EXTRAVAGINAL
TESTICULAR TORSION: A CLINICAL ENTITY WITH UNSPECIFIED SURGICAL ANATOMY
(
Download pdf )
IASON D. KYRIAZIS, JOHN DIMOPOULOS, GEORGE SAKELLARIS, JURGEN WALDSCHMIDT †, GEORGE CHARISSIS
Department of Pediatric Surgery (IDK, JD, GS, GC), University Hospital of Heraklion, Greece, and Department of Pediatric Surgery (JW, GC), Universitaetsklinikum Benjamin Franklin, Freie Universitaet Berlin, Berlin, Germany
† In memorian
ABSTRACT
Purpose:
To review and evaluate the anatomical definitions of perinatal extravaginal
torsion (EVT) of the testis.
Materials and Methods: An extensive review
of the literature was made to reveal the prevalent anatomical background
predisposing to EVT. Gross appearance of twisted testes obtained during
surgery for 14 cases of EVT was used to test the validity of the above
theories.
Results: The most commonly accepted suggestions
describe an EVT within dartos muscle that includes all layers of spermatic
cord or an EVT outside parietal layer of tunica vaginalis within internal
spermatic fascia. However, both of them were found inadequately documented,
while a large volume of controversial data has been accumulated, that
raises doubts regarding the validity of such definitions. The gross appearance
of twisted testes failed to confirm both an EVT including all layers of
the spermatic cord and also an EVT outside tunica vaginalis as possible
mechanisms of torsion.
Conclusion: The anatomical basis of EVT
remains unclear and further investigation is required.
Key
words: testis; spermatic cord; anomalous; torsion
Int Braz J Urol. 2008; 34: 617-26
INTRODUCTION
Extravaginal torsion (EVT) of the testis is reported to be the predominant mechanism of torsion in the fetus and neonate. In this kind of torsion, twist of the spermatic cord is taking place outside the sack of tunica vaginalis in the scrotum. Accordingly, this entity is considered to have a different surgical anatomy, than the one reported in older children and adults who demonstrate the bell clapper deformity and torsion of the testis occurs intravaginally (1). This article reviews and evaluates the current theories on the anatomical basis of EVT given that the low incidence of perinatal torsion and the poorly documented anatomical findings at operation have left surgical anatomy of this clinical entity poorly defined.
MATERIALS AND METHODS
Photographic data from 14 cases of perinatal testicular torsion, operated by Professor Waldschmidt and Professor Charissis between 1973 and 2006, were examined retrospectively to define the gross appearance of EVT. Moreover, an extensive review of the literature was carried out to reveal the most commonly accepted definitions concerning the surgical anatomy predisposing to EVT. In particular, all related articles appearing in PubMed under the search terms “extravaginal”, “perinatal”, “testicular torsion” were examined for reference in anatomy of perinatal torsion in addition with referred pathological anatomy of perinatal torsion in text books on Urology and Pediatric Surgery. Finally, evaluation of the proposed theories illustrated by our gross appearance photos of the twisted mass was performed.
RESULTS
Gross
Appearance of Extravaginal Torsion
EVT is considered to be an antenatal event
and probably because of the different time intervals between time of torsion
and time of observation, gross appearance of twisted mass varies from
case to case. However, there were some common characteristics found in
all of our cases that can be drawn and described. Our photographic data
demonstrated that EVT is usually constituted by a narrow, twisted pedicle
that suspends a dark globular mass containing an infracted testis and
epididymis, which appears immediately after opening the skin and dartos
muscle (Figure-1). Moreover, as histologically evidenced by the most substantiated
work on the subject by Herman et al., twisted tissues are surrounded by
a smooth membrane layer sequestering an underlying hemorrhage (2) (Figure-2).
