PREDICTION
OF PATHOLOGICAL STAGE IN PROSTATE CANCER THROUGH THE PERCENTAGE OF INVOLVED
FRAGMENTS UPON BIOPSY
(
Download pdf )
MARCOS F. DALL’OGLIO, ALEXANDRE CRIPPA, LUIS C. OLIVEIRA, JOAO F. NEVES NETO, KATIA R. LEITE, MIGUEL SROUGI
Division of Urology, Paulista School of Medicine, Federal University of Sao Paulo, UNIFESP, Sao Paulo, SP, Brazil
ABSTRACT
Introduction:
The need for defining the extension of disease in patients undergoing
radical prostatectomy due to prostate adenocarcinoma is a relevant factor
cure in such individuals. In order to identify a new independent preoperative
factor for predicting the extension of prostate cancer, we assessed the
role of the percentage of positive fragments upon biopsy.
Materials and Methods: A retrospective study
compared the percentage of positive fragments on biopsy with the extension
of disease as defined by the pathological examination of the surgical
specimen from 898 patients undergoing radical prostatectomy due to clinically
localized prostate cancer.
Results: On the univariate analysis, the
percentage of positive fragments on biopsy showed a statistical significance
for predicting confined disease (p < 0.001), which was found in 66.7%
of the cases under study. Additionally, we observed that the total number
of removed fragments exerts no influence on the extension of the disease
(p = 0.567).
Conclusion: the percentage of positive fragments
is an independent factor for predicting the pathological stage of prostate
adenocarcinoma, and the number of removed fragments is not related to
the extension of the disease.
Key
words: prostatic neoplasms; biopsy; needle; neoplasm staging
Int Braz J Urol. 2005; 31: 445-51
INTRODUCTION
According
to data from the National Cancer Institute at the Ministry of Health,
between 1979 and 2000 there was an increase of 141% in mortality due to
prostate adenocarcinoma in Brazil, making this disease the second cause
of death from tumors in males, second only to lung cancer. Prostate cancer
also represents the second most prevalent malignant neoplasm, behind skin
cancer. In 2003 in Brazil, 35,240 new cases were predicted, with 8230
deaths due to prostate adenocarcinoma (1). These figures are approximately
10 times lower than those estimated for the United States of America by
the National Cancer Institute, where prostate cancer was responsible for
10% of deaths from malignant neoplasms in 2004, second only to lung cancer
(2).
Among the available treatments in cases
of localized prostate adenocarcinoma, the most frequently performed is
radical prostatectomy, which is used in 52% of patients, followed by external
radiotherapy or brachytherapy, which is used in approximately 20% of patients
(3).
The great challenge in clinical practice
is to perform an accurate early diagnosis of confined disease, since in
more than 30% of cases judged as localized, the subsequent pathological
study shows more advanced disease than was initially expected (4).
Aiming to clinically define the presence
of localized disease, and thus, the feasibility for curative treatment,
most experts consider especially the initial PSA levels, the tumor extension
upon digital rectal examination and the degree of neoplastic differentiation
as assessed by the Gleason score (5). New parameters for predicting the
chances of disease recurrence and the presence of organ-confined tumors
have also been studied (6,7), including the number of fragments positive
to cancer on biopsy, which seems to represent an independent prognostic
factor (8).
Considering that the percentage of fragments
involved by tumor on biopsy represents an important prognostic factor
(6,9), we devised the present study, which intends to analyze the preoperative
predictive role of the percentage of positive fragments upon biopsy for
predicting the extension of disease.
MATERIALS AND METHODS
We
retrospectively analyzed 960 patients diagnosed with localized prostate
cancer undergoing retropubic radical prostatectomy whose medical charts
recorded the total number of biopsied fragments, the number of fragments
with cancer, the Gleason score on biopsy, the serum PSA levels and the
pathological exam of the surgical specimen. Fifty-four patients who had
received neoadjuvant treatment were excluded, as were 8 patients whose
diagnosis was obtained by endoscopic resection of the prostate or transvesical
prostatectomy, thus totaling 62 excluded cases and 898 inclusions. Patient
ages ranged from 40 to 83 years, with a mean age of 62.9 years.
