VAGINAL WALL TRANSVERSE FLAP SLING FOR REPAIR OF SEVERE CYSTOCELE AND CYSTOURETHROCELE WITH ASSOCIATED STRESS INCONTINENCE
JAVIER C. ANGULO, RAFAEL LERA, MANUEL ESTEBAN, JOSE M. HONTORIA
Department of Urology, Hospital Principe de Asturias, Department of Morphological Sciences and Surgery, Universidad de Alcala, Alcala de Henares, Madrid, Spain
ABSTRACT
Objective:
Surgical treatment of severe anterior vaginal wall prolapse and associated
stress incontinence is controversial. We present our experience with a
modification of the vaginal sling combined with anterior colporraphy for
severe cystocele and cystourethrocele.
Patients and Methods: Since 1992 we used
this technique in 41 consecutive patients suffering stress incontinence
and anterior vaginal wall prolapse, with a minimum postoperative follow-up
of 1 year. Vaginal wall prolapse was severe in all cases: 19 (46%) grade
III and 22 (54%) grade IV cystocele. Stress incontinence was evidenced
in all cases, originally consulted in 29 (71%) and revealed by a positive
vaginal pack test in the rest (29%). Anterior colporraphy was accomplished
by percutaneous suspension of a large vaginal wall transverse flap that
was rotated to support the bladder neck and was sutured to the rectus
fascia. Vaginal hysterectomy and posterior colporraphy were performed
in 14 (34%) and 25 (62%), respectively.
Results: At a mean follow-up of 42 months
success rate was 93% (38/41) for cystocele repair and 88% (36/41) for
treatment of associated stress incontinence. Significant postoperative
detrusor instability was present in 9 (22%), and “de novo” developed
in 3 of them. Intermittent catheterization was needed in 22 (54%) and
time to resume postoperative voiding was 3.6 weeks, range 1-14. No patient
developed permanent urinary retention. No sexually active patient suffered
dispareunia six months after surgery. Mean hospital stay was 3.1 days,
including cases with hysterectomy.
Conclusions: Anterior colporraphy with buttressed
support of the bladder through a vaginal wall transverse flap sling is
a safe method for repair of severe cystocele or cystourethrocele and treatment
of associated stress incontinence that achieves satisfactory results at
a reasonable follow-up. This approach prevents development of stress incontinence
after surgery of cystocele in cases with a positive vaginal pack test.
Besides, the peculiar orientation of the vaginal mucosa harvested for
the sling avoids the potential problems of foreshortening the vaginal
vault.
Key words:
urinary incontinence; stress; bladder; surgery; cystocele
Braz J Urol, 27: 386-393, 2001
INTRODUCTION
Based
on novel concepts, the selection of the proper approach to treat stress
urinary incontinence must consider both the degree of anterior vaginal
wall prolapse and the anatomical origin of incontinence: hypermotility
or intrinsic sphincteric deficiency. Anterior vaginal wall prolapse can
be graded according to the level of descend of the bladder in relation
to vaginal introitus. Most often the bladder base produces the cystocele;
but the bladder neck and urethra are often involved, especially when prolapse
is severe. Urethral hypermobility and occult sphincteric deficiency are
generally present with moderate and severe cystocele (1).
The
classical approach to cystocele was based on the approximation of lax
pubocervical fascia and narrowing of the bladder neck (Kelly plication),
but failure rate in terms of correcting or preventing incontinence is
well-known (2). The abdominal approach of Burch colposuspension successfully
achieves continence in many cases but only treats mild-to-moderate cystocele
and needs a laparotomy (3). Its recent laparoscopical modification diminishes
both morbidity and hospital stay but is still inappropriate to cope with
a severe cystocele. In the search of a rational repair of severe cystocele
that allows improvement of results and decrease of morbidity, the transvaginal
route with combined bladder neck suspension and repair of the defect in
the pubocervical fascia was promoted (4,5). In this sense, some authors
have described the use of a vaginal tube fixed in the bladder neck or
suspended subcutaneously, similarly to the technique of Pereyra (6). Recently,
pubovaginal sling (7-9) and even transvaginal placement of a hammock of
nonabsorbable mesh (10) have been promoted as first choice therapy for
anterior vaginal wall prolapse and associated stress incontinence of any
kind.
