RIGID
URETEROSCOPY FOR DIAGNOSIS AND TREATMENT OF URETERAL CALCULI DURING PREGNANCY
(
Download pdf )
GUSTAVO C. LEMOS, OMAR R. EL HAYEK, MARCELO APEZZATO
Albert Einstein Jewish Hospital, São Paulo, SP, Brazil
ABSTRACT
Objective:
To evaluate ureteroscopy as a treatment option for women presenting ureteral
calculi during pregnancy.
Materials and Methods: Eighteen pregnant
patients presenting renal colic and indication of surgical treatment for
ureteral calculi were analyzed. Patients were 20 to 34 years old (medium
= 28), and the gestation period ranged from 12 to 34 weeks (medium = 18).
Lumbar pain was present in 14 patients, and 4 had diffuse abdominal pain.
Four patients were febrile in the occasion of the examination. Thirteen
patients presented microscopic hematuria, 8 leucocituria, and 4 positive
urine culture. The stone was detected by ultrasonography (US) in 12 patients.
Magnetic resonance imaging (MRI) was performed in 2 cases, and did not
demonstrate calculi. The stone location was: 1 in the superior ureter
(pregnancy of 15 weeks), 4 in the medium ureter (pregnancy of 12, 15,
18 and 20 weeks), 12 in the inferior ureter, and 1 was not determined.
The surgical indication was difficult pain control, fever, and presence
of uterine contractions.
Results: Double-J insertion, as single treatment,
was possible in 4 patients and it was kept in place for up to 2 weeks
after delivery. Among the patients submitted to ureteroscopy, the calculi
retrieval was always possible, except in 1 case where the calculus was
not located by US, MRI or ureteroscopy. In 2 patients, the ultrasonic
lithotriptor was used and in 11 the stone was removed intact with a basket.
There were no complications due to the procedure and all pregnancies were
carried to full term.
Conclusion: Rigid ureteroscopy for extraction
of ureteral calculi during pregnancy is efficient and safe.
Key words: ureter; ureteral obstruction; calculus; pregnancy; ureteroscopy
Int Braz J Urol. 2002; 28: 311-6
INTRODUCTION
The
incidence of urolithiasis in pregnant women varies from 0.026 to 0.531%
(1). Symptomatic calculi appear in 1:1,500 pregnancies and is a predetermining
factor of premature delivery (2). Calculi occur most frequently in multiparous
women, are usually present in the second and third trimesters and are
equally frequent in both sides (3,4).
Pregnancy
does not predispose to calculi formation, but the dilation of the superior
urinary tract caused by the ureteral compression does facilitate the movement
of pre-existent kidney calculi. The diagnosis of urolithiasis during pregnancy
is more difficult, because the symptoms are misdiagnosed for the common
pain of this period, besides the fact that the colic is of low intensity.
From 65 to 85% of the ureteral calculi in pregnant women are spontaneously
eliminated with the use of analgesics, hydration and infection control,
when present (5). Aggravating factors, such as fever, infection and uncontrolled
pain, indicate interventionist treatment.
The
less aggressive method for ureteral drainage is the simple introduction
of a double-J catheter under ultrasonographic control and its use until
the end of the pregnancy. The extracorporeal lithotripsy is not indicated
during pregnancy due to the risks of abortion and teratogeny (1,6). Ureteroscopy
in pregnant woman looks difficult at first sight due to the anatomic distortions
caused by the size of the uterus. In practice, these difficulties do not
occur and the high rate of success and safety of this procedure is making
it one of the best surgical options for the definite treatment of ureteral
calculi (7). The calculus can be removed with the Dormia basket or fragmented
with ultrasonic, ballistic or laser lithotriptors. The electrohydraulic
lithotriptor should be avoided because of the higher risk of ureteral
lesion (7).
MATERIALS AND METHODS
Eighteen
pregnant patients from 20 to 34 years of age (median = 28), suffering
from renal colic and with indication for ureteral drainage were studied.
The gestational period varied from 12 to 34 weeks (median = 18). Fourteen
patients reported lumbar pain, and 4 reported diffuse abdominal pain.
Four patients presented with fever in the examination. Nine had previous
history of renal colic due to lithiasis.
Analgesia
was performed with 20 mg of hyoscine and 2 ml of intravenous dipirone.