The clinical staging (Table-1) used the
TNM classification (10). For this purpose, auxiliary examinations were
performed, including digital rectal examination, transrectal ultrasound
of the prostate, abdominal and pelvic computerized tomography or magnetic
resonance imaging, bone scintigraphy and thorax radiography.
Patients underwent retropubic radical prostatectomy
with bilateral selective iliac lymphadenectomy. All interventions were
performed by the same surgeon (MS).
All surgical specimens consisting of the
prostate, seminal vesicles and obturator lymph nodes were assessed by
the same pathology (KML).
The specimens were fixed in 10% formol for
approximately 6 hours and underwent a routine starting with measuring
and weighing the gland. Thin transversal sections were performed on the
surgical margins relative to the bladder neck and the prostate apex. Using
the urethra as a reference, the remaining gland was immersed in India
ink stain and then sequentially sliced each 3 millimeters. 8 to 10 sections
from each lobe were included for histological examination. Seminal vesicles
were sectioned at the base and prepared for histological examination following
longitudinal sectioning. Obturator lymph nodes were dissected and sliced
in order to go through pathological examination.
Following the usual preparation in paraffin,
the sections were stained by HE and analyzed under binocular light microscope.
Parameters assessed were:
Infiltration of periprostatic tissue –
Periprostatic involvement was defined as the neoplastic invasion of fat
tissue and periprostatic neurovascular plexus. In such cases, the disease
was classified as non-confined.
Infiltration of seminal vesicles –
The involvement of seminal vesicles was considered only when their parenchyma
– and not the adventitial region – was involved in the tumor.
Metastases to lymph nodes – Obturator
lymph nodes that were involved by tumor were classified as having metastases.
Postoperative pathological staging –
the TNM staging system was used for the final analysis (10). The distribution
of patients under study is reported in Table-2.
The frequency of organ-confined disease,
periprostatic extension and invasion of seminal vesicles was compared
with the percentage of positive fragments. For this purpose, the percentage
of positive fragments was divided into four categories: 0 - 25%; 25.1
- 50%; 50.1 - 75% and 75.1 - 100%. We also divided the number of fragments
collected on biopsy into 3 categories: less than 6; 6; and more than 6,
and compared them with the extension of disease.
Statistical
Analysis
In order to compare the percentages of positive
fragments on biopsy with confined or non-confined disease, we used the
Pearson’s Qui-Square test (univariate analysis). For comparing the
mean percentage of positive fragments on biopsy with confined or non-confined
disease, we used the student’s t test following the analysis of
distribution normality for percentages of positive fragments. A significance
level of 5% was adopted, with results being considered as statistically
significant when they showed p < 0.05.
RESULTS
Figure-1
shows that the number of fragments removed on biopsy did not interfere
with the pathological results of surgical specimens (p = 0.567), thus
evidencing the uniformity of cases under study.
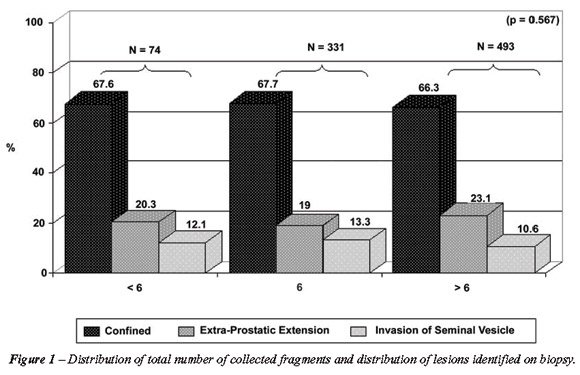
Figure-2 compares the percentage of positive
fragments and the presence of organ-confined disease. According to the
data obtained in the study, there is a positive association between the
percentage of positive fragments on biopsy and the stage of disease (p
< 0.001).