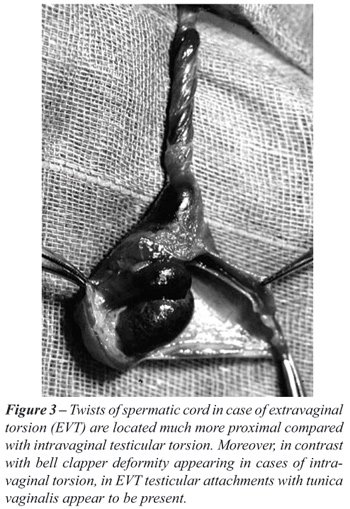
Moreover, in contrast with intravaginal torsion where torsion occurs intravaginaly,
in cases of EVT, twists of the spermatic cord are located outside the
cavity created by the two layers of tunica vaginalis (Figure-1,2 and 3).
Finally, although due to the usual chronic character of this antenatal
event in EVT scrotal anatomy is found greatly altered, and identification
of particular anatomical structures within the twisted mass becomes very
difficult, testicular attachments with the parietal layer of tunica vaginalis
were in fact present, an observation in accordance with most other anatomical
references on the subject (Figure-3) (3-5). Each theory on surgical anatomy
of EVT must be consistent with these gross characteristics.


Theories
on the Anatomical Basis of Extravaginal Torsion
The literature review revealed 2 controversial
anatomical definitions of EVT (6,7). These describe an extravaginal torsion
within dartos muscle, including all layers of the spermatic cord and an
extravaginal torsion within internal spermatic fascia, outside the parietal
layer of tunica vaginalis (Figure-4). For discriminative reasons we will
refer to them as EVT outside or inside the cremaster muscle.

Torsion
Outside Cremaster Muscle
There is evidence that in perinatal period
of life a lack of attachments of the entire scrotal contents with the
scrotal wall is present, allowing testis and its tunics to demonstrate
an unusual mobility. Cooper (1830) and Jerkings et al. (1983) first proposed
this lack of attachment because of the ease with which the intrascrotal
contents could be lifted out in newborns, without tearing any fascial
attachments (5,6). More precisely, external spermatic fascia does not
seem to be adherent to the dartos muscle. These attachments are suggested
to be formed during the first 7 to 10 days of life anchoring the spermatic
cord into the scrotum (7). Numerous authors use this fact to report that
EVT is predisposed by this lack of attachments and accordingly, twists
of the cord occur outside cremaster muscle and its fascia (external spermatic
fascia), within dartos muscle, including all layers of spermatic cord
(6-9) (Figure-4a). According to this point of view, EVT should become
impossible after the first days of life, when connection of testicular
tunics with the scrotum is established. Gross appearance of EVT reinforce
the above mentioned theory, since the black necrotic twisted mass noted
immediately on opening the dartos muscle clearly indicates a torsion involving
all layers of spermatic cord (Figure-3).
However, this perinatal lack of attachments
is a normal condition appearing in all newborns up to 7-10 days after
birth. According to Noseworthy (2002) the above mentioned explanation
of EVT poorly supports the relatively rare occurrence of this condition.
If lack of fixation in all newborns was a predisposing factor for EVT,
this should lead to a considerably higher incidence of EVT during the
perinatal life (10). In addition, EVT has been reported in older patients
at 12-14 years of age when such attachments are considered to be well
established (11-13). In such cases, EVT in the presence of connection
between dartos and external spermatic fascia remains unexplained by the
examined theory, raising doubts on its validity.
As regards gross appearance, given that
the outer membrane layers of the spermatic cord are very thin and transparent
it is almost impossible by observation alone to distinguish the exact
twisted layer of spermatic cord. In contrast, histological ischemic lessons
outside tunica vaginalis observed in the removed specimens after orchidectomy
has never, to our knowledge, been previously documented. Furthermore,
the fact that hemorrhagic fluid is always confronted within an outer membrane
layer, indicates that this layer (that is the external spermatic fascia
and probably inner layers too) remains intact and is not included in the
ischemic tissues (Figure-4).
Taking all the above factors into consideration,
in cases of perinatal EVT doubts on whether or not external spermatic
fascia is included in the twisted mass are reveled, while the mechanism
that describes an EVT outside cremaster muscle including all layers of
the spermatic cord remains to be defined.
