CT-VIRTUAL
ENDOSCOPY OF THE URINARY TRACT
(
Download pdf )
ADILSON PRANDO
Department of Radiology, Vera Cruz Hospital, Campinas, São Paulo, Brazil
ABSTRACT
Objective:
To demonstrate the various applications of CT-virtual endoscopy, for the
assessment of urinary tract abnormalities
Materials and Methods: Sixty-three patients
were evaluated by CT-virtual endoscopy (49 CT-cystoscopy; 14 CT-pyeloureteroscopy).
CT-cystoscopy was obtained for follow-up of bladder tumor (n=21), radiologic
suspicion (n=12) or radiologic evidence of urinary tract lesion (n=16).
CT-pyeloureteroscopy was done due to neoplasm (n=5), calculi (n=3) and
extrinsic compressions (n=3).
Results: In 49 patients submitted to CT-cystoscopy,
27 tumors were detected intraoperatively (ranging 0.5-4.8cm). CT-cystoscopy
revealed 21 tumors (78%); all tumors larger than 0.6 cm were detected.
Tumor within a bladder diverticulum was seen by CT-cystoscopy but not
by endoscopy, in two patients. Useful additional information such as extension
of tumors into the anterior portion of the bladder neck (n=2) and adequate
characterization of bladder diverticulum in a child (n=1) was also obtained.
CT-pyeloureteroscopy detected 6 of 9 tumors (67%), and was useful in the
differential diagnosis of pelvic/ureteral tumor versus calculi (n=8) and
intrinsic versus extrinsic ureteral lesion (n=3).
Conclusion: CT-virtual endoscopy is a useful
procedure, particularly in the following situations: a)- Follow-up of
bladder tumors; b)- Complimentary evaluation of areas of difficult approach
by endoscopy; c)- Differential diagnosis of intrinsic versus extrinsic
lesion of the renal pelvis and ureter.
Key words:
urinary tract, imaging; bladder; ureter; neoplasms; diagnostic imaging;
CT, endoscopy
Int Braz J Urol. 2002; 28: 317-22
INTRODUCTION
Recently CT-virtual endoscopy has been introduced to the imaging armamentarium for use in the evaluation of urinary bladder (1-7). CT-virtual endoscopy in the evaluation of bladder (CT-cystoscopy), has been described in several studies in the literature but its utility for evaluation of the pelviocaliceal system (CT-pyeloureteroscopy), has illustrated only sporadically (8,9). Our purpose is to demonstrate the various applications of CT-virtual endoscopy, for the assessment of the abnormalities found in the bladder, pelviocaliceal system, and ureter.
MATERIALS AND METHODS
CT-cystoscopy
Was performed in 49 patients. After voiding,
a 12F Foley catheter was inserted into the bladder and residual urine
withdrawn. The bladder was then distended with 300-400mL of air. After
a scout view for adequate planning, helical CT of the bladder was then
obtained with patient in the supine and prone position (3mm in thickness,
reconstructed at 1.5mm, “pitch” 1, and 120 kV-230 MA). The data
was sent to an independent workstation for evaluation of the 2-D axial
scans and to generate intraluminal views of the bladder (CT-endoscopic
navigator system and the use of a threshold surface rendering technique).
CT-pyeloureteroscopy
This procedure was utilized as a complimentary
technique of CT-urography in 14 patients with signs of urinary tract obstruction
(dilation larger than 0.5cm). CT-urography was performed with intravenous
administration of 150mL of nonionic low osmolarity contrast agent, enabling
homogeneous, dense opacification by contrast material of the pelviocaliceal
system and ureters. Using a CT endoscopic navigator system at a computer
workstation and a 100 to 150 HU of the lower threshold and upper threshold
maximum the CT-pyeloureteroscopic images were generated .All intraluminal
navigation study was performed by the same radiologist (author). A complete
CT-cystoscopic or ureteroscopic examination, including the acquisition
and interpretation of images, required approximately 30 minutes. Images
were then correlated with surgical and pathological findings in all patients.