In the emergency room, patients were submitted to abdominal ultrasonography,
urine sediment analysis, urine culture and antibiogram.
Microscopic
hematuria was present in 13 patients, leukocytosis in 8 and positive urine
culture in 4. Three patients had Escherichia coli and 1 Klebisiela sp.
They were the patients with fever. It was possible to locate the calculus
with ultrasound (US) in 12 patients. In the other 6, the presumptive diagnosis
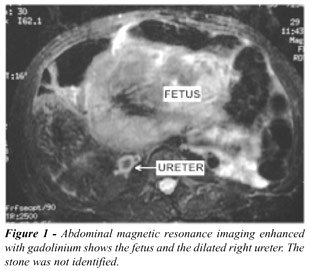
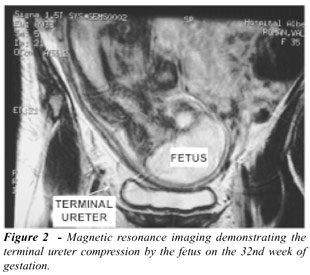
was done by the signs and symptoms. Magnetic resonance imaging (MRI) was
performed in 2 patients and did not locate the calculus in any of them
(Figure-1 and 2). Ureteroscopy was performed in 14 patients, establishing
the diagnosis in 13. The calculi dimension on the US varied from 4 to
12 mm, median of 6 mm.
As
for location, 1 calculus was in the superior ureter (pregnancy of 15 weeks),
4 in the mid-ureter (pregnancy of 12, 15, 18 and 20 weeks), 12 in the
inferior ureter, and in 1 patient the calculus was not located. Ten calculi
were on the right side and 8 on the left side.
The
difficulty to control the pain, the fever, and the increase in the number
of uterine contractions were the factors which led to the indication of
surgical intervention. The technique of choice was ureteroscopy with complete
removal of the calculus. The decision to introduce or not a double-J stent
at the end of the procedure depended on the lesion to the ureteral mucosa
caused by calculi fragmentation or removal. The double-J stent introduced
after ureteroscopy was kept in place for 10 days. In the cases of fever,
the calculi were not manipulated, double-J stents were introduced and
kept in place until the end of pregnancy, without any further manipulation.
The
anesthesia used was the epidural associated to midazolam sedation. The
surgical procedure consisted of cystoscopy with introduction of a safety
guide-wire in the ureter up to kidney or until resistance. After removing
the cytoscope, the 7F or 10F ureteroscope was placed with a second guide-wire
in its working channel. This second guide-wire was introduced only some
centimeters over the optic, and the ureteroscope was placed under direct
vision until the calculus. Dilation of ureteral meatus was not necessary
in any patient. After visualization of the calculus, the working guide-wire
was substituted by the extracting basket which, appropriately placed,
allowed the apprehension and removal of the calculus under direct vision.
In the cases of larger calculi, in which removal was impossible without
fragmentation, the basket was unassembled, the ureteroscope removed from
the ureter and reintroduced by the side of the basket and by the safety
guide-wire. The ultrasonic lithotriptor was introduced through the working
channel and the calculus was fragmented inside the basket. All fragments
were removed from the ureter with extracting stent. The safety guide-wire
was placed into the renal pelvis under direct vision to allow safe introduction
of a double-J catheter.
In
2 patients with calculi in the mid-ureter, and 2 with calculi the inferior
ureter, presenting with leucocituria and fever, the treatment was only
the introduction of a silicone double-J catheter which was kept in place
until the end of the pregnancy, without no further manipulation. The other
14 patients were submitted to ureteroscopy, and a double-J ureteral stent
was placed at the end of the procedure in 8 of them. In the vesical extremity
of the catheter, a nylon 3-0 was tied and exteriorized through the urethra
to allow its ambulatory removal after 10 days.
In
2 patients the placement of the double-J stent was monitored with ultrasound,
in 1 patient with fluoroscopy, and in the others no image control was
used. The fluoroscopy was used in 1 patient due to an ureteral fold which
impaired the guide-wire introduction and consequently the access to the
calculus. Thirty-six seconds of fluoroscopy were used in a pregnancy of
32 weeks.
RESULTS
The
introduction of a double-J stent, as a single treatment, was possible
in the 4 patients in which it was indicated. The fever disappeared 24
hours after intervention and the stent was kept in place until 2 weeks
after delivery.
