PHEOCHROMOCYTOMA:
A LONG-TERM FOLLOW-UP OF 24 PATIENTS UNDERGOING LAPAROSCOPIC ADRENALECTOMY
(
Download pdf )
LÍSIAS N. CASTILHO, FABIANO A. SIMOES, ANDRE M. SANTOS, TIAGO M. RODRIGUES, CARLOS A. DOS SANTOS JUNIOR
Section of Urology, Catholic University of Campinas, Campinas, Sao Paulo, Brazil
ABSTRACT
Purpose:
Pheochromocytomas are tumors derived from chromaffin cells that often
secrete catecholamines and cause hypertension. The clinical diagnosis
of pheochromocytoma depends on the presence of excessive production of
catecholamines. Conventional imaging modalities that have been used in
the preoperative evaluation include CT, MRI, and 131I-MIBG scintigraphy.
Surgical resection is the definitive treatment for patients with pheochromocytoma.
The goal of this study was to evaluate the long-term follow-up of 24 patients
undergoing laparoscopic adrenalectomy for pheochromocytoma.
Materials and Methods: From January 1995
to September 2006, 24 patients underwent laparoscopic adrenalectomy for
adrenal pheochromocytoma. Twenty (83.3%) patients had arterial hypertension.
The inclusion criteria of patients in this retrospective study were laparoscopic
approach, unilateral or bilateral adrenal tumor, pathological diagnosis
of pheochromocytoma and a minimum follow-up of 18 months.
Results: Intra-operative complications occurred
in 4 (16.7%) patients. Two (8.3%) patients had postoperative complications.
Two patients (8.3%) had blood transfusion. The mean postoperative hospital
stay was 3.8 days (range 1 to 11). Eighteen (90%) of the twenty patients
who had symptomatic hypertension, returned to normal blood pressure immediately
after surgery, during the hospital stay. In one patient, the high blood
pressure levels remained unchanged. Another patient persisted with mild
hypertension, well controlled by a single antihypertensive drug.
Conclusions: Our results confirmed that
laparoscopic adrenalectomy for pheochromocytoma is a safe and effective
procedure, providing the benefits of a minimally invasive approach. In
our study, the initial positive results obtained in the treatment of 24
patients were confirmed after a mean follow-up of 74 months.
Key
words: laparoscopy; pheochromocytoma; adrenalectomy
Int Braz J Urol. 2009; 35: 24-35
INTRODUCTION
Pheochromocytomas
(PCCs) are tumors derived from chromaffin cells that produce and often
secrete catecholamines. Over 90% of PCCs are in the abdomen, most frequently
in the chromaffin cells of the adrenal medulla. Approximately 10% are
found in extra-adrenal sites where they are called paragangliomas due
to their association with sympathetic nervous system ganglia in the chest,
abdomen, or pelvis (1).
The estimated incidence ranges from 0.005%
to 0.1% of the general population and from 0.1% to 0.2% of the adult hypertensive
population. The highest incidence occurs during the fourth and fifth decades
of life, and is nearly identical in both sexes (1).
Approximately 10% of pheochromocytomas are
hereditary. Hereditary tumors are frequently multiple or bilateral and
rarely malignant. Familial syndromes associated with PCCs include multiple
endocrine neoplasia type 2 (MEN 2), von Hippel-Lindau disease (VHL), and
the neuroectodermal dysplasias consisting of neurofibromatosis, tuberous
sclerosis, and Sturge-Weber syndrome (2). Approximately 10 to 15% of pheochromocytomas
exhibit malignant behavior. In order to diagnose malignant PCCs, one must
document invasion of adjacent organs or metastatic disease. The most frequent
sites of metastases are the liver, lung, and bone, particularly the spine,
skull, and ribs. There is no absolute clinical, imaging, or laboratory
criteria to predict malignancy; however, patients with malignant disease
tend to have larger tumors and higher urinary metanephrine levels (2).