Torsion
Inside Cremaster Muscle
The second theory to explain EVT is that
in the full-term infant, the spermatic cord and testis are free to rotate
within the inguinal canal and scrotum, due to lack of attachment between
the testicular tunica vaginalis and the scrotum. Most authors refer to
this theory (12,14-18) (Figure-4b). In matters of gross appearance, the
smooth membrane layer usually covering the twisted mass, sequestering
the underlying hemorrhagic fluid reinforce this theory, indicating that
torsion occurs in an inner rather than an external spermatic layer. However,
we have reasons to believe that this theory is based on a misinterpretation
of the definition “lack of fixation of tunica vaginalis to the scrotum”
as defined by Cooper (1830), which has been subsequently uncritically
copied by most authors (5). It has usually been referred to as, “due
to the recent descent of the gonad, there is an extreme mobility of tunica
vaginalis within the scrotum before fixation of tunica vaginalis to the
scrotal wall” (15,16), or “there is lack of firm attachment
of parietal layer of tunica vaginalis with the scrotum” (2). However,
literally, parietal layer of tunica vaginalis is never fixed to the scrotum,
but its outer associated membranes (cremaster muscle and fascias) will.
Therefore, inadequate fixation of tunica vaginalis to the scrotum is a
term incorrectly used for the description of the normal lack of connections
of the entire scrotal contents with the scrotal wall in the first days
of life, as described by Cooper (5).
Moreover, not only, perinatal lack of attachment
between testicular tunica vaginalis and its outer associated membranes
in the scrotum have never, in fact, been documented, but also there is
no obvious etiological reason to explain why such a lack should be present
in the first place. During embryogenesis, both the parietal layer of tunica
vaginalis (derivative of the peritoneum forming the parietal layer of
processus vaginalis) and the derived by the pars vaginalis gubernaculum
outer associated membranes (internal spermatic fascia, cremaster muscle
and external spermatic fascia) were never separate (19). This firm relationship
negates the possibility of a perinatal absence of such attachments (Figure-5).

On the contrary, even assuming an absence
of attachments between tunica vaginalis and internal spermatic fascia,
torsion outside tunica vaginalis could not possibly occur. Given that
in EVT testicular anatomy is considered to be normal (absence of bell
clapper deformity) in scrotal and inguinal region the testis, epididymis,
spermatic vessels and vas deference lie posteriorly connected with the
internal spermatic fascia through a wide mesentery (mesogonadal - mesorcheon)
and cannot move freely (20) (Figure-6).

These factors prove that, there is no embryological
basis to support a perinatal lack of tunica vaginalis attachments with
the internal spermatic fascia, while as in every scrotum with normal anatomy,
in cases of EVT, rotation inside cremaster muscle cannot occur (21).
COMMENTS
The validity of the anatomical basis of EVT has been previously questioned. Mushat (1932) in his work on mechanism of testicular torsion raised doubts on whether EVT was actually possible (21). Additional doubts on whether current anatomical interpretation is correct are derived from data suggesting the possibility of the existence of a bell clapper deformity in case of perinatal torsion. As stated above and demonstrated by our photographic data EVT is considered to be characterized by connection of testis with tunica vaginalis, in contrast with intravaginal torsion where posterior attachment of testis with tunica vaginalis is absent and scrotal structures demonstrate the bell clapper deformity. Investigation of contralateral testes in cases of vanishing testis syndrome, a condition representing the final effect of antenatal torsion revealed the presence of a contralateral bell clapper deformity in the remarkable percentage of 86% of cases (15,22-25). Given that bell clapper deformity is usually bilateral, existence in the ipsilateral, where antenatal torsion has occurred, of a bell clapper deformity as well before the vanishing event is very possible. Therefore, the question whether presence of connection between testis and tunica vaginalis in case of EVT represents normal anatomy or fibrotic connections of an underlying bell clapper deformity due to the chronic character of this antenatal event remains to be defined. This fact would reinforce the majority of authors, who support an EVT within dartos muscle, though under a different hypothesis than the one proven to be incorrect by our study.