Among
the 14 patients submitted to ureteroscopy, it was possible to determine
a lithiasic etiology of the obstruction in 13 cases. In these cases of
calculus, its removal was always possible. In one patient the diagnosis
of renal colic was clinical, and this woman presented with intense colic
abdominal pain, large dilation of the right superior ureter and hydronephrosis,
but no calculus was located by the US, MRI or ureteroscopy. During caesarian
in this patient, a large adherence of the right tube and ovary to the
abdominal wall was seen. The uterine growth probably determined the stretch
of these structures with pain simulating renal colic. In 2 patients, the
calculus was fragmented with ultrasonic lithotriptor, and in 11 it was
removed intact by using extracting baskets. The double-J catheter was
removed in the physician’s office on the 10th postoperative day by
pulling the nylon wire.
There
were no complications in any of the patients and all gestations were carried
on till the end.
DISCUSSION
During
pregnancy, the renal physiology and urinary tract anatomy are altered.
Uretero-hydronephrosis occurs in up to 90% of the pregnant women, and
the renal colic is the major non-obstetric cause of hospitalization (6,8).
This dilation is due to ureteral compression by the uterus, iliac vessels
and dilated ovarian veins, which appear on the second trimester and disappear
1 month after the birth. The ureteral compression is very evident in MRI.
Generally the dilation is non-symptomatic, nevertheless it may cause colic
pain which improve when the patient lies down on the pain contralateral
side (9).
The
causes of nephrolitiasis during pregnancy are idiopathic hypercalciuria
in 42%, hyperuricosuria in 13%, struvite calculus in 13%, hyperparatireoidism
in 10%, cystine calculus in 3%, and idiopathic in 19% (10).
The
diagnosis of renal colic by lithiasis in pregnant women is very difficult
due to the different causes of pain during pregnancy. The lumbar pain
is the most frequent symptom in the pregnant woman, and it can be intermittent
or continuous, irradiated to the abdomen inferior and anterior quadrant
(5). Lumbar pain secondary to overweigh of the spinal column, pubic pain
because of the disjunction of the symphysis at the end of the pregnancy,
urinary infection, and dilation of the urinary tract by ureter compression
are very common. Location of the pain is very altered by uterine growth
which dislocates organs and alters irradiations (8). The pain is generally
accompanied by nausea, vomiting, increase in urinary frequency and urgency.
Hematuria,
both macro and microscopic, is a frequent sign, but is not specific (5,8,11).
Urinary infection is present in 20 to 45% of the cases of calculus during
pregnancy (1,10,12). Ultrasonography is the main diagnostic method in
these cases, because besides its non-invasive nature, it does not use
radiation, and is universally available (4,8). Its sensibility in the
diagnosis of ureteral calculus during pregnancy reaches 95% (6).
In
exceptional cases of diagnostic difficulties and persistent obstruction,
patients can be submitted to intravenous urography with 3 plain films;
1 simple, 1 after 5 minutes of contrast medium injection, and another
after 15 minutes. The fetus will be exposed to 0,2 radiation, dose which
after the 17th week of pregnancy does not increase significantly the risk
of malformations (1,4,8). Sometimes the use of the X-Ray is necessary
and cannot be substituted by the US. In these cases, the benefits surpass
the potential risks to the fetus (13). The exposure of the fetus to radiation
can be minimized diminishing to the minimum the time of fluoroscopy, use
of collimation devices, lead aprons, and few number of exposures (13-15).
The
intravenous urography by magnetic resonance imaging (MRI) with gadolinium
is a new and very promising method (16). The calculus is not visible by
resonance, being detected by indirect signs, such as the inverted calyx
sign. The MRI is only useful in cases of moderate to large dilation of
the excretory system. Unfortunately, it is an expensive procedure and
is not available in all centers (16).
Ureteroscopy
as a method for diagnosing ureteral obstruction during pregnancy is very
efficient, but is also aggressive. In our series, it has been indicated
to 6 patients with clinical diagnosis of renal colic, dilation of excretory
system and indication of drainage. In 5 of these cases, the cause of the
obstruction could be identified and corrected. We do not support the isolated
diagnostic ureteroscopy during pregnancy. There are cases of intense renal
colic of difficult clinical control which cause increase of uterine contractions
and, therefore, lead to the risk of premature delivery. In these cases,
even without confirmation of ureteral calculus by imaging examination,
and only with clinical evidences and indirect signs, 6 patients were submitted
to ureteroscopy. In 5 patients there was a calculus which was removed.