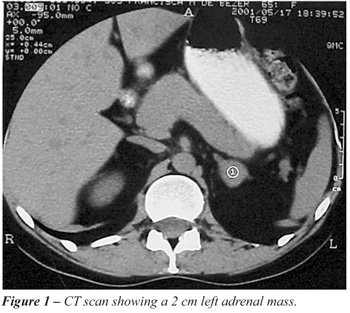
Conventional imaging modalities that have
been used in the preoperative evaluation of patients with a biochemically
confirmed pheochromocytoma include CT, MRI, and Iodine-131-metaiodobenzylguanidine
(131 I-MIBG) scintigraphy. CT easily detects tumors of 1 cm or more with
high sensitivity, which varies between 93% and 100% for adrenal gland
tumor detection and approximately 90% for extra-adrenal disease identification
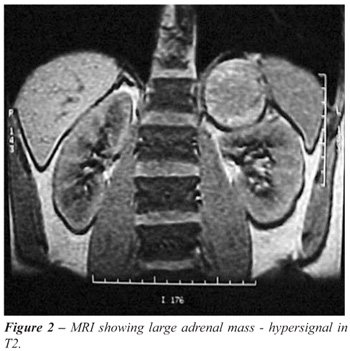
(Figure-1). MRI is also sensitive. Characterization of adrenal masses
is done with chemical shift MRI based on the absence of fat in PCCs. In
addition, the hypervascularity of pheochromocytomas makes them appear
characteristically bright, with a high signal on T2-weighted images (Figure-2).
131I-MIBG scanning works by administering a radiolabeled amine for which
chromaffin tissue is selectively avid. Since it is a physiologic study,
MIBG can identify pheochromocytomas regardless of their location. This
modality may be useful in patients with biochemical evidence of a pheochromocytoma
that has not been localized by CT or MRI or in the follow-up evaluation
of patients with suspected or documented recurrent or metastatic disease
(2).
Surgical resection is the definitive treatment
for patients with pheochromocytoma. Prior to the surgery, the patient
must be adequately prepared with alpha-adrenergic blockade and complete
restoration of fluid and electrolyte balance. Alpha-blockade works to
oppose catecholamine-induced vasoconstriction and sometimes must be associated
with the beta-adrenergic blockade with propranolol and expanding volume
(3).
Pheochromocytoma was initially considered
a contraindication to laparoscopic approach due to the fear of hypertensive
crisis associated with the pneumoperitoneum. However, an increasing series
of laparoscopy using the transperitoneal or retroperitoneal approach have
been reported and proved to be a safe procedure with similar blood loss
and no difference in blood pressure or heart rate increments when compared
with open adrenalectomy (3). Patients also experience faster resolution
of postoperative ileum, decreased analgesic requirements, a shorter length
of hospital stay, and a shorter convalescence with a more rapid return
to normal activity (3-5).
The goal of this study was to evaluate the long-term results of 24 patients
undergoing laparoscopic adrenalectomy for pheochromocytoma.
MATERIALS AND METHODS
From
January 1995 to September 2006, we retrospectively reviewed the results
of transperitoneal laparoscopic adrenalectomy performed in 24 patients
with pheochromocytoma. This series consisted of 14 (58.3%) males and 10
(41.7%) females, with the mean age of 46 years (range 10 to 75 years,
median 46.5).
The Body Mass Index (BMI) ranged from 19.4
to 33.5. Nine (37.5%) cases presented with overweight (BMI between 25
and 30) and one (4.2%) case with obesity (BMI 33.5).
Twenty (83.3%) of the twenty-four patients
had arterial hypertension, half of them with severe hypertensive crisis
and the other 10 patients with mild to moderate hypertension. The mean
time between installation of hypertension and the diagnosis of pheochromocytoma
was 3 years (3 months to 8 years). Four (16.7%) patients had normal blood
pressure levels. Three were completely asymptomatic (incidental findings)
and 1 had abdominal pain and recurrent anxiety crises.
The mean tumor size estimated by CT scan
was 3.9 cm (1 to 12 cm, median 3.7 cm). In 14 (58.3%) patients the tumors
were on the right side, 9 (37.5%) on the left, and only 1 (4.2%) was bilateral
(Table-1).

The inclusion criteria of patients in this
retrospective study were laparoscopic approach, unilateral or bilateral
adrenal tumor, pathological diagnosis of pheochromocytoma and a minimum
follow-up of 18 months.
