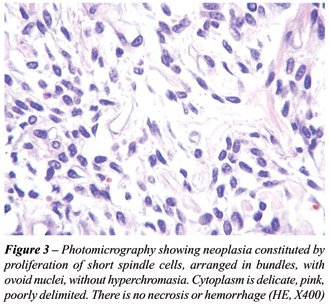
Histologically, the tumor was composed by
short spindle cells with ovoid nucleus, pale cytoplasm, arranged in interlaced
bundles with rare foci of stromal hyalinization, with a mitotic activity
of 3/10 HPF and absence of necrosis (Figure-3). The external portion of
the detrusor muscle was identified in continuity to the tumor.
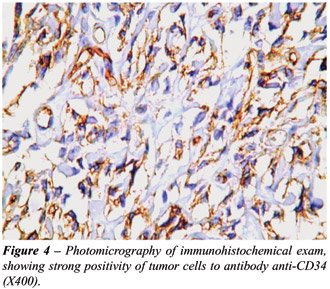
The immunohistochemical analysis showed
strong positivity of tumor cells to CD34 (BIRMA-K3, Dako, 1:100) (Figure-4)
and Bcl2 (Dako, 1:200). The lesion was negative for smooth muscle actin
(HHF-35, Dako, 1:400) protein S100 (Dako, 1:300), and CD117 (c-Kit, polyclonal,
Dako, 1:400). With this result, the final diagnosis was primary solitary
fibrous tumor in bladder wall.
COMMENTS
This
is the seventh case of solitary fibrous tumor originated in bladder wall
(5-8). It is a benign neoplasia, whose behavior depends on its size and
location. It affects preferentially men, with mean age around 57 years
(42 - 67 years). It is usually an incidental finding, with vague symptoms
being described, such as heaviness sensation, prolapse, increase in urinary
frequency and difficulty to void.
Only one patient presented hematuria. These
tumors vary in location and have a mean size of 8.0 cm (3.2 - 17 cm).
This diagnosis is difficult to make, and errors are common even in its
preferential site, the thorax. Those derived from the lower urinary tract,
invariably receive other denominations, including sarcomas. This mistake
is due to the small number of occurrences for this lesion in the urogenital
tract, and its histological presentation, which is similar to several
other entities, with absolutely distinct behavior. Hemangiopericytoma,
malignant fibrohistiocytoma, leiomyoma, leiomyosarcoma, schwannoma, carcinosarcoma
and gastrointestinal stromal tumor (GIST) are some examples.
The performance of an immunohistochemical
panel is mandatory in such conditions. The solitary fibrous tumor invariably
expresses CD34, with recent descriptions of positivity to Bcl2, type II
insulin-like growth factor and CD99 (4,7). The main differential diagnosis
in the presence of such panel would be hemangiopericytoma. It is an equally
rare tumor, with 5 described cases, 4 of them occurring in women, and
presents richer vascularization and tend to exhibit a less exuberant reactivity
to CD34 (4).
Approximately 10% of extrathoracic solitary
fibrous tumors are considered malignant, though they are less frequent
at these sites than in thorax. In bladder, despite some cases having some
malignant features, such as hypercellularity, nuclear pleomorphism and
mitotic activity higher than 4/10 HPF, the complete tumor resection has
shown to be curative.
In the case describe above, the tumor was
removed with safety margin, and within 11 months of follow-up, patient
has been free from disease. Thus, we call the attention of urologists
and pathologists so that they consider the diagnosis of solitary fibrous
tumor in the presence of spindle-cell bladder neoplasias, which can avoid
unnecessary radical surgeries.
REFERENCES
- Egland DM, Hochholzer L, McCarthy MJ: Localized benign and malignant fibrous tumors of the pleura. A clinico-pathologic review of 233 cases. Am J Surg Pathol. 1989; 13: 640-58. (Erratum in: Am J Surg Pathol. 1991; 15: 818.
- Van de Rijn M, Rouse V Robert: CD34, a review. Appl Immunohistochem. 1994; 2: 71-80.
- Vallat-Decouvelaere AV, Dry SM, Fletcher CD: Atypical and malignant solitary fibrous tumors in extrathoracic locations: evidence of their comparability to intra-thoracic tumors. Am J Surg Pathol. 1998; 22: 1501-11.
- Mentzel T, Bainbridge TC, Katenkamp D: Solitary fibrous tumour: clinicopathological, immunohistochemical, and ultrastructural analysis of 12 cases arising in soft tissues, nasal cavity and nasopharynx, urinary bladder and prostate. Virchows Arch. 1997; 430: 445-53.
- Bainbridge TC, Singh RR, Mentzel T, Katenkamp D: Solitary fibrous tumor of urinary bladder: report of two cases. Hum Pathol. 1997; 28: 1204-6.
- Westra WH, Grenko RT, Epstein J: Solitary fibrous tumor of the lower urogenital tract: a report of five cases involving the seminal vesicles, urinary bladder and prostate. Hum Pathol. 2000; 31: 63-8.
- Corti B, Carella R, Gabusi E, D´Errico A, Martorana G, Grigioni WF: Solitary fibrous tumour of the urinary bladder with expression of bcl-2, CD34, and Insulin-like Growth factor type II. Eur Urol. 2001; 39: 484-8.
- Ishikawa T, Kawabata G, Terakawa T, Kamidono S, Fujisawa M: Solitary fibrous tumor in the pelvic space. Urol Res. 2004; 32: 49-50.
___________________
Received: May 3, 2004
Accepted: July 11, 2004
_______________________
Correspondence address:
Dr. Kátia Ramos Moreira Leite
Rua Adma Jafet, 91
São Paulo, SP, 01308-050, Brazil
Fax: + 55 11 3231 2249
E-mail: katiaramos@uol.com.br