CONCLUSION
In summary, the two most commonly accepted anatomical definitions of perinatal testicular torsion namely an extravaginal torsion within dartos muscle, including all layers of spermatic cord and an extravaginal torsion outside parietal layer of tunica vaginalis within internal spermatic fascia remain questionable. In the first case, although there is evidence of perinatal lack of attachments between external spermatic fascia and dartos muscle, such torsion has not been proved with certainty. On the contrary, a large body of literature argues against this explanation. In the second case, doubts on whether there is lack of attachments between testicular tunica vaginalis and scrotum have been revealed. Yet, even if such a lack was actually present, testicular torsion inside internal spermatic fascia would still be impossible, since genital apparatus remains fixed by its wide mesorchium to external membrane layers of the scrotum. Finally, suspicions regarding the existence of a bell clapper deformity in all cases of EVT were raised, a fact confronting the current understanding of the condition. It is concluded that the prevalent anatomical definitions of EVT fail to explain adequately the phenomenon of perinatal torsion and to allow an evidence based documentation of the indicated treatment modality. EVT still remains a condition of unknown etiology, pathophysiology and surgical anatomy and thus further investigation in the field is required.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Waldschmidt J: Hodentorsion. In: Waldschmidt J, Hamm B, Schier F (ed.), Das acute Skrotum. Stuttgard – Verlag, Hippokrates. 1990; pp. 27-48.
- Herman A, Schvimer M, Tovbin J, Sandbank J, Bukovski I, Strauss S: Antenatal sonographic diagnosis of testicular torsion.Ultrasound Obstet Gynecol. 2002; 20: 522-4.
- Whitaker RH: Diagnoses not to be missed. Torsion of the testis. Br J Hosp Med. 1982; 27: 66-9.
- Mishriki SF, Winkle DC, Frank JD: Fixation of a single testis: always, sometimes or never. Br J Urol. 1992; 69: 311-3.
- Cooper Sir Astley: Observations on the structure and disease of the testis. Longman, London, 1830.
- Jerkins GR, Noe HN, Hollabaugh RS, Allen RG: Spermatic cord torsion in the neonate. J Urol. 1983; 129: 121-2.
- Sheridan WG, Davies DG: Extravaginal testicular torsion. Br J Clin Pract. 1988; 42: 128-30.
- Kay R, Strong DW, Tank ES: Bilateral spermatic cord torsion in the neonate. J Urol. 1980; 123: 293.
- Junnila J, Lassen P: Testicular masses. Am Fam Physician. 1998; 57: 685-92.
- Noseworthy J: Testicular torsion. In: Ashcraft K.W (ed.), Pediatric Surgery 3rd ed. WB Saunders, Philadelphia, 200; 674-80.
- Das S, Singer A: Controversies of perinatal torsion of the spermatic cord: a review, survey and recommendations. J Urol. 1990; 143: 231-3.
- Barker K, Rapeer FP: Torsion of the testis. Br J Urol. 1964; 36: 35-41.
- Johnston JH: The testicles and the scrotum. In: DI Williams (ed.), Pediatric Urology. London, Q Butterworths. 1968; pp. 450-74.
- Sorensen MD, Galansky SH, Striegl AM, Koyle MA: Prenatal bilateral extravaginal testicular torsion--a case presentation. Pediatr Surg Int. 2004; 20: 892-3.
- Belman AB, Rushton HG: Is the vanished testis always a scrotal event? BJU Int. 2001; 87: 480-3.
- Al-Salem AH: Intra-uterine testicular torsion: early diagnosis and treatment. BJU Int. 1999; 83: 1023-5.
- Traubici J, Daneman A, Navarro O, Mohanta A, Garcia C: Original report. Testicular torsion in neonates and infants: sonographic features in 30 patients. AJR Am J Roentgenol. 2003; 180: 1143-5.
- Arena F, Nicotina PA, Scalfari G, Visalli C, Arena S, Zuccarello B, et al.: A case of bilateral prenatal testicular torsion: Ultrasonographic features, histopathological findings and management. J Pediatr Urol. 2005; 1: 369-72.