The preoperative diagnosis of pheochromocytoma
in the symptomatic patients was confirmed by the clinical presentation
and the biochemical and radiographic findings. The vanylmandelic acid
level of a 24-hour urine sample and plasma norepinephrine and epinephrine
levels were routinely tested before surgery and every six months after
surgery. Abdominal CT scans were obtained in all cases, both in pre-operative
as in the post-operative annually. 131I-MIBG was performed in 21 patients,
20 cases with clinical and laboratory suspicion of pheochromocytoma and
one case without any suspicion that presented an incidental finding. In
all cases MIBG were repeated annually after surgery. MRI was performed
in 7 patients in the pre-operative evaluation because of iodine allergy
or inconclusive CT images.
Patients with hypertension and/or abnormally
high catecholamine levels were given prazosin 2 to 20 mg/day during 14
to 21 days before surgery. In order to expand the blood volume, patients
were infused with crystal liquids (2 to 3 liters) just prior to surgical
intervention. All patients underwent general endotracheal anesthesia.
The mean arterial pressure, central venous pressure, and vital signs were
monitored during surgery. Sodium nitroprusside was administered to control
the blood pressure when needed. Intraoperative hemodynamic changes resulting
from the pneumoperitoneum and intraoperative manipulations were documented.
The surgical technique of transperitoneal
laparoscopic adrenalectomy has been extensively described (2,5).
The follow-up of patients was done based
on data review from medical records and telephone contacts. During the
first year of follow-up, each patient was examined in at least four different
occasions. Their blood pressure was measured and registered in their records.
In the sixth and tenth months following the surgery, each patient was
submitted to dosage of cathecholamines in urine and serum. They were submitted
to MIBG at the end of the first year after surgery. After the first year,
each patient was examined at least once a year and submitted to laboratory
exams and MIBG for at least five years. All the cases included in the
study had a minimum follow-up of 18 months (18 to 150 months, mean 74
months).
RESULTS
We
successfully performed twenty-five laparoscopic adrenalectomies in twenty-four
different patients. Twenty-three patients underwent unilateral LA and
one patient underwent right total and left partial adrenalectomy for bilateral
pheochromocytoma. This case was operated in two stages. Of the 25 interventions,
2 (8%) were converted to open surgery, one due to a major venous bleeding
and the other due to difficulty in freeing the gland, located almost entirely
behind the inferior vena cava.
The mean operative time, excluding the two
converted cases, was 126 minutes (60 to 215 min.).
Intra-operative complications occurred in
4 (16.7%) patients (Table-2).
In one case, during specimen withdrawal,
the extractor bag ruptured and the specimen was not found by laparoscopic
inspection. It was necessary to make a small incision in the abdomen to
remove the gland. In another case, we had a small vena cava injury that
was sutured by laparoscopy without any difficulty. A 10-year-old patient
suffered an injury in anomalous right adrenal vein. The subsequent bleeding
required conversion to open surgery. The oldest patient in this series,
a 75-year-old woman with a 12 cm left adrenal tumor, there was an injury
of the splenic artery during dissection. The arterial injury could not
be repaired and a laparoscopic splenectomy was performed.
No cases of severe hemodynamic instability
were observed throughout the duration of anesthesia, but most of the patients
had transient elevation of blood pressure during the manipulation of the
gland, before adrenal vein ligation. These elevations were in general
controlled with sodium nitroprusside.
Two (8.3%) patients had postoperative complications
(Table-2). In one of the converted procedures, the patient developed an
acute renal failure, postoperative ileum and subcutaneous infection. He
left the hospital in a good condition on the 7th postoperative
day. Another patient developed an abdominal and lumbar ecchymosis after
hospital discharge with spontaneous resolution.
Two patients (8.3%) received a blood transfusion
(Table-2), one of them in the operating room and the other during the
first postoperative day.
All patients resumed oral nutrition and
ambulation 1 to 2 days after the surgery.
The mean postoperative hospital stay was
3.8 days (1 to 11 days).
All the tumors were pathologically identified
as pheochromocytomas. There was no evidence of malignancy such as local
invasion or metastasis. The largest specimen removed measured 12 cm and
weighed 200g (case 23).
Of the twenty patients who had symptomatic
hypertension, 18 (90%) returned to normal blood pressure immediately after
the surgery, during the hospital stay. In one of the patients the blood
pressure level remained unchanged (hypertensive crises). Another patient
persisted with mild hypertension, controlled with a single antihypertensive
drug. These results remained unchanged during the follow-up.
