PUBOVAGINAL
SLING WITH A LOW-COST POLYPROPYLENE MESH
(
Download pdf )
FRANSBER R. RODRIGUES, ROMULO MAROCCOLO FILHO, ROBERTO R. MAROCCOLO, LUCIO C. PAIVA, FERNANDO A. DIAZ, EDUARDO C. RIBEIRO
Service of Urology, Brasilia University Hospital, Brasilia, DF, Brazil
ABSTRACT
Objective:
The aim of this study was to present the results of pubovaginal sling
with a low-cost polypropylene mesh in the treatment of stress urinary
incontinence.
Materials and Methods: 118 women diagnosed
with stress urinary incontinence (SUI) due to urethral hypermobility or
intrinsic sphincteric deficiency, treated with pubovaginal sling (PVS)
with a low-cost polypropylene mesh confectioned by the surgeon, were analyzed.
All patients had a basic evaluation that included a medical history, physical
examination, stress tests and urodynamic investigation.
Results: The average follow up was of 42
months. Urethral hypermobility was observed in 67% of the cases. The process
was carried out on an outpatient basis on 67 patients. Intra-operative
complications included 4 vesical injuries, treated with catheterization
for 3 days. There were 13 early complications, of which 8 were urinary
retentions treated with vesical drainage for 1 to 3 weeks and 3 vaginal
extrusions of the mesh treated with covering of the sections with mucous
membrane. There was a need for 6 urethrolysis in patients who presented
irritative and postoperative obstructive symptoms; 81.3% of the patients
were considered cured, while 9.3% had significant improvement. Three initially
unsuccessful cases required sling reconfiguration. All cases were eventually
cured.
Conclusion: The construction of a pubovaginal
sling using a low-cost polypropylene mesh is a safe and effective technique
for the relief of SUI. It should be considered an alternative, especially
for patients in public health systems with low financial resources.
Key
words: urinary incontinence, stress; prostheses and implants;
suburethral slings; polypropylene
Int Braz J Urol. 2007; 33: 690-94
INTRODUCTION
Suburethral
slings have become the preferred technique for the treatment of stress
urinary incontinence (SUI) (1). The Integral Theory and concept of a medium
tension free urethral sling, surgical refinements and new materials allowed
these procedures to be carried out in a non invasive manner, with low
morbidity rates and satisfactory results (2-4).
Various materials were used in the slings,
from autogenous tissues to synthetic materials, and the choices were based
upon well-defined criteria, in which the cost was one of the most important
factors for the selection of materials, mainly in countries with limited
public health resources (5).
Studies confirm that the choice of a tension
free polypropylene mesh allow high success rates and the TVT®
simplified the SUI therapy, becoming one of most common options for the
treatment of this disease (3,6). Thus, the industry has offered different
kits to make the slings, but most of the time the costs are prohibitive
for public health systems with few financial resources.
The objective of this study is to analyze
the results of pubovaginal sling (PVS) using a low-cost polypropylene
mesh for the treatment of stress urinary incontinence (SUI).
MATERIALS AND METHODS
A
retrospective study of 118 women with SUI treated with PS using a low
cost polypropylene mesh was conducted from April 2002 to April 2006. The
preoperative evaluation consisted of the medical history, urogynecological
examination, stress tests and a urodynamic assessment cystometry, measure
of the leak point pressure and flux-pressure study. The etiology of SUI
was considered urethral hypermobility when the leak point pressure under
stress (VLPP) was greater than 60 cmH2O, and intrinsic sphincteric
deficiency (ISD) when the pressure was below that value.
The follow up was carried out with consultations
in the first month after the treatment and every 4 months, in which stress
tests and clinical histories were obtained. Urodynamic studies were indicated
in patients with persistence of SUI, irritative and/or moderate obstructive
symptoms, or urinary retention 30 days after the surgical procedure.
Patients who related satisfaction and did
not express urinary loss after stress tests were considered cured. Patients
in use of pads for precaution, due to minimal urinary loss, but satisfied
with the results were considered patients with significant recovery. The
other cases were classified as failures.
Surgical
Technique
All the procedures were carried out under
spinal anesthesia, except 1 patient who underwent concomitant laparoscopic
surgery. Patients received first generation cephalosporin as a prophylactic
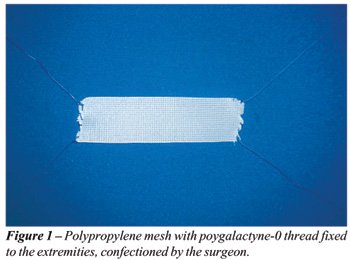
antibiotic. The surgical technique adopted was similar to the technique
described by Almeida and Raz (6), using a polypropylene mesh of 10 x 1.5
cm, with polygalactyne-0 threads fixed at each extremity of the mesh,
confectioned by the surgeon (Figure-1).