- Pham SB, Hong MK, Teague JA, Hutson JM: Is the testis intraperitoneal? Pediatr Surg Int. 2005; 21: 231-9.
- Hollinshead WH: The perineum. In: Hollinshead WH (ed.), Anatomy for Surgeons Vol 2. 2nd ed. New York, Harper and Row. 1971; pp. 853-68.
- Mushat M: The pathological anatomy of testicular torsion; explanation of its mechanism. Surgery, Gynecology and Obstetrics. 1932; 54: 758-63.
- Gong M, Geary ES, Shortliffe LM: Testicular torsion with contralateral vanishing testis. Urology. 1996; 48: 306-7.
- Belman AB, Rushton HG: Is an empty left hemiscrotum and hypertrophied right descended testis predictive of perinatal torsion? J Urol. 2003; 170: 1674-5; discussion 1675-6.
- Bellinger MF: The blind-ending vas: the fate of the contralateral testis. J Urol. 1985; 133: 644-5.
- Harris BH, Webb HW, Wilkinson AH Jr, Stevens PS: Protection of the solitary testis. J Pediatr Surg. 1982; 17: 950-2.
____________________
Accepted after revision:
July 7, 2008
_______________________
Correspondence address:
Dr. Iason D. Kyriazis
22 Xatzikonstanti St. Papagos
PC 15669, Athens, Greece
Fax: + 30 210 656-0220
E-mail: jkyriazis@gmail.com
EDITORIAL COMMENT
Most
cases of fetal and neonatal testicular torsion are diagnosed at birth
either by absence of the testis in the scrotum or inguinal region (vanishing
testis), or by the presence of a hard testis fixed to the scrotal skin.
These cases are thought to be caused by an extravaginal torsion of the
spermatic cord (EVT), due to inadequate attachments between the layers
of the spermatic cord, usually completed only after few weeks of life.
Despite prompt surgical exploration of the ischemic testes in the neonatal
period, their salvage rate is very low, and the real debate is if early
contralateral testicular fixation is warranted. Cases of testicular torsion
occurring later, in previously normal testes, are also caused by an intravaginal
torsion of the spermatic cord, by the bell-clapper deformity, that usually
is observed also in the contralateral testis (1). In these cases, since
the salvage rate of the affected testis rises to almost 50%, emergency
surgical exploration is always recommended, and must include the contralateral
testicular fixation (2).
The work by Dr Kyriazis and associates evaluates
the anatomical definitions of the perinatal EVT, based mainly on a thorough
review of the literature. The bibliographical survey is well performed,
and the authors elegantly discuss the two theories on the anatomical basis
of the EVT, the one occurring inside, and the other outside the cremaster
muscle. They also propose an evaluation of a photographic data from 14
previously operated cases. Unfortunately, although illustrative, this
evaluation is superficial and presented without scientific methodology.
Furthermore, they present no pathological data of their cases that could
give support to any of the two mentioned theories.
Although this work does not address the
issue of the management of EVT, I encourage the authors to review their
material and include more significant information of their cases, including
age of the patients, management of the contralateral testes and pathological
data, that would surely enrich the scarce literature on the subject.
REFERENCES
- Favorito LA, Cavalcante AG, Costa WS: Anatomic aspects of epididymis and tunica vaginalis in patients with testicular torsion. Int Braz J Urol. 2004; 30: 420-4.
- Sorensen MD, Galansky SH, Striegl AM, Mevorach R, Koyle MA: Perinatal extravaginal torsion of the testis in the first month of life is a salvageable event. Urology. 2003; 62: 132-4.
Dr.