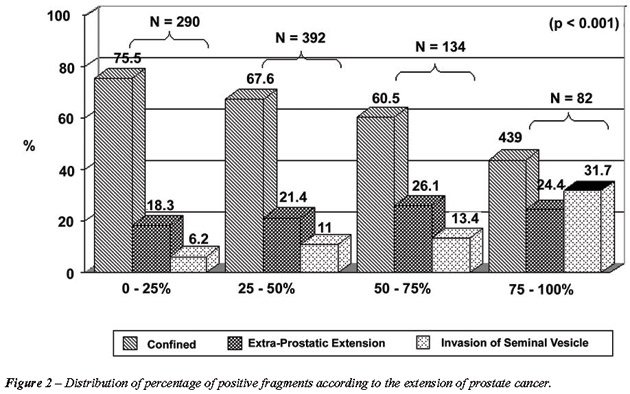
Table-3 compares the mean percentage of
positive fragments between confined and non-confined disease. The percentage
of positive fragments on average is 9.72% (± 1.68) higher in patients
with non-confined disease (p < 0.001).
Table-4 shows that regardless of results
from the surgical specimen, approximately 55% of patients had more than
six fragments removed.
In Table-5 we can see that regardless of
results from the surgical specimen, the average of collected fragments
was 8 ± 3, with a minimum of 2 and a maximum of 22 fragments removed
on biopsy.
We can see in Table-6 that regardless of
results from the surgical specimens, the average of positive fragments
was 3.2 ± 2.1, with the minimal number of positive fragments being
one and the maximal 20.
COMMENTS
In
our study, 66.7% of patients had neoplasm confined to the gland following
radical prostatectomy, with this figure ranging from 13 to 82% (11,12).
This variation depends mainly on Gleason score, PSA, clinical stage and,
currently, the percentage of positive fragments on biopsy.
D’Amico et al. (9) observed that the
percentage of positive fragments on biopsy is an important parameter for
predicting confined disease, demonstrating that when less than 34% of
the fragments are affected, 79% of the patients have gland-confined disease,
and when the number of affected fragments is greater than 50%, only 43%
have confined disease. In our work, we observed that when there are less
than 25% of fragments affected by tumor, the chance of confined disease
is 75.5%, and only 43.9% of individuals with more than 75% of positive
fragments on biopsy have confined disease.
When comparing the percentage of fragments
involved in cancer with the possibility of involvement of the seminal
vesicles by the neoplasm, we verified that when only one fragment has
neoplasm, the risk of seminal vesicles being positive to cancer is 6%;
however, when there are six fragments involved, this risk raises to 83%
(4). Our study revealed that involvement of the seminal vesicles in 6.2%
of patients when less than 25% of fragments had cancer, versus 31.7% when
more than 75% were affected.
The importance of the number of positive
fragments on biopsy for predicting confined disease is related to the
number of positive fragments and the results obtained with radical prostatectomy.
When the disease is confined, the average of positive fragments is 35%,
while in individuals with non-confined disease this average rises to 55%
(7). In our work, we found similar figures, with an average of 38% for
confined disease versus 47.7% for non-confined disease.
The percentage of positive fragments has
a linear relationship with tumor volume in the surgical specimen (13).
Additionally, for each 1% increase in the affected fragments, the risk
of non-confined disease increases by 2% (14).