A longitudinal incision of 2 cm was made
on the anterior vaginal wall, 1 cm from the urethral meatus, and dissection
of the periurethral spaces was done. The endopelvic fascia was opened
on each side, with access to the retropubic space. A hypogastric incision
of 2 cm was made on the upper border of the pubic bone, allowing the passage
of the long tongs to the retropubic space, bringing them out through the
vaginal incision at each side of the urethra. The threads at the extremities
of the mesh were held by the tongs and pulled till the abdominal incision,
where they were tied after confirmation of the absence of vesical injuries
by cystoscopy, in such a manner that the mesh stays below the urethra,
free of tension.
RESULTS
The
average age was 52 years (29-77 years). From the 118 patients, 2 had been
treated previously with Burch colposuspension and 23 received surgical
indications after failure of perineal physiotherapy. Eighty patients were
diagnosed with urethral hypermobility (67%), from which 4 presented detrusor
hyperactivity, and 38 were diagnosed with ISD (33%). The stress test was
positive in all cases. Fifty six women (48%) used pads daily, with an
average of 1.7 pad/day. The medium VLPP was 84 cmH2O. Fifty-two patients
(44%) presented irritative symptoms before the surgery.
Procedures associated to PVS were carried
out in 17 cases, described in Table-1. The average operative time was
49 minutes, including other concomitant procedures. The surgery was carried
out on an outpatient basis on 67 patients (56%), with an average operative
time of 28 minutes. Four vesical injuries (3.3%) were observed during
the procedures and were treated with a vesical tube for 3 days. No cases
of substantial hemorrhage were observed.
Post-operative complications are described
in Table-2. All cases of acute urinary retention were resolved with vesical
tubes for 1-3 weeks. The 3 cases of vaginal mesh extrusion (2.5%) were
treated with coverage by the vaginal mucosa, with success in 2 patients.
The third patient presented recurrent erosion, requiring removal of the
mesh segment, but persisting continent.
Average post-operative follow up was 42
months (14-61 months). After the procedure, 5 patients presented irritative
urinary symptoms “de novo” (4.2%), without detrusor hyperactivity
on postoperative urodynamics. All patients with preoperative detrusor
hyperactivity continued with irritative symptoms, however without SUI.
From the 52 patients with preoperative irritative symptoms, 40 (76.9%)
reported improvement of symptoms. There was necessity for urethrolysis
in 6 patients (5%) who continued with significant irritative symptoms
and a suspicious infra-vesical obstruction on urodynamics. Three patients
from this group continued continent, while the others underwent a new
PVS using the initial technique, and presented incontinence resolution.
Ninety six patients (81.3%) were considered
cured, and 11 patients (9.3%) presented significant improvement of incontinence.
From the 11 women who did not benefit from the treatment, 3 underwent
a new PVS, achieving continence. The others are being followed up by the
perineal physiotherapy staff.
COMMENTS
The
Integral Theory postulates that female urinary continence occurs due to
the closing of the medium portion of the urethra, which depends on the
integrity of pubourethral ligaments and the suburethral support given
by the anterior wall of the vagina. Similar to TVT®, the
technique discussed here is based on this theory, positioning the sling
in the medial third of the urethra, free of tension. The principal difference
lies in the cost of the material used, since in this study the same propylene
mesh was used, however it was prepared by the surgeon, instead of the
specific commercialized material for this procedure. The propylene mesh
and polygalactyne thread approximately costs U$ 15.00.
The sling made of autogenous tissue, like
the abdominal rectus fascia or fascia lata, has shown good long-term results.
However, the high morbidity rates associated to the procedure pose a disadvantage
(7-9). The use of cadaverous fascia would eliminate some inconveniences
and, in short term, produce similar results to that observed with autogenous
slings (10); however, further studies have not confirmed these initial
good results (11). This scenario led to the development of synthetic materials
for slings, especially polypropylene, which is very durable, has low indices
of rejection and is easily available.
The main intraoperative complications of
PVS were vesical perforation and hemorrhage. Bousted (4), in a metanalysis,
observed 6.9% of vesical perforations in 160.000 patients treated with
TVT®. Tamoussino et al. (12) verified vesical injuries
in 2.7% of 2.795 patients from the Austrian series. According to data
from Meshia et al. (13), bleeding was reported in 15 % of the cases. In
this series, low incidence of intraoperative complications was observed,
including 4 vesical injuries (3.3%), and there were no significant cases
of hemorrhage.
Postoperative complications included 8 cases
of urinary retention (6.7%), and vaginal erosion of the mesh in 3 patients
(2.5%); there were also isolated cases of pubic hematoma and acute vaginitis.
A variable incidence of urinary retention after the TVT®
was reported (2.3%-43%), in which an increase is observed when associated
to other pelvic procedures (14,15). The vaginal erosion of the mesh was
observed in approximately 1% of the cases. Patients who presented this
complication were treated with simple procedures, with good results.
Resolution of preoperative irritable symptoms
was observed in 76.9% of the women, and 4.2% presented “de novo”
urinary urgency, without detrusor hyperactivity. The incidence of this
symptom is not consistent in literature, being reported in 1% to 35% of
patients (16,17). In this study, obstructive and/or irritative symptoms
persisted in 6 patients (5%), and all underwent urethrolysis, with improvement
in all cases.