Francisco Tibor Dénes
Section of Pediatric Urology
University of Sao Paulo, USP
Sao Paulo, SP, Brazil
E-mail: ftdenes@terra.com.br
EDITORIAL COMMENT
Testicular
torsion is divided into two types, intravaginal and extravaginal. Intrauterine
testicular torsion (IUTT) is of the extravaginal type. IUTT was first
described by Taylor in 1897 and when compared to intravaginal torsion,
it is a very rare condition that is being recognized with increasing frequency
(1). One reason for this is the adoption of routine thorough examination
of all newborns prior to their discharge. We however recommend that this
routine general examination be done in the immediate postpartum period
as well as prior to discharge. This will obviate any delay in diagnosis
and treatment of IUTT since the majority of them will manifest in the
immediate postpartum period (2). IUTT is a very rare condition that may
also be difficult to recognize when seen for the first time and so it
may be missed or confused with other conditions. To obviate delay in diagnosis,
physicians caring for these patients should be aware of this.
Since its first description, controversies
continue to exist regarding: (1) its exact cause, (2) the need for urgent
exploration and (3) the necessity for contra lateral orchidopexy.
The cause as well as the anatomical basis
of IUTT is not known. In this issue, Kyriazis et al. in an extensive review
attempted to evaluate the anatomical basis of intrauterine torsion. Although
IUTT is usually a prenatal event, the exact timing and duration of torsion
are not known and there are reports of prenatally diagnosed torsion. Tripp
and Homsy reported a case of bilateral torsion diagnosed prenatally at
35 weeks gestation and Hubbard et al. reported a case of unilateral torsion
diagnosed at 35.5 week gestation (3,4). On the other hand, and although
most cases of IUTT are apparent at birth, there are reports of torsion
occurring after delivery or within the first week after birth (5). It
is believed that IUTT is the main cause of monorchidism, which is supported
by the fact that a vas deference, epididymis, calcification or hemosiderine
pigmentation is present in about 90% of the cases (6). In cases of IUTT,
controversy still continues regarding the urgency for surgical exploration
as well as the need for contra lateral orchidopexy. Some investigators
advocate delayed operation, and consider this not an emergency (7). This
is to obviate the anesthetic risk imposed on the neonate as well as the
low salvage rate of these testes. If such a policy is adopted, then these
patients should not be operated on at all as ultimately the affected testis
will atrophy. On the contrary, these patients are healthy, of good birth
weight and without any other associated anomalies that impose an anesthetic
risk (2). Keeping this in mind as well as the hope of testicular preservation,
we like others adopted a policy of early surgical intervention (2,8).
Olguner et al. reported a patient at the postnatal 28th hour with right
scrotal erythema and swelling. Emergency technetium Tc 99m pertechnetate
scintingraphy showed hypo perfusion in both sides and because the patient
underwent surgery immediately, the left testis was judged viable, treated
by means of detorsion and saved while the right testis was necrotic (8).
Early surgical exploration also establishes the diagnosis and excludes
other rare causes such as benign and malignant tumors and traumatic hematocele.
Another controversial point is whether contra
lateral orchidopexy is justified. Some investigators suggested that since
predisposing factors are lacking in extravaginal torsion, there is no
need for contra lateral orchidopexy (6). This however is difficult to
establish. On the other hand, the increasing number of reported cases
with bilateral intrauterine torsion supports a predisposing factor (3,8-10),
and although asynchronous bilateral torsion is rare, it can however occur
at any time and has been reported as early as 48 hours after torsion on
the other side (10). To obviate the risk of anorchia, we like others advocate
routine and simultaneous contra lateral exploration and orchidopexy. This
is a simple procedure, has no or minimal morbidity and safeguards against
contra lateral torsion.
REFERENCES
- Taylor MR: A case of testicular strangulation at birth, castration, recovery. Br Med J. 1897; 1: 458.
- Al-Salem AH: Intrauterine testicular torsion: a surgical emergency. J Pediatr Surg. 2007; 42: 1887-91.
- Tripp BM, Homsy YL: Prenatal diagnosis of bilateral neonatal torsion: a case report. J Urol. 1995; 153: 1990-1.
- Hubbard AE, Ayers AB, MacDonald LM, James CE: In utero torsion of the testis: antenatal and postnatal ultrasonic appearances. Br J Radiol. 1984; 57: 644-6.