In cases followed over 5 years, Epstein
et al. (15) observed that approximately 26% of patients with less than
4 cc of tumor in the surgical specimen evidenced a recurrence of the disease
and almost 50% of patients with more than 4 cc had a progression in the
disease, thus demonstrating the importance of tumor volume for the outcome
of disease. Similarly, Stamey et al. (16) confirmed the prognostic importance
of tumor volume and reported that 86% of patients with volume between
0.5 and 2.0 cc did not experience a progression of the disease, in opposition
to patients with more than 12 cc of tumor volume, of which 96% evidenced
a biochemical recurrence of the disease. Upon understanding the importance
of tumor volume in relation to the risks of recurrence of disease, the
number of positive fragments on biopsy has been used to predict the occurrence
of non-confined disease and recurrence following radical prostatectomy
(9,17). Nevertheless, some polemics involve the subject, since some studies
suggest that we should not consider the percentage of positive fragments
but the percentage of cancer found in each fragment, which would be a
more accurate predictive factor (18). However, studies comparing the percentage
of positive fragments on biopsy with the percentage of tissue affected
by cancer (14,19) have demonstrated that both methods are strongly associated
with the definition of non-confined disease (20). Since the final result
appears to be equal, and the calculation of the area with cancer in the
fragments is more time-consuming and complex, it is advantageous to use
the percentage of positive fragments on biopsy in the clinical practice.
Prostate adenocarcinoma is the third cause
of death from cancer in males in the world, and its incidence and mortality
are increasing in our country, due to the increase in life expectancy,
improvement and dissemination of diagnostics methods, and unknown etiopathogenic
factors. In order to improve the accurate preoperative diagnosis of confined
disease, we should intensify the studies on the parameters that should
be used, thus allowing more effective interventions and, consequently,
increasing the chances of cure for patients with this disease. In this
context, the present study aimed to define and consolidate a new parameter
that should be considered for assessing the extension of disease preoperatively.
CONCLUSION
The percentage of positive fragments on biopsy is an independent preoperative factor (univariate analysis) for predicting the pathological stage of prostate cancer in the surgical specimen, and the number of fragments removed on biopsy has no influence on the extension of disease.
Adriana Sanudo performed the statistical analysis.
REFERENCES
- Brazil. Ministry of Health. National Cancer Institute. Estimate of cancer and mortality for cancer in Brazil 2003. Available at: www.inca.gov.br/estimativas/2003. Accessed on: 02/26/2004. [in Portuguese]
- Jemal A, Tiwari RC, Murray T, Ghafoor A, Samuels A, Ward E, et al.: Cancer statistics, 2004. CA Cancer J Clin. 2004; 54: 8-29.
- Cooperberg MR, Broering JM, Litwin MS, Lubeck DP, Mehta SS, Henning JM, et al.: The contemporary management of prostate cancer in the United States: lessons from the cancer of the prostate strategic urologic research endeavor (CapSURE), a national disease registry. J Urol. 2004; 171: 1393-401.
- Peller PA, Young DC, Marmaduke DP, Marsh WL, Badalament RA: Sextant prostate biopsies. A histopathologic correlation with radical prostatectomy specimens. Cancer. 1995; 75: 530-8.
- Han M, Partin AW, Zahurak M, Piantadosi S, Epstein JI, Walsh PC: Biochemical (prostate specific antigen) recurrence probability following radical prostatectomy for clinically localized prostate cancer. J Urol. 2003; 169: 517-23.
- Gancarczyk KJ, Wu H, McLeod DG, Kane C, Kusuda L, Lance R, et al.: Using the percentage of biopsy cores positive for cancer, pretreatment PSA, and highest biopsy Gleason sum to predict pathologic stage after radical prostatectomy: the Center for Prostate Disease Research nomograms. Urology. 2003; 61: 589-95.
- Sebo TJ, Bock BJ, Cheville JC, Lohse C, Wollan P, Zincke H: The percent of cores positive for cancer in prostate needle biopsy specimens is strongly predictive of tumor stage and volume at radical prostatectomy. J Urol. 2000; 163: 174-8.
- Grossfeld GD, Latini DM, Lubeck DP, Broering JM, Li YP, Mehta SS, et al.: Predicting disease recurrence in intermediate and high-risk patients undergoing radical prostatectomy using percent positive biopsies: results from CapSURE. Urology. 2002; 59: 560-5.