Most
ureteral calculi during pregnancy are eliminated with analgesia, rest
and hydration (1,5,17). When an interventionist treatment is necessary,
the options are the introduction of a double-J ureteral catheter, ureteroscopy
and open ureterolithotomy (1,4,5,8). The extracorporeal lithotripsy is
not indicated during pregnancy due to the risk of placenta detachment,
lesion to the fetal pulmonary parenchyma and possible risks of malformation,
still unknown (1,8).
Pregnant
patients with ureteral calculus and fever should be treated with antibiotics
and drainage of the urinary system. The introduction of a double-J catheter
is an efficient and low invasive method. These patients should not be
submitted to ureteroscopy because ureteral manipulation and liquid injection
under pressure in the excretory system may lead to bacteriuria and dissemination
of the infection. The disadvantage of the treatment with double-J stent
isolated is the need for catheter permanence until the end of pregnancy,
which can be a predisposing factor to infections and may cause vesical
discomfort in most patients (18).
Ureteroscopy
in pregnant woman follows the usual rules, except for the use of fluoroscopy.
Ureteroscopy appeared in the beginning of the 80’s, and the first
studies published on ureteroscopy in pregnant women were of 1996 (7,19).
It was supposed that anatomic distortions caused by the fetal presence
would not allow the introduction of the rigid ureteroscope and that this
surgery could be of high risk to the pregnancy. The natural ureteral dilation
in pregnancy facilitates the introduction of the ureteroscope (19). In
the present series, we have used the 7F and 10F ureteroscope, without
need of dilating the ureteral meatus in any of the cases. In fact, this
procedure is simpler than it was supposed in the past.
CONCLUSION
Ureteroscopy for diagnosis and removal of ureteral calculi during pregnancy is an efficient and safe method. We cannot support the method only for diagnosis, but it can be useful as a single procedure, associating diagnosis and treatment, in difficult cases.
REFERENCES
- Hendricks SK, Ross SO, Krieger JN: An algorithm for diagnosis and therapy of management and complications of urolithiasis during pregnancy. Surg Gynecol Obstet. 1991; 172: 49-54.
- Drago, JR, Rohner, TJJr, Chetz, RA: Management of urinary calculi in pregnancy. Urology. 1982; 20: 578-81.
- Maikranz P, Coe FL, Parks J: Nephrolithiasis in pregnancy. Am J Kidney Dis. 1987; 9: 354-8.
- Maikranz P, Lindheimer M, Coe F: Nephrolithiasis in pregnancy. Bailliere’s Clin Obstet Gynaecol. 1994; 8: 375-86.
- Stothers, L, Lee, LM: Renal colic in pregnancy. J Urol. 1992; 148: 1383-7.
- Swanson SK, Heilman RK, Eversman WG: Urinary tract stones in pregnancy. Surg Clin North Am. 1995; 75: 123-42.
- Carringer,M, Swartz R, Johansson JE: Management of ureteric calculi during pregnancy by ureteroscopy and laser lithotripsy. Br J Urol. 1996; 77: 17-20.
- Parulkar BG, Hopkins TB, Wollin MR, Howard PJ Jr, Lal A: Renal colic during pregnancy: a case for conservative treatment. J Urol. 1998; 159: 365-68.
- Rasmussen PE, Nielsen FR: Hydronephrosis during pregnancy: A literature survey. Eur J Obstet Gynecol Reprod Biol. 1988; 27: 249-59.
- Coe FL, Parks JH, Lindheimer MD: Nephrolithiasis during pregnancy. N Engl J Med. 1978; 298: 324-6.
- Epstein FB: Acute abdominal pain in pregnancy. Emerg Med Clin North Am. 1994; 12: 151-65.
- Kammerer WS: Nonobstetric surgery in pregnancy. Med Clin North Am. 1987; 71: 551-60.
- Gray JE: Safety (Risk) of Diagnostic Radiology Exposures. In: Janower ML, Linton OW (eds.): Radiation Risk: A Primer. American College of Radiology, Commission on Physics and Radiation Safety, Committee on Radiologic Units, Standards and Protection, 1996, pp. 15-32.