In one of four normotensive patients, the
blood pressure had a peak during the anesthetic induction but was easily
controlled with sodium nitroprusside. Another normotensive patient complained
of abdominal pain and anxiety. His symptoms disappeared after surgery
(case 14). All these 4 cases remained normotensive in the late postoperative
period (Table-3).
During a mean follow-up of 74 months, no
tumor recurrence or metastasis was observed.
One patient died 18 months after surgery
because of myocardial infarction. This patient underwent bilateral surgery,
with right total and left partial adrenalectomy. He became normotensive
and the postoperative adrenal function remained normal, without the use
of glucocorticoids or mineralocorticoids (case 15).
COMMENTS
Since
the first report of laparoscopic adrenalectomy by Gagner et al. in 1992,
this procedure has become the preferred surgical management of benign
adrenal tumors due to its numerous advantages (6). Comparative studies
between open and laparoscopic surgery have shown that laparoscopic intervention
should be considered the gold-standard procedure for adrenal surgery (7,8).
To date no relevant prospective and randomized
series comparing laparoscopic adrenalectomy versus conventional surgery
for pheochromocytoma, to our knowledge, has been published in the literature.
Nevertheless, the accumulated international experience is significant
and suggests that laparoscopic approach is better than open surgery regarding
morbidity, bleeding, length of hospitalization, convalescence, postoperative
pain and aesthetic sequels (7-9).
Pheochromocytoma was initially considered
a contraindication to LA because it was reported by Meurisse et al. that
pneumoperitoneum could promote an acute release of catecholamines (10).
However, several authors have shown that when there is an adequate preoperative
preparation these changes are discrete and well-tolerated by patients
(11-13).
In a recent study, Sood et al. showed that
the maintenance of a lower intraabdominal pressure (8-10 mmHg) reduces
the release of catecholamines and helps prevent hemodynamic instability
(14).
There are four possible laparoscopic approaches
to the adrenal gland, mainly transperitoneal, lateral retroperitoneal,
posterior retroperitoneal and trans-thoracic trans-diaphragmatic (15,16).
The transperitoneal access is often preferred by many surgeons because
of its broader working space and familiar anatomy. Nonetheless, retroperitoneal
laparoscopic adrenalectomy has gained popularity because it provides direct
access to the adrenal gland and avoids bowel handling and potential intraaabdominal
viscera injury. Rubinstein et al. published a randomized trial with 56
patients at the Cleveland Clinic, showing that operative parameters, perioperative
morbidity and pathological characteristics of the intact extracted specimen
were similar between both approaches (17). The choice of laparoscopic
approach for adrenalectomy varies according to personal experience and
preference of the laparoscopic surgeon.
In our experience, the small incidence of
complications, the short convalescence period and the long-term satisfactory
results, have enabled us to establish the laparoscopic adrenalectomy as
the procedure of choice in pheochromocytoma management.
With the introduction of robotic surgery,
adrenalectomy using robotic endoscopic surgical devices (Da Vinci system)
has recently been proposed. Morino et al., published a prospective randomized
trial with 20 patients, comparing the outcomes of robotic (RA) versus
lateral transperitoneal laparoscopic procedures. This study showed that
RA is associated with a longer operative time, increased cost and a higher
morbidity when compared to lateral transperitoneal LA (18). However, further
studies are needed to define the role of robotic-assisted adrenalectomy
(19).
Perioperative management of patients with
phaeochromocytoma requires detailed knowledge of the potential complications.
Intraoperatively, hypertensive crisis and tachyarrhythmia may occur resulting
from massive catecholamine release. Thus, in agreement with other authors
we consider preoperative treatment with the alpha-antagonist phenoxybenzamine
obligatory (20).
Most research published on laparoscopic
adrenalectomy refer to tumors smaller than 6 cm without pre-operative
characteristics suggesting malignancy. Despite some reports of surgeries
performed in large tumors with identified malignancy potential in pre-operative
assessment, these procedures should be left to academic centers with extensive
experience in laparoscopic surgery of the adrenal gland.
CONCLUSIONS
Our results have confirmed that laparoscopic adrenalectomy for pheochromocytoma is a safe and effective procedure, providing the benefits of a minimally invasive approach. In our experience, the initial positive results obtained in the treatment of 24 patients were confirmed after a median follow-up of 74 months.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Karagiannis A, Mikhailidis DP, Athyros VG, Harsoulis F: Pheochromocytoma: an update on genetics and management. Endocr Relat Cancer. 2007; 14: 935-56.