We
report our experience with a modification of Raz procedure for the treatment
of severe anterior vaginal wall prolapse that uses the combination of
both anterior colporraphy and a transverse long vaginal flap sling to
support the bladder neck and effectively treat stress incontinence.
Surgical
Technique
The
patient is placed in the lithotomy position with access to the suprapubic
area and a 18F Foley catheter is inserted through the urethra and the
bladder emptied. Perioperative intravenous ampicillin and gentamicin are
administered, and will be continued until hospital discharge. The vagina
is exposed and a vertical midline incision is made in the anterior vaginal
wall, from the area of the mid urethra to the posterior edge of the cystocele,
and extended laterally to create a rectangular flap measuring 8 to 10
cm long and 3 to 4 cm wide (Figures-1A and B). This island of anterior
vaginal wall is dissected with the help of Allis clamps but great care
is taken to preserve the vascular supply of the vaginal wall. For this
purpose the periurethral fascia is included in the flap. This flap will
be transversely rotated to act as a sling and the contralateral side of
the vagina is incised and undermined to create a second advance flap that
will cover the island at a later step (Figures-1B and D). Lateral dissection
is performed along the periurethral fascia to the pubic bone. The urethropelvic
ligament is identified and bluntly dissected to perforate the endopelvic
fascia and enter the retropubic space. The bladder neck and urethra are
easily mobilized. At the level of the bladder base the pubocervical fascia
and the edge of levators are dissected from the bladder on each side and
separated from the herniated bladder that will be later introduced.
The
vaginal transverse flap sling is prepared. No. 1 polypropylene sutures
that incorporate the entire vaginal wall and periurethral fascia anchor
the four corners of the rectangle and are transferred individually using
a double-pronged ligature carrier from the vagina to the suprapubic region
up to the rectus fascia as designed by Raz et al. (11) (Figure-1C). The
sling is carefully placed at the level of the bladder neck and proximal
urethra. The edges of the pubocervical fascia are approximated by 2-0
polyglactic sutures from the bladder neck to the cardinal ligaments. Endoscopic
examination is helpful at this point to prevent unnoticed penetration
of bladder or urethra. Vaginal hysterectomy and/or posterior colporraphy
can be performed at this time if needed. The lateral vaginal wall flap
is advanced to restore the integrity of the vagina using a running 2-0
polyglactic suture (Figure-1D). Only after closure of the vaginal wall
the 4 sutures are tied independently by the assistant at the small suprapubic
incision on each side. Not much tension is needed but urethral motility
must no longer be felt by tugging on the Foley catheter while the knot
is tied down. The small suprapubic incisions are closed. A vaginal pack
is not considered necessary unless significant bleeding persists, and
we do not use suprapubic tube either. The Foley catheter is removed on
postoperative day 2 and post-void residual is recorded. If patient is
unable to void, or residual volume is greater than 100 cc, intermittent
self-catheterization is started. The patient is taught and supervised
in the office, thus allowing early discharge. Intermittent catheterization
is continued until residual urine is consistently less than 100 cc. All
patients were examined, operated, and controlled by the same surgeon (JCA).
To reduce potential examiner bias, a blinded third party (ME) reevaluated
all patients postoperatively, independently from surgeon assessment. Follow-up
was closed at the time outcome measurements, based on physical examination
and physician’s interview, were performed. Presence of a significant
cystocele, continence status, persistent and de novo urge incontinence,
duration of self-catheterization, and the possibility of dyspareunia were
recorded.