- D’Amico AV, Whittington R, Malkowicz SB, Schultz D, Fondurulia J, Chen MH, et al.: Clinical utility of the percentage of positive prostate biopsies in defining biochemical outcome after radical prostatectomy for patients with clinically localized prostate cancer. J Clin Oncol. 2000; 18: 1164-72.
- Schroder FH, Hermanek P, Denis L, Fair WR, Gospodarowicz MK, Pavone-Macaluso M: The TNM classification of prostate cancer. Prostate Suppl. 1992; 4: 129-38.
- Partin AW, Yoo J, Carter HB, Pearson JD, Chan DW, Epstein JI, et al.: The use of prostate specific antigen, clinical stage and Gleason score to predict pathological stage in men with localized prostate cancer. J Urol. 1993; 150: 110-4.
- Freedland SJ, Csathy GS, Dorey F, Aronson WJ: Percent prostate needle biopsy tissue with cancer is more predictive of biochemical failure or adverse pathology after radical prostatectomy than prostate specific antigen or Gleason score. J Urol. 2002; 167: 516-20.
- Rubin MA, Mucci NR, Manley S, Sanda M, Cushenberry E, Strawderman M, et al.: Predictors of Gleason pattern 4/5 prostate cancer on prostatectomy specimens: can high grade tumor be predicted preoperatively? J Urol. 2001; 165: 114-8.
- Sebo TJ, Cheville JC, Riehle DL, Lohse CM, Pankratz VS, Myers RP, et al.: Predicting prostate carcinoma volume and stage at radical prostatectomy by assessing needle biopsy specimens for percent surface area and cores positive for carcinoma, perineural invasion, Gleason score, DNA ploidy and proliferation, and preoperative serum prostate specific antigen: a report of 454 cases. Cancer. 2001; 91: 2196-204.
- Epstein JI, Carmichael M, Partin AW, Walsh PC: Is tumor volume an independent predictor of progression following radical prostatectomy? A multivariate analysis of 185 clinical stage B adenocarcinomas of the prostate with 5 years of follow up. J Urol. 1993; 149: 1478-81.
- Stamey TA, McNeal JE, Yemoto CM, Sigal BM, Johnstone IM: Biological determinants of cancer progression in men with prostate cancer. JAMA. 1999; 281: 1395-400.
- Ravery V, Chastang C, Toublanc M, Boccon-Gibod L, Delmas V, Boccon-Gibod L: Percentage of cancer on biopsy cores accurately predicts extracapsular extension and biochemical relapse after radical prostatectomy for T1-T2 prostate cancer. Eur Urol. 2000; 37: 449-55.
- Bostwick DG, Grignon DJ, Hammond ME, Amin MB, Cohen M, Crawford D, et al.: Prognostic factors in prostate cancer. College of American Pathologists Consensus Statement 1999. Arch Pathol Lab Med. 2000; 124: 995-1000.
- Linson PW, Lee AK, Doytchinova T, Chen MH, Weinstein MH, Richie JP, et al.: Percentage of core lengths involved with prostate cancer: does it add to the percentage of positive prostate biopsies in predicting postoperative prostate-specific antigen outcome for men with intermediate-risk prostate cancer? Urology. 2002; 59: 704-8.
- Ojea Calvo A, Nunez Lopez A, Dominguez Freire F, Alonso Rodrigo A, Rodriguez Iglesias B, Benavente Delgado J, et al.: Correlation of the anatomo-pathological staging of radical prostatectomy specimens with the amount of cancer in the preoperative sextant biopsy. Actas Urol Esp. 2003; 27: 428-37.
_______________________
Received: February 1, 2005
Accepted after revision: May 16, 2005
_______________________
Correspondence address:
Dr. Marcos F. Dall’Oglio
Rua Barata Ribeiro, 398 / 501
São Paulo, SP, 01308-000, Brazil
Fax: + 55 11 3159-3618
E-mail: marcosdallogliouro@terra.com.br