- Mittendorf EA, Evans DB, Lee JE, Perrier ND: Pheochromocytoma: advances in genetics, diagnosis, localization, and treatment. Hematol Oncol Clin North Am. 2007; 21: 509-25.
- Castilho LN, Medeiros PJ: O tratamento laparoscópico do feocromocitoma. Rev Cienc Med. 2003; 12:63-7.
- Kasturi S, Kutikov A, Guzzo TJ, Smith AL, Wein AJ: Modern management of pheochromocytoma. Nat Clin Pract Urol. 2007; 4: 630-3.
- Castilho LN: Suprarrenalectomia. In: Castilho LN (ed.), Laparoscopia Urológica. Campinas, LPC Comunicações. 2000; pp. 365-77.
- Gagner M, Lacroix A, Bolté E: Laparoscopic adrenalectomy in Cushing’s syndrome and pheochromocytoma. N Engl J Med. 1992; 327: 1033.
- Castilho LN, Liang LS, Ferreira U, Fregonesi A, Saade RD, Netto Jr,NR: Cirurgia do tumor benigno de supra-renal por videolaparoscopia. J Bras Urol. 1996; 22:33-6.
- Castilho LN, Medeiros PJ, Mitre AI, Dénes FT, Lucon AM, Arap S: Pheochromocytoma treated by laparoscopic surgery. Rev Hosp Clin Fac Med Sao Paulo. 2000; 55: 93-100.
- Janetschek G, Altarac S, Finkenstedt G, Gasser R, Bartsch G: Technique and results of laparoscopic adrenalectomy. Eur Urol. 1996; 30: 475-9.
- Meurisse M, Joris J, Hamoir E, Hubert B, Charlier C: Laparoscopic removal of pheochromocytoma. Why? When? and Who? (reflections on one case report). Surg Endosc. 1995; 9: 431-6.
- Fernández-Cruz L, Sáenz A, Taurá P, Sabater L, Astudillo E, Fontanals J: Helium and carbon dioxide pneumoperitoneum in patients with pheochromocytoma undergoing laparoscopic adrenalectomy. World J Surg. 1998; 22: 1250-5.
- Chigot JP, Movschin M, el Bardissi M, Fercocq O, Paraskevas A: Comparative study between laparoscopic and conventional adrenalectomy for pheochromocytomas. Ann Chir. 1998; 52: 346-9.
- Col V, de Cannière L, Collard E, Michel L, Donckier J: Laparoscopic adrenalectomy for phaeochromocytoma: endocrinological and surgical aspects of a new therapeutic approach. Clin Endocrinol (Oxf). 1999; 50: 121-5.
- Sood J, Jayaraman L, Kumra VP, Chowbey PK: Laparoscopic approach to pheochromocytoma: is a lower intraabdominal pressure helpful? Anesth Analg. 2006; 102: 637-41.
- Gill IS: Laparoscopic Adrenal Surgery. In: 95th Annual Meeting, Atlanta; 2000. Laparoscopic Organ Ablative Urology – Postgraduate Course. Houston: AUA Office of Education; 2000. p.1-4.
- Subramaniam R, Pandit B, Sadhasivam S, Sridevi KB, Kaul HL: Retroperitoneoscopic excision of phaeochromocytoma--haemodynamic events, complications and outcome. Anaesth Intensive Care. 2000; 28: 49-53.
- Rubinstein M, Gill IS, Aron M, Kilciler M, Meraney AM, Finelli A, et al.: Prospective, randomized comparison of transperitoneal versus retroperitoneal laparoscopic adrenalectomy. J Urol. 2005; 174: 442-5; discussion 445.
- Morino M, Benincà G, Giraudo G, Del Genio GM, Rebecchi F, Garrone C: Robot-assisted vs laparoscopic adrenalectomy: a prospective randomized controlled trial. Surg Endosc. 2004; 18: 1742-6.
- Brunaud L, Bresler L, Ayav A, Zarnegar R, Raphoz AL, Levan T, et al.: Robotic-assisted adrenalectomy: what advantages compared to lateral transperitoneal laparoscopic adrenalectomy? Am J Surg. 2008; 195: 433-8.
- Knüttgen D, Wappler F: Anaesthesia for patients with phaeochromocytoma - specifics, potential complications and drug strategies. Anasthesiol Intensivmed Notfallmed Schmerzther. 2008; 43: 20-7.