Patients
Since
1992 we have used this technique in 41 consecutive patients suffering
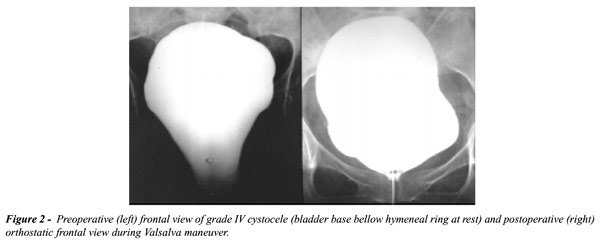
severe cystocele, with a minimun follow-up of at least one year. Inclusion
criteria were large (grade III and IV) cystocele (Figure-2), positive
vaginal pack test, and absence of previous surgical procedures to correct
incontinence. Mean age was 65.4 years (C.I. 62.8-67.9, range 49-76). In
19 patients (46%) the bladder base appeared outside introitus with strain
(grade III cystocele) and in 22 (54%) the bladder base was below the hymeneal
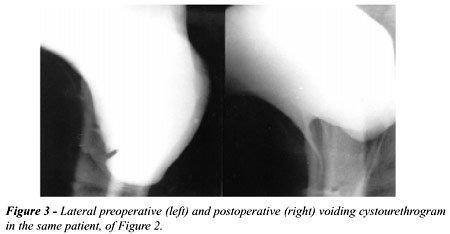
ring at rest (grade IV cystocele or cystourethrocele). The degree of the
cystocele was also documented under fluoroscopic monitoring with the patient
in standing position (Figure-3). Vaginal pack test demonstrated stress
incontinence in all cases (n = 41). Without insertion of the vaginal pack,
stress urinary incontinence was evidenced on physical examination in 29
cases (71%) and the vaginal pack test demonstrated occult incontinence
in the remaining 12 (29%). Patients with a large cystocele that remained
continent after vaginal pack insertion are not the object of this communication
as they received cystocele repair alone without the vaginal sling. Incontinent
patients, either at initial examination or after the pack test, were treated
as described above by anterior colporraphy and vaginal wall transverse
flap sling. Multichannel cystometry was performed before surgery in 22
patients (54%) and approximately 30-60 days after surgery in 8 (20%).
Indications for preoperative urodynamic study were associated urgency
incontinence and previous surgical procedure (vaginal hysterectomy and
failed cystocele repair). Urodynamic study was performed postoperatively
when results were unsatisfactory, either due to persistent stress incontinence
or de novo urge incontinence. A number of added procedures were needed
to complete perineal repair. Vaginal hysterectomy was performed in 14
cases (34%), posterior colporraphy in 25 (62%), and enterocele repair
and vaginal vault prolapse in 1 (2.4%) each. Hysterectomy was indicated
either for medical reasons (e.g., fibroids, bleeding) or because of the
presence of significant uterine prolapse associated with pelvic discomfort
and dyspareunia. This procedure had been previously performed in 7 cases
(17%), 4 of them with associated failed colpoperineorraphy. Patients were
periodically followed until June 1999, and outcome was assessed from June
1999 to September 1999.
RESULTS
At
a mean follow-up of 42 months (C.I. 31.3-52.8, range 12 to 83) 36 of the
41 patients were completely continent for a success rate of 88%. Continence
is defined as absent or very rare stress incontinence, without need of
pads or any social limitations. Among the cases that were incontinent
after surgery, 2 patients worn 2 pads or less a day and 3 patients used
at least 3 pads. Abdominal leak point pressure was under 60 cm water in
4 of 5 cases with failure, thus suggesting intrinsic sphincter deficiency.
In one case incontinence was demonstrated before surgery only by a positive
vaginal pack test, but it was clinically overt after surgery. Therefore,
we were able to correct stress incontinence in 25 of 29 patients (86%)
with severe cystocele and associated stress incontinence and were able
to prevent development of incontinence in 11 of 12 patients (92%) in which
incontinence was only revealed by a positive vaginal pack test.
Preoperative
Valsalva leak point pressure ranged from 15 to 180 cm H20 (mean 61.3,
SE 8.6) in the patients studied. Stress incontinence was accompanied by
urgency incontinence at diagnosis in 16 patients (39%) and urodynamic
testing demonstrated instability in 13. Postoperative significant detrusor
instability (i.e. frequency, urgency and/or urge incontinence in the absence
of a positive urine culture) was complained in 9 cases (22%). It appeared
de novo in 3 patients (7%) and persisted despite surgery in 6 (15%). In
all cases it was effectively controlled with anticholinergic therapy and
no patient suffered urge incontinence. Therefore, with the use of this
surgical procedure, bladder instability disappeared after cystocele repair
in a significant number of cases (10 of 16 patients), and was easily managed
medically in the rest.