- Burge DM: Neonatal testicular torsion and infarction: aetiology and management. Br J Urol. 1987; 59: 70-3.
- Lamesch AJ: Monorchidism or unilateral anorchidism. Langenbecks Arch Chir. 1994; 379: 105-8.
- Cumming DC, Hyndman CW, Deacon JS: Intrauterine testicular torsion: not an emergency. Urology. 1979; 14: 603-4.
- Olguner M, Akgür FM, Aktuð T, Derebek E: Bilateral asynchronous perinatal testicular torsion: a case report. J Pediatr Surg. 2000; 35: 1348-9.
- Weingarten JL, Garofalo FA, Cromie WJ: Bilateral synchronous neonatal torsion of spermatic cord. Urology. 1990; 35: 135-6.
- LaQuaglia MP, Bauer SB, Eraklis A, Feins N, Mandell J: Bilateral neonatal torsion. J Urol. 1987; 138: 1051-4.
Dr.
Ahmed H. Al-Salem
Consultant Pediatric Surgeon
Maternity ad Children Hospital
Dammam, Saudi Arabia
E-mail: ahalsalem@hotmail.com
EDITORIAL COMMENT
The
authors challenge established anatomical and pathological principles of
“extravaginal” testicular torsion through a discussion on
the clinical findings, a literature review and a focused anatomical discussion.
The importance of this discussion lies within the implications for clinical
management in this group. The debate within pediatric surgical literature
between the active exploration of the perinatal torsion and its conservative
management is firmly grounded in the surgical precepts that intra and
extra vaginal torsions are separate anatomical and surgical anomalies.
The
paper debunks the accepted theories of extravaginal torsion. The authors
argue that the simple lack of perinatal attachments which is the clinical
norm in the first seven to ten days does not equate to the relative infrequency
of the condition. The absence of a clear definition of extravaginal torsion
and the specter of presence of bell clapper deformity leads to a requirement
for a much more aggressive surgical management of this condition.
Despite
the relative infrequency of the asynchronous torsion in the literature
as pediatric urologists we all seem to have one or more of these patients
in our own units leading to real concerns of under reporting (1). A significant
body of opinion argues against conservative management due to incidence
of asynchronous events (2-4). Baglaj et al. identified 48 cases of bilateral
perinatal torsions in the literature (5). Synchronous torsion occurred
in 67% thus asynchronous torsion occurred in 33%. Urgent exploration of
the torted testis and empiric exploration and orchidopexy for the contralateral
testis is recommended in all cases of perinatal torsion. Parental counseling
which explains the relatively low salvage rate and the high asynchronous
torsion rate is warranted.
The
challenge for pediatric surgeons is to examine all the excised perinatal
testicles that in order to delineate the pathology. Further anatomical
studies are required on the scrotal anatomy of neonates with fully descended
testes who die in the perinatal period in order to define the normal anatomical
attachments of the testes.
REFERENCES
- Beasley SW, McBride CA. The risk of metachronus (asynchronous) contralateral torsion following perinatal torsion. N Z Med J. 2005; 118: U1575.
- Cuervo JL, Grillo A, Vecchiarelli C, Osio C, Prudent L: Perinatal testicular torsion: a unique strategy. J Pediatr Surg. 2007; 42: 699-703.
- Yerkes EB, Robertson FM, Gitlin J, Kaefer M, Cain MP, Rink RC: Management of perinatal torsion: today, tomorrow or never? J Urol. 2005; 174: 1579-82; discussion 1582-3.
- Sorensen MD, Galansky SH, Striegl AM, Mevorach R, Koyle MA: Perinatal extravaginal torsion of the testis in the first month of life is a salvageable event. Urology. 2003; 62: 132-4.
- Baglaj M, Carachi R: Neonatal bilateral testicular torsion: a plea for emergency exploration. J Urol. 2007; 177: 2296-9.
Dr. Feilim Murphy
Consultant Paediatric Urologist
Department of Paediatric Surgery and Urology
St George’s Hospital,
London, United Kingdom
E mail: feilimmurphy@ireland.com