____________________
Accepted after revision:
September 1, 2008
_______________________
Correspondence
address:
Dr. Lísias Nogueira Castilho
Av. Princesa D’Oeste, 1144 / 171
Campinas, SP, 13100-040, Brazil
E-mail: lisias@dglnet.com.br
EDITORIAL COMMENT
Surgical
cure of pheochromocytomas is a real challenge and must be considered a
model when multidisciplinary approach is essential to achieve the best
results. The endocrinologist, cardiologist, the anesthesiologist as well
as the surgeon must work together to avoid the devastating effects of
non programmatic surgical approach that in the past had high mortality
(1).
Pheochromocytomas often secrete catecholamine
that causes vasoconstriction and hypertension as the main symptom. The
complications of the adequate treatment are mild, and mortality is more
related to the patient’s condition than to the surgical technique
(2).
The variations on the blood pressure are
the biggest problem during the anesthetic procedure. Endocrine and cardiologic
preparations before the operation are the first steps to reduce complications.
Alpha-blocking agents in the pre operative period are obligatory in the
majority of patients for at least 15 days before the procedure. Beta blocking
can be associated in cases of excessive tachycardia or arrhythmias. Fluid
intake prior to the procedure is also mandatory (3). Echocardiogram defines
selected patients with excessive compromises of left ventriculum when
cardio tonics can show some benefits (4). After surgical resection, hypotension
or left ventriculum failure may occur and vasopressors must be infused
(3). Particularly when considering cure of hypertension after surgery,
cardiac failure can be considered a confounding factor for the immediate
evaluation.
As regards the surgical technique, in the
past ten years laparoscopic surgery has become the gold standard for tumors
smaller than 6 cm (5). At the beginning of the laparoscopic experience,
it has been thought that pneumoperitoneum could affect the blood pressure
during surgery (6).
Some contemporary reports have shown that
the variation in blood pressure occurred independently conventional surgery
or laparoscopic approach (7,8). Additionally, some authors have defended
that beyond the vantages of lower bleeding and faster recovery, the delicate
manipulation on laparoscopic technique would be an additional for minimum
invasive procedure (8-11).
Into pheochromocytoma surgery, it is important
to have an early stage control of the main adrenal vein with the intention
of reducing the blood pressure decompensation, yet it has been a questionable
paradigm these days (9). Some studies have proposed that the early control
of the vein could be done only via the transperitoneal technique, Salomon
et al. described the feasibility of doing this through extra peritoneal
approach (10).
In our experience the control of the vein
is not only bilateral feasibly but seems easier on the right side (where
the adrenal vein is shorter and frequently retrocaval), than through transperitoneal
approach, specially, when it is a large tumor (11).
Another important issue is the treatment
of the malignant disease that occurs in approximately 10 % (12). Some
initial series suggest that it is possible to offer laparoscopic treatment
with good results, but there are some cases of tumor recurrence and portal
implants (13).
The benefit of the laparoscopic procedure
in the case of malignant pheochromocytoma at a locally confined stage
still remains unclear and requires prospective, randomized studies.
REFERENCES
- Gagner M, Pomp A, Heniford BT, Pharand D, Lacroix A: Laparoscopic adrenalectomy: lessons learned from 100 consecutive procedures. Ann Surg. 1997; 226: 238-46; discussion 246-7.
- Gil-Cárdenas A, Cordón C, Gamino R, Rull JA, Gómez-Pérez F, Pantoja JP, et al.: Laparoscopic adrenalectomy: lessons learned from an initial series of 100 patients. Surg Endosc. 2008; 22: 991-4.
- Adams HA, Hempelmann G: Anesthesia for patients with pheochromocytoma. Our own results and a review. Anasthesiol Intensivmed Notfallmed Schmerzther. 1993; 28: 500-9.
- Meune C, Bertherat J, Dousset B, Jude N, Bertagna X, Duboc D, et al.: Reduced myocardial contractility assessed by tissue Doppler echocardiography is associated with increased risk during adrenal surgery of patients with pheochromocytoma: report of a preliminary study. J Am Soc Echocardiogr. 2006; 19: 1466-70.
- Guazzoni G, Cestari A, Montorsi F, Bellinzoni P, Centemero A, Naspro R, et al.: Laparoscopic treatment of adrenal diseases: 10 years on. BJU Int. 2004; 93: 221-7.