The
success rate for anatomical cystocele repair with the vaginal wall transverse
flap sling and colporraphy was 93%. Cured cystocele, considered so when
an excellent anterior vaginal wall support or a mild asymptomatic cystocele
in the standing position is documented, was achieved in all cases but
three. Persistent cystocele was mild but symptomatic, and 2 of them coexisted
with stress incontinence. There were no intraoperative complications,
such as need for blood transfusion, bladder perforation or fistula formation.
Postoperative complications include already mentioned de novo detrusor
instability (3 cases); wound infection with formation of a suprapubic
abscess (1 case), and enterocele formation (1 case). No patient suffered
permanent retention but 22 (54%) suffered it transiently, i.e. needed
intermittent catheterization, a week or more. Among them, the mean time
to resume voiding with postvoid residual under 100 cc was 3.6 weeks (range
1 to 14 weeks, C.I. 1.8-5.4). No patient complained dyspareunia postoperatively.
Mean hospital stay was 3.1 days (C.I. 2.5-3.7, median 3 days), and that
included cases with hysterectomy. Mean stay of 27 cases treated with anterior
colporraphy and vaginal wall transverse flap sling without hysterectomy
was 2.2 days (C.I. 1.6-2.8).
We
present a simple and secure vaginal procedure for the correction of severe
cystocele or cystourethrocele and associated incontinence, either evident
or occult. This technique incorporates anterior colporraphy with buttressed
support of the bladder neck through a vaginal sling. The peculiar transversely
rotated quadrangular flap we describe, later covered by a second contralateral
advance flap, allows a very satisfying reconstruction of redundant anterior
vaginal wall and is particularly appropriate to repair a large cystocele.
The main advantage over the conventional inverted U vaginal flap described
by Raz et al. (11) is that no vaginal shortening is to be expected but
a reconstructive narrowing is performed instead. Dyspareunia has been
investigated and proved absent in every case.
Many
patients with severe genital prolapse have underlying incontinence uncovered
during urodynamic testing (13). We consider this technique is specially
indicated when severe cystocele is accompanied by a positive vaginal pack
test. Under this circumstance a high percentage of patients demonstrates
internal sphincteric deficiency and the rest suffer urethral hypermotility
(1). Once type III incontinence is identified pubovaginal or vaginal sling,
in addition to pelvic floor repair, is recommended (14-16). Results of
vaginal and pubovaginal slings appear equally satisfactory on the long-term
(17). Besides, increasing evidence exits to expand the indication of sling
procedures for treatment of type II stress incontinence, based on its
high success rate and affordable low number and severity of complications
related to the procedure (i.e., long-term obstruction and de novo detrusor
instability). Sling procedures can therefore be the ideal overall treatment
for stress incontinence regardless of type, and be indicated as first
line treatment for both urethral hypermotility and intrinsic sphincteric
deficiency (16,18-20).
We
report 93% cure rate for cystocele and 88% cure rate for incontinence
with the use of anterior colporraphy with vaginal wall transverse flap
sling, at a mean follow-up of more than 3 years. The fact that the vaginal
pack test was positive in all cases means a high proportion of patients
with complicated type III stress incontinence has been selected and, even
though, outcome is encouragingly good. Anterior colporraphy with buttressed
support of the bladder through a vaginal wall transverse flap sling, is
a safe method to prevent development of iatrogenic incontinence after
repair of severe cystocele. It is a minimally invasive vaginal procedure
that can easily be combined with vaginal hysterectomy and/or posterior
colporraphy. It obviates the morbidity associated with an abdominal procedure
and allows early hospital discharge.
