EMPHYSEMATOUS
CYSTITIS AS COMPLICATION IN CHRONIC REJECTION OF RENAL TRANSPLANT
(
Download pdf )
Radiology Page
Vol. 37 (1):
113-114, January - February, 2011
doi: 10.1590/S1677-55382010000100015
ERICH K. LANG, KARL ZHANG, DANIEL THORNER, QUAN D. NGUYEN
Department of Radiology (EKL, KZ, DT, QDN), SUNY, Downstate Medical School, Brooklyn, New York, USA and Johns Hopkins Medical Institutions, Bayview Center, Baltimore, Maryland, USA
ABSTRACT
This
43-year-old Caucasian female presented in a septic condition in the emergency
room. At the time of admission her temperature was 38.5 Celsius, white
blood cells (WBC) 12800, red blood cells 3.8 mill, hemoglobin 10.8, hematocrit
36, urea 28 mg/dl, serum creatinine 3.2 mg/dl, K 5.8 meq/l, Na 128 meq/l,
alk ptsa 142 U/l. Urine analysis 50 WBC/hpf, innumerable bacteria/hpf,
cellular debries, gas bubbles. Both urine and later blood cultures revealed
E. coli.
The lower abdomen and pelvis were exquisitely
tender to palpation. Patient had been hemodialyzed 2 days earlier. Patient
had received a cadaver-transplant 3 years ago, which functioned well until
4 months ago. At this time chronic rejection was diagnosed. An antegrade
pyelogram revealed a stricture at the implant site of the cadaver ureter,
dilatation and possible ulcerations of the mid – and upper ureter.
Bullous edema of the native bladder was seen, most prominent near the
implant site. Immunosuppressive therapy was instituted and despite these
efforts, function of the transplant kidney continued to deteriorate and
the patient was finally put on hemodialysis 1 month ago. It was contemplated
to perform a uretero-neo-calicostomy with the still present native ureter
to hopefully salvage the kidney
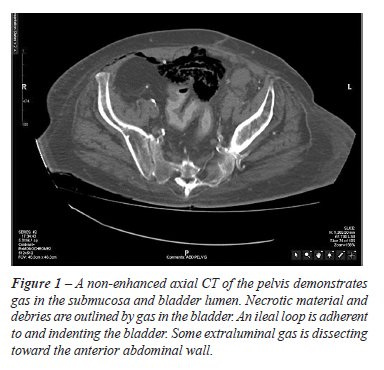
A non-contrast multi-detector computed tomography
demonstrated gas in the submucosa and bladder, and also extravesical anterior
to the bladder (Figure-1). Strands of debries and sloughed tissue surrounded
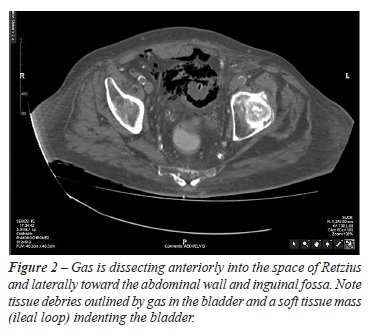
by air are seen in the bladder lumen (arrow). Gas has dissected along
the anterior abdominal wall (Figure-2). A coronal reconstruction shows
relatively little striation in the perirenal space. There is edema in
the peripelvic area and around the upper ureter (Figure-3).

To control the fulminating gas forming infection,
bladder, transplant kidney and ureter were removed, the space of Retzius
drained. Depending on the severity of the infection and underlying conditions
such as diabetes mere control of the diabetes and appropriate antibiotic
therapy may suffice while severe forms may mandate surgical intervention
to remove the necrotic debries (1-3). After prolonged antibiotic therapy
and hemodialysis the patient recovered and received a second successful
transplant kidney.
REFERENCES
- Dinckan R, Tekin R, Turkyilmaz S, Kacak H, Gurkan A, Erdogen G, Tuncer M: Early and late urologic complications corrected surgically following renal transplantation. Transpl. Int. 2007; 20: 702-7.
- Akalin E, Hyde C, Schmitt G, Kaufman J, Hamburger RJ: Emphysematous cystitis and pyelitis in a diabetic renal transplant recipient. Transplantation 1996; 62: 1024 -6.
- Davavri HR, Yarmohammadi H, Malekhosseini SA, Salahi H, Bahador A, Salchipoun S: Urologic complications in 980 consecutive patients with renal transplantation. Int. J. Urol. 2006; 13: 1271-5.
_______________________
Correspondence address:
Dr. Erich K. Lang
Departments of Urology and Radiology
SUNY, Downstate Health Science Center
455 Lenox Road
Brooklyn, NY, 11203, USA
E-mail: erich.lang@downstate.edu