- Mittendorf EA, Evans DB, Lee JE, Perrier ND: Pheochromocytoma: advances in genetics, diagnosis, localization, and treatment. Hematol Oncol Clin North Am. 2007; 21: 509-25.
- Pugliese R, Boniardi M, Sansonna F, Maggioni D, De Carli S, Costanzi A, et al.: Outcomes of laparoscopic adrenalectomy. Clinical experience with 68 patients. Surg Oncol. 2008; 17: 49-57.
- Tobias-Machado M, Rincón Ríos F, Tulio Lasmar M, Tristão R, Hermínio Forseto P Jr, Vaz Juliano R, et al.: Laparoscopic retroperitoneal adrenalectomy as a minimally invasive option for the treatment of adrenal tumors. Arch Esp Urol. 2006; 59: 49-54.
- Lang B, Fu B, OuYang JZ, Wang BJ, Zhang GX, Xu K, et al.: Retrospective comparison of retroperitoneoscopic versus open adrenalectomy for pheochromocytoma. J Urol. 2008; 179: 57-60; discussion 60.
- Salomon L, Rabii R, Soulie M, Mouly P, Hoznek A, Cicco A, et al.: Experience with retroperitoneal laparoscopic adrenalectomy for pheochromocytoma. J Urol. 2001; 165: 1871-4.
- Tobias-Machado M, Lasmar MT, Zambon JP, Tristão R, Forseto PH Jr, Juliano RV, et al.: Laparoscopic adrenalectomy: a prospective study comparing transperitoneal and retroperitoneal approaches. Rev Assoc Med Bras. 2006; 52: 208-13.
- Strong VE, Kennedy T, Al-Ahmadie H, Tang L, Coleman J, Fong Y, et al.: Prognostic indicators of malignancy in adrenal pheochromocytomas: clinical, histopathologic, and cell cycle/apoptosis gene expression analysis. Surgery. 2008; 143: 759-68.
- Tobias-Machado M, Tristão RA, Silva MNR, Wroclawski ER: Laparoscopic adrenalectomy for malignant disease: Technical feasibility and oncological results. Einstein. 2007; 5: 44-47.
Dr.
Marcos Tobias-Machado &
Dr. Maria Claudia Bicudo
Section of Urology
ABC Medical School
São Paulo, SP, Brazil
E-mail: tobias-machado@uol.com.br
EDITORIAL COMMENT
The
surgical management of patients with pheochromocytoma is potentially curative
and it has always been a question of debate because of the clinical complexity
of such patients with potential high-risk peri-operative morbid-mortality.
When laparoscopic surgery was introduced
as an alternative approach for open surgery the tension rose among traditional
surgeons, used to the common problems associated with patients with pheochromocytoma,
that were mainly concerned with the safety of the laparoscopic approach.
As the experience among laparoscopists grew,
it became clear that this approach was not only a matter of better cosmesis,
whereas on the contrary, several reports revealed the benefits of treating
patients with pheochromocytoma preferentially via laparoscopy over the
conventional open approach, such as less cathecolamines release (1), less
bleeding (1,2), less UCI length of stay (2), less hospital stay (1,2),
shorter convalescence (1) and mainly revealing to be as safe as open surgery
(1,2).
Castilho and colleagues, in this issue of
the Int Braz J Urol reported on the long-term follow-up of 24 patients
who underwent laparoscopic adrenalectomy for pheochromocytoma over an
11-year period with a mean follow up of 74 months. Castilho’s study
found that only one patient was not totally cured in the period studied
(1 out of 24 - 4.2%); this single patient continued to have an hypertensive
crisis and another patient continued with mild hypertension under control.
No tumor recurrence was observed. The Castilho et al. report is very important
to demonstrate the long-term safety of laparoscopic approach as a means
of cure and tumor recurrence, in addition to the safety also reported
during the peri-operative time.
Treatment of patients with pheochromocytoma
requires a committed multidisciplinary team of urologist, endocrinologist,
anesthesiologist, radiologist and all staff in a well equipped hospital
and aware of all potential needs of such patients. Laparoscopic surgery
performed by an experienced surgical group along a knowledgeable committed
multidisciplinary team in a prepared hospital have proven efficacy and
safety. It should be kept in mind that laparoscopy is only one of the
advances now applied to patients with pheochromocytoma.