Herniation
of the bladder outside the introitus, either with strain (grade III cystocele)
or at rest (grade IV), implies severe weakness of vesicopelvic fascia
both in its lateral aspect (lateral defect) and in the midline (central
defect). According to Raz et al., the lateral defect can be repaired by
a four corner bladder neck suspension that supports the bladder base anchoring
the pubocervical fascia, cardinal ligaments and vaginal wall; and the
central defect is repaired by re-approximation of the pubocervical fascia
and cardinal ligaments in the midline (2,5). The Burch operation both
corrects urethral hypermotility and repairs the cystocele by suspending
the vaginal wall and secondarily the urethra and bladder to Cooper’s
ligament, without urethral obstruction (12). A vaginal wall sling has
the advantage to provide both compression and support for the urethra
and also resuspend the bladder neck (21). It has proved an excellent option
for the treatment of both genuine incontinence and intrinsic sphincteric
deficiency (16,22). Therefore, vaginal sling combined with central defect
repair by re-approximation of the pubocervical fascia and cardinal ligaments
is a logical option for repair of anterior vaginal wall prolapse. The
technique we describe is a variation of the pubovaginal sling that uses
a flap of anterior vaginal wall, and could behave more like a pubovaginal
sling than the vaginal sling described by Raz et al. In this sense, the
results we present could be better than those reported for other techniques
to treat large cystoceles; however, prospective comparative trials evaluated
with validated questionnaires are needed. Other authors have already proposed
the association of a sling and formal cystocele repair as a good option
within the therapeutic arsenal of large volume cystocele (7-10,23).
The
degree of cystocele formation is not totally related to the degree of
incontinence. A large cystocele may serve as a pressure-relief system
that protects a poor urethral continence mechanism and prevents leakage
with exercise. The vaginal pack test is a simple maneuver to identify
patients at risk for stress urinary incontinence after repair of a cystocele.
If urethral hypermotility or intrinsic sphincteric deficiency is not detected
and, therefore, cystocele repair is not completed with any form of urethral
support, de novo stress incontinence is very likely to develop. Surgical
techniques that do not face the possibility of sphincteric deficiency
are at increased risk of failure. Anterior colporraphy with buttressed
support of the bladder through a vaginal wall transverse flap sling is
a safe method for repair of severe cystocele or cystourethrocele and treatment
of associated stress incontinence or prevention of the novo stress incontinence
after a positive vaginal pack test. Anterior colporraphy alone may be
effective enough, however, to cure a cystocele with a negative pack test
during evaluation. We share the opinion that vaginal pack test makes sophisticated
videourodynamics equipment unnecessary for evaluation of large cystourethrocele
(24). Abdominal leak point pressure is not valid in the presence of a
cystocele and cannot be taken as an accurate indicator to classify type
II or III incontinence under this circumstance, neither can it define
the appropriate operation. Based on increasingly acceptance of sling procedures
for type II incontinence, we have abandoned Raz bladder neck or Burch
abdominal suspensions to treat grade III and IV cystocele with a positive
vaginal pack test and currently perform a vaginal wall sling in the fashion
we describe. It not only suspends the bladder neck, but also elevates
the whole trigone centrally and laterally, and reinforces paraurethral
and paravesical fascia with a resistant and totally biocompatable tissue.
We hope that same as its close relative, fascial pubovaginal sling, this
technique withstands the test of time.
In
conclusion, we consider vaginal wall transverse flap sling in combination
with anterior colporraphy is a reconstructive technique of choice for
severe cystocele or cystourethrocele with a positive vaginal pack test.
This simple and minimally invasive technique can be easily combined with
vaginal hysterectomy or posterior colporraphy. Morbidity is minimal and
laparotomy is avoided. Transitory retention requiring intermittent catheterization
is frequent but we have not observed permanent retention. De novo detrusor
instability develops in a small percentage but can be managed with anticholinergics.
Mean hospital stay is short, even when hysterectomy or other associated
procedures are performed.
- Gohniem GM, Walters F, Lewis V: The value of the vaginal pack test in large cystoceles. J Urol, 152: 931-934, 1994.
- Raz S, Klutke CG, Golomb J: Four-corner bladder and urethral suspension for moderate cystocele. J Urol, 142: 712-715, 1989.
- Van Geelen JM, Theeuwes AGM, Eskes TKAB, Martin CB: The clinical and urodynamic effects of anterior vaginal repair and Burch colposuspension. Am J Obstet Gynecol, 159: 137-144, 1988.
- Leach GE, Zimmern P, Staskin D, Schmidbauer CP, Hadley HR, Raz S: Surgery for pelvic prolapse. Semin Urol, 4: 43-50, 1986.