- Gibbs SJ: Basic Mechanisms of Radiation Injury Somatic and Genetic. In: Janower ML, Linton OW (eds.): Radiation Risk: A Primer. American College of Radiology, Commission on Physics and Radiation Safety, Committee on Radiologic Units, Standards and Protection, 1996, pp. 5-15.
- Wyte CD: Diagnostic modalities in the pregnant patient. Emerg Med Clin North Am. 1994; 12: 9-17.
- Spencer JA, Tomlinson AJ, Weston MJ, Lloyd SN: Early report: comparison of breath-hold MR excretory urography, Doppler ultrasound and isotope renography in evaluation of symptomatic hydronephrosis in pregnancy. Clin Radiol. 2000; 55: 446-53.
- Cass AS, Smith CS, Gleich P: Management of urinary calculi in pregnancy. Urology. 1986; 28: 370-2.
- Delakas D, Karyotis I, Loumbakis P, Daskalopoulos G, Kazanis J, Cranidis A: Ureteral drainage by double-J-catheters during pregnancy. Clin Exp Obstet Gynecol. 2000; 27: 200-2.
- Scarpa, RM, de Lisa A, Usai E: Diagnosis and treatment of ureteral calculi during pregnancy with rigid ureteroscopes. J Urol. 1996; 155: 875-7.
__________________________
Received: September 26, 2001
Accepted after revision: April 30, 2002
_______________________
Correspondence address:
Dr. Gustavo Caserta Lemos
Av. Albert Einstein, 623 / sala 1313
05651-901, São Paulo, SP, Brazil
Fax: + 55 11 3845-1118
E-mail: gclemos@ajato.com.br
EDITORIAL COMMENT
Pregnant
patients who present with renal colic present many difficulties for their
physicians and this paper by Lemos and colleagues outlines some of the
problems. The diagnosis may be difficult to make in many individuals owing
to the necessity to avoid ionizing radiation and when the diagnosis is
made, the treatment of the patient may be unsatisfactory. In the past,
double-J stents have been placed as a procedure of first choice in the
hope of unobstructing the kidney and relieving the patient’s discomfort.
The stent, however, often causes seemingly as many problems as the original
stone and at least in some patients the stent may become calcified and
present significant difficulties in its removal after pregnancy has run
its course.
The
authors present a good case for ureteroscopic extraction of stones as
primary treatment in pregnancy and I certainly, in general terms, support
this concept. Certainly in an era of small flexible and rigid instruments,
if the stone can be seen, it can almost always be destroyed by methods
of intracorporeal lithotripsy.
I
think, however, a number of caveats need to be recognized. If the patient
is febrile, or has other signs of infection, double-J stent drainage for
a few days to stabilize the patient, reduce the fever, and have an opportunity
to treat infection is certainly preferable to an attempt at ureteroscopic
removal of the stone. The authors recommend engaging the stone in a basket
and removing it if possible and if not, breaking the stone up within the
basket. I really believe that I would not intentionally engage in a basket
a stone that I knew I could not extract and would vastly prefer to use
an intracorporeal lithotripsy to fragment the stone and then extract the
fragments. This would obviate the very difficult situation if the basket
and stone were truly unable to be extracted. As to what the preferred
method of stone destruction should be, I think it really is a matter of
personal preference, although in the United States currently the Holmium
laser is the preferred instrument for this. I realize that some authors
have counseled against the use of electrohydraulic lithotrite, but I think
if that is what one has one should use that and it certainly can be used
safely to minimize the risk of perforation of the ureter. While it is
true that pregnancy does not itself predispose to calculus formation,
the urinary stasis of pregnancy can certainly precipitate stones in women
who have a previous mild or more overt metabolic stone forming diathesis.
Often such patients have pre-existing stones and if these stones can be
identified prior to conception, it may be possible to prophylactically
remove some of these stones or to investigate the patient metabolically
and see if there is a stone forming diathesis present. Recently, Lingeman
and colleagues reported a series of patients in the Journal of Endourology
making a point similar to those made in this fine article.
I
do think that endoscopic management of these should be a matter of first
consideration in the absence of signs of infection or sepsis and congratulate
the authors on a nice contribution.
Dr.
Joseph W. Segura
Carl Rosen Professor of Urology
Mayo Medical School
Rochester, Minnesota, USA