Bousted analyzed the results from 16 studies
about TVT®, with a minimum follow up of 12 months, observing
objective cure rates of 80% to 96%, and 5% to 17% of significant improvement
(4). In the present study, the cure rate (81.3%) and significant improvement
(9.3%) are similar to those obtained by TVT®, even in patients
diagnosed with ISD, whose results tend to be worse. Rezapour et al. (18)
obtained cure in 74% and an important improvement in 12% of the patients
with ISD that underwent sling with TVT®.
CONCLUSION
Complications and cure rates of the pubovaginal sling (PVS) using a low cost polypropylene mesh can be compared to those of TVT® for the treatment of SUI, with an advantage of lower costs. This procedure should be considered as an alternative to PVS with commercial kits, mainly for patients of public health systems with few financial resources.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Niknejad K, Plzak LS 3rd, Staskin DR, Loughlin KR: Autologous and synthetic urethral slings for female incontinence. Urol Clin North Am. 2002; 29: 597-611.
- Petros PE, Ulmsten UI: An integral theory and its method for the diagnosis and management of female urinary incontinence. Scand J Urol Nephrol Suppl. 1993; 153: 1-93.
- Leach GE, Dmochowski RR, Appell RA, Blaivas JG, Hadley HR, Luber KM, et al.: Female Stress Urinary Incontinence Clinical Guidelines Panel summary report on surgical management of female stress urinary incontinence. The American Urological Association. J Urol. 1997; 158: 875-80.
- Bousted GB: The tension-free vaginal tape jfor treating female stress urinary incontinence. BJU int. 2002; 89: 687-9.
- Palma PC: Which sling for which patient? Int Urogynecol J. 2004; 15: 369-2.
- Rodriguez LV, Raz S: Prospective analysis of patients treated with a distal urethral polypropylene sling for symptoms of stress urinary incontinence: surgical outcome and satisfaction determined by patient driven questionnaires. J Urol. 2003; 170: 857-63; discussion 863.
- Bemelmans BL, Chapple CR: Are slings now the gold standard treatment for the management of female urinary stress incontinence and if so which technique? Curr Opin Urol. 2003; 13: 301-7.
- Cross CA, Cespedes RD, McGuire EJ: Our experience with pubovaginal slings in patients with stress urinary incontinence. J Urol. 1998; 159: 1195-8.
- Elliott DS, Boone TB: Is fascia lata allograft material trustworthy for pubovaginal sling repair? Urology. 2000;56: 772-6.
- Singla AK: The use of cadaveric fascia lata in the treatment of stress urinary incontinence in women. BJU Int. 2000; 85: 264-9.
- O’Reilly KJ, Govier FE: Intermediate term failure of pubovaginal slings using cadaveric fascia lata: a case series. J Urol. 2002; 167: 1356-8.
- Tamussino K, Hanzal E, Kolle D, Ralph G, Riss P, Austrian Urogynecology Working Group: The Austrian tension-free vaginal tape registry. Int Urogynecol J Pelvic Floor Dysfunct. 2001; 12 (Suppl 2): S28-9.
- Meschia M, Pifarotti P, Bernasconi F, Guercio E, Maffiolini M, Magatti F, et al.: Tension-Free vaginal tape: analysis of outcomes and complications in 404 stress incontinent women. Int Urogynecol J Pelvic Floor Dysfunct. 2001; 12 (Suppl 2): S24-27.
- Kuuva N, Nilsson CG: A nationwide analysis of complications associated with the tension-free vaginal tape (TVT) procedure. Acta Obstet Gynecol Scand. 2002; 81: 72-7.
- Partoll LM: Efficacy of tension-free vaginal tape with other pelvic reconstructive surgery. Am J Obstet Gynecol. 2002; 186: 1292-5; discussion 1295-8.
- Debodinance P, Delporte P, Engrand JB, Boulogne M: Tension-free vaginal tape (TVT) in the treatment of urinary stress incontinence: 3 years experience involving 256 operations. Eur J Obstet Gynecol Reprod Biol. 2002; 105: 49-58.
- Fynes M, Murrey C, Carey M, Rosamilia A, Dwyer P: Prognostic factors for continence outcome following tension-free vaginal tape. An observational study. Int Urogynecol J Pelvic Floor Dysfunct. 2000; 11 (suppl 1): S33.
- Rezapour M, Falconer C, Ulmsten U: Tension-Free vaginal tape (TVT) in stress incontinent women with intrinsic sphincter deficiency (ISD)—a long-term follow-up. Int Urogynecol J Pelvic Floor Dysfunct. 2001; 12 (Suppl 2): S12-14.
____________________
Accepted
after revision:
July 03, 2007
_______________________
Correspondence address:
Dr. Fransber Rondinelle Araújo Rodrigues
CSB 07, lote 04, ap.304, Taguatinga
Distrito Federal, DF, 72015-575, Brazil
Fax: + 55 61 3351-0045
E-mail: fransber.rodrigues@sbu.org.br