Nevertheless, laparoscopic surgery may not
yet have eliminated open surgery. At our institution, 4 patients with
pheochromocytoma out of 51 (8%) that were operated on from 2000 to 2008
(non-published data) still required open conventional approach either
because of major vessel involvement or tumor size greater than 10 cm or
adjacent organ concomitant removal.
Further studies are encouraged to continue
to improve our surgical results on such complex patients with a complex
disease.
REFERENCES
- Gill IS: The case for laparoscopic adrenalectomy. J Urol. 2001; 166: 429-36.
- Faria EF, Andreoni C, Krebs RK, Nascimento H, Goldman SM, Kater C, et al.: Advances in pheochromocytoma management in the era of laparoscopy. J Endourol. 2007; 21: 1303-7.
Dr.
Cassio Andreoni
Section of Urology
Federal University of Sao Paulo, UNIFESP
Sao Paulo, SP, Brazil
E-mail: cassio.andreoni@globo.com
EDITORIAL COMMENT
Pheochromocytomas
are relatively uncommon tumors whose operative resection has clear medical
and technical challenges.
While the safety and efficacy of laparoscopic
adrenalectomy are relatively well documented, few studies with extended
follow-up have been conducted to measure the success of the procedure
for the most challenging of the adrenal tumors. In addition, several reports
have questioned the applicability of a minimally invasive approach for
pheochromocytomas larger than 6 cm in diameter. This paper from Castilho
et al. evaluated long term results of laparoscopic adrenalectomy in patients
with pheochromocytoma (diameter ranging from 10 to 120 mm) and authors
have to be commended for this interesting work. As other series of laparoscopic
resection for pheochromocytoma, this paper shows that despite appropriate
perioperative medical management, intraoperative hypertensive remains
a valid concern especially during intra-abdominal insufflation and tumor
manipulation (1). In addition, it emphasizes that laparoscopic approach
to these tumors has traditionally been associated with higher complication
rates than adrenalectomy for other indications. Lesions larger than 6
cm are associated with longer operative times and may be more difficult
to safely resect laparoscopically. Extreme care must be taken to avoid
intraoperative capsular disruptions and lifetime follow-up is an important
aspect of the postoperative care of the pheochromocytoma patient (1).
Recently, robotic technology has been introduced providing a 3-dimensional
display that enhances depth perception, enabling the surgeon to operate
in a comfortable seated position in which the eye, hand, and target are
in line, and the instruments contain a “wrist” joint to improve
dexterity. These advantages could theoretically improve laparoscopic adrenalectomy
procedure and then subsequently lead to improved perioperative and postoperative
outcomes. We recently reported 24 patients with pheochromocytoma who underwent
unilateral robotic-assisted adrenalectomy (2). Conversion rate was 8.3%
and tumor capsule was ruptured in 1 patient with a right 7.5 cm cystic
pheochromocytoma (cyst rupture).
Moreover, per-operative hemodynamic modifications
seem to be similar during robotic and conventional adrenalectomy for pheochromocytoma
(unpublished data). This emphasizes that robotic approach can not be considered
de facto as precluding all difficulties that can be observed during conventional
laparoscopic adrenalectomy for pheochromocytoma. Laparoscopic excisions
of pheochromocytomas with or without robotic system remain challenging
surgical procedures because of intraoperative catecholamine release and
tumor vascularization. Extensive experience in minimally invasive techniques,
as well as in endocrine surgery are two key elements for surgeons performing
laparoscopic adrenalectomy for pheochromocytoma.
REFERENCES
- Kercher KW, Novitsky YW, Park A, Matthews BD, Litwin DE, Heniford BT: Laparoscopic curative resection of pheochromocytomas. Ann Surg. 2005; 241: 919-26; discussion 926-8.
- Brunaud L, Ayav A, Zarnegar R, Rouers A, Klein M, Boissel P, Bresler L: Prospective evaluation of 100 robotic-assisted unilateral adrenalectomies. Surgery. 2008; 144: 995-1001.
Dr.
M Fau &
Dr. Laurent Brunaud
Department of General and Endocrine Surgery
CHU Nancy, Hopital Brabois Adultes
School of Medicine, University of Nancy
Nancy, France
E-mail: l.brunaud@chu-nancy.fr