RESULTS
CT-cystoscopy
Forty-nine patients presenting 27 tumors
at surgery (ranging 0.5-4.8cm), were submitted to CT-cystoscopy. Twenty-one
(78%) of 27 lesions detected intra-operatively were visualized with this
technique. This procedure allowed readers to identify 21 of 21 masses
(100%) larger than 0.6cm. On the other hand, 6 lesions ranging from 0.25
to 5.5mm were missed. Our results were distributed according to their
main clinical applications:
a)- Follow-up of bladder tumor: 8 tumors
were detected in 19 patients in the follow-up for bladder cancer (Figure-1);

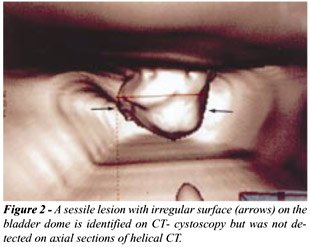
b)- Patients with hematuria presenting radiologic
suspicion or normal findings on axial CT images. In this group consisting
of 16 patients, we detected 6 tumors. Three patients showed tumor in bladder
dome and bladder base, which was not visualized in axial CT, images (Figure-2);
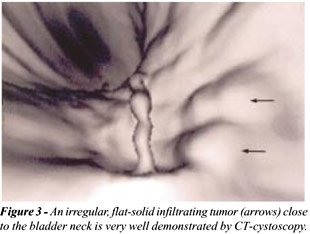
c)- Complimentary study of areas of difficult
evaluation by conventional cystoscopy. This was the indication of CT-cystoscopy
in 8 patients. Useful additional information such as extension of tumors
into the anterior portion of the bladder neck was demonstrated in 3 patients
(Figure-3);
d) Evaluation of bladder diverticulum with
small opening. Three tumors within a bladder diverticulum were seen by
CT-cystoscopy but not by endoscopy, in 2 patients (Figure-4). Adequate
characterization of bladder diverticulum in a child (n=1) was also obtained
(Hutch diverticulum);

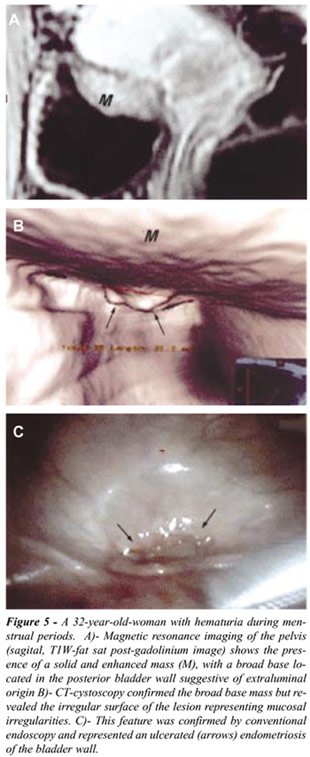
e) Differentiation between intraluminal
and extraluminal bladder wall mass: In this group, 4 tumors were identified
and in 3 patients, it was difficult to establish the origin of the bladder
mass based on conventional radiologic procedures. CT-cystoscopy accurately
demonstrated the intraluminal origin or component of the mass in these
patients by showing either a irregular surface of the lesion or the presence
of a lesion with a narrow base (Figure-5).
 |
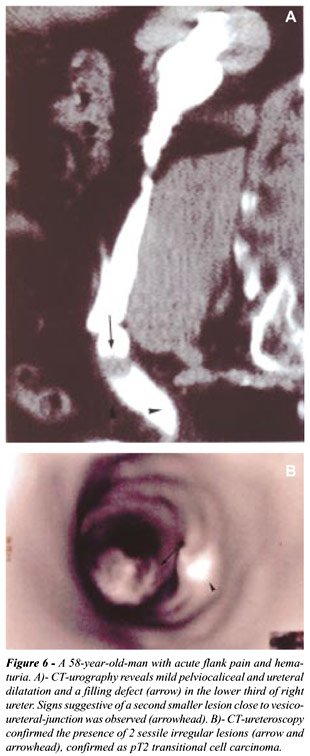 |
CT-pyeloureteroscopy
The presence of minimal dilatation was sufficient
for adequate intraluminal evaluation of the pelviocaliceal system and
ureter, which was done in 14 patients (Figure-6). In 11 of these patients,
a filling defect in the renal pelvis, or ureter, or ureteral strictures
was observed. Gross examination of 6 resected kidneys and ureters, and
3 ureters revealed 9 tumors (0.3 to 1.7cm) and 2 intrinsic, and 1 extrinsic
ureteral strictures. CT-pyeloureteroscopy detected 6 of 9 tumors (67%),
all larger than 0.4cm in diameter and was useful for the correct diagnosis
of intrinsic versus extrinsic ureteral lesions in these 3 patients and
for the demonstration of urinary calculi as the cause of the filling defects
in the remaining 2 patients.