- Raz S, Little NA, Juma S, Sussman EM: Repair of severe anterior vaginal wall prolapse (grade IV cystourethrocele). J Urol, 146: 988-992, 1991.
- Benizri EJ, Volpé P, Pushkar D, Chevallier D, Amiel J, Sanian H, Toubol J: A new vaginal procedure for cystocele repair and treatment of stress urinary incontinence. J Urol, 156: 1623-1625, 1996.
- Cross CA, Cespedes RD, McGuire EJ: Treatment results using pubovaginal slings in patients with large cystoceles and stress incontinence. J Urol, 158: 431-434, 1997.
- Cross CA, Cespedes RD, McGuire EJ: Our experience with pubovaginal slings in patients with stress urinary incontinence. J Urol, 159: 1195-1198, 1998.
- Chaikin DC, Rosenthal J, Blaivas JG: Pubovaginal fascial sling for all types of stress urinary incontinence: long-term analysis. J Urol, 160: 1312-1316, 1998.
- Nicita G: A new operation for genitourinary prolapse. J Urol, 160: 741-745, 1998.
- Raz S, Siegel AL, Short JL, Synder JA: Vaginal wall sling. J Urol, 141: 43-46, 1989.
- Burch JG: Urethrovaginal fixation to Cooper’s ligament for correction of stress incontinence, cystocele, and prolapse. Am J Obst Gynec, 81: 281-290, 1961.
- Rosenzweig BA, Pushkin S, Blumenfeld D, Bhatia NN: Prevalence of abnormal urodynamic test results in continent women with severe genitourinary prolapse. Obst Gynec, 79: 539-542, 1992.
- McGuire EJ, Bennett CJ, Konnak JA, Sonda LP, Savastano JA: Experience with pubovaginal slings for urinary incontinence at the University of Michigan. J Urol, 138: 525-526, 1987.
- Blaivas JG, Jacobs BZ: Pubovaginal fascial sling for the treatment of complicated stress urinary incontinence. J Urol, 145: 1214-1218, 1991.
- Raz S, Stothers L, Young GPH, Short J, Marks B, Chopra A, Wahle GR: Vaginal wall sling for anatomical incontinence and intrinsic sphincter dysfunction: efficacy and outcome analysis. J Urol, 156: 166-170, 1996.
- Juma S, Little NA, Raz S: Vaginal wall sling: four years later. Urology, 39: 424-428, 1992.
- Zaragoza MR: Expanded indications for the pubovaginal sling: treatment of type 2 or 3 stress incontinence. J Urol, 156: 1620-1622, 1996.
- Klutke CG: Editorial: Female stress incontinence in the 1990s - changing concepts. J Urol, 156: 1626-1627, 1996.
- Kane L, Chung T, Lawrie H, Iskaros J: The pubofascial anchor sling procedure for recurrent genuine urinary stress incontinence. Br J Urol, 83: 1010-1014, 1999.
- Stothers L, Chopra A, Raz S: Vaginal reconstructive surgery for female incontinence and anterior vaginal-wall prolapse. Urol Clin North Am, 22: 641-655, 1995.
- Litwiller SE, Nelson RS, Fone PD, Kim KP, Stone AR: Vaginal wall sling: long-term outcome analysis of factors contributing to patient satisfaction and surgical success. J Urol, 157: 1279-1282, 1997.
- McGuire EJ, Gardy M, Elkins T, DeLancey JOL: Treatment of incontinence with pelvic prolapse. Urol Clin North Am, 18: 349-353, 1991.
- Zimmern PE. Re: Treatment results using pubovaginal slings in patients with large cystoceles and stress incontinence. Letter. J Urol, 160: 132-133, 1998.
Received: June 26, 2000
Accepted after revision: July 12, 2001
_______________________
Correspondence address:
Dr. Javier C. Angulo
Department of Urology
Hospital Principe de Asturias
Carretera Alcalá-Meco s/n, Alcalá de Henares
Madrid 28805, Spain
Fax: + + (34) (91) 880-1825
E-mail: jangulo@futurnet.es