DISCUSSION
Conventional
endoscopy plays a key role in the diagnosis of urinary tract tumors due
to its capability of detect subtle alterations in mucosal-texture and
to allow direct resection with or without mucosal biopsy.
Helical CT with its continuous acquisition
of volumetric data enables the presentation of acquired data in three-dimensional
images. CT-virtual endoscopy using surface rendering techniques enables
imaging of the interior of a hollow viscera or organ by extracting CT
numbers only from the boundary regions between the organ walls and the
contrast agent. A great difference in CT attenuation between the exterior
and lumen of the organ is necessary to generate CT endoscopic images.
For virtual cystoscopy, inflated air is used and for the CT-pyeloureteroscopy,
the high CT attenuation of the intraluminal contrast. With a CT endoscopic
navigator system in the workstation, standard axial, sagital coronal and
oblique reference images are automatically obtained. Using an appropriate
threshold level in order to avoid artificial defects, and adequate trackball
real-time angles and cut planes of the interiors of the organ of interest
are displayed. By this technique the viewpoint of the observer can be
manipulated through 360 degrees in any axis and within the bladder (CT-cystoscopy)
all the internal surface of the organ can be evaluated, particularly the
anterior bladder neck and the bladder base which are difficult areas for
the conventional cystoscopy. Other applications of CT-cystoscopy are in
patients with urethral stricture (which precludes conventional cystoscopy)
and in the follow-up of bladder tumors since its recurrence is common
mainly in cases of multifocal or high-grade lesion. In this clinical setting,
CT-cystoscopy depicted in our study all lesions larger than 0.5cm.
Since lesion on the dome or base of the
bladder can be missed in axial images (due to the limitation of Z-axis
resolution of CT), sets of axial images and intraluminal views must be
used for accurate radiologic detection of these lesions. Axial images
are essential for evaluation the extraluminal component of the tumor and
the presence of nodal metastasis. CT-virtual endoscopy offers the possibility
of evaluate the surface morphology of the lesion, this is an important
additional radiologic finding that must be reported since polypoid pedunculated
lesion is usually low grade cancer and mostly flat solid infiltrating
tumors are high grade lesions (10). CT-cystoscopy has important limitations
such as detect subtle mucosal color changes (carcinoma ”in situ”)
and impossibility to provide tissue analysis by the biopsy.
CT-pyeloureteroscopy may occasionally be
possible in normal structures, but has better results in patients with
some degree of urinary tract dilation (above 0.5cm). The use of furosemide
has been shown useful for distinguishing ureteral tumors from ureteral
strictures. Since we performed virtual endoscopy only in patients with
sufficient urinary tract dilatation, the use of furosemide, was not necessary.
With this technique, sensitivity and specificity
for detecting ureteral tumors and carcinoma were 81% and 100% respectively
(9).
We considered our clinical data set too
small to determine the overall accuracy of this method.
CONCLUSION
CT-virtual endoscopy (CT- cystoscopy, CT-pyeloureteroscopy) is not a competitive technique to conventional endoscopy of the urinary tract; on the contrary, it has been proved a useful complementary tool. CT-virtual endoscopy can be helpful for visualizing the complex morphology of urinary tract tumors (particularly lesions larger than 0.5 cm in diameter) and distinguishing tumor from calculi or from strictures. Other important application is for the differential diagnosis of intrinsic versus extrinsic lesion of the renal pelvis, ureter, and bladder. CT-virtual endoscopy is a promising and evolving technique ant its role is still to be determined, but this technique probably will have an important role in the diagnosis of urinary tract tumors because an increase number of ideal surgical candidates for uretero-nephroscopic resection will be identified.
REFERENCES
- Vining DJ, Zagoria RJ, Liu K, Stelts D: CT-cystoscopy an innovation in bladder imaging. AJR. 1996; 166: 409-10.
- Fenlon HM, Bell TV, Ahari HK, Hussain S: Virtual cystoscopy: early clinical experience. Radiology. 1997, 205: 272-5.
- Stenzl A, Frank R, Eder R, Recheis W, Knapp R, zur Nedden D, et al.: 3-Dimensional CT and virtual reality endoscopy of the reconstructed lower urinary tract. J Urol. 1998; 159: 741-6.
- Gualdi GF, Casciani E, Rojas M, Polettini E: Virtual cystoscopy of bladder neoplasms. Preliminary experience. Radiol Med (Torino). 1997; 199: 506-9.
- Song JH, Francis IR, Platt JF, Cohan RH, Mohsin J, Kielb SJ, et al.: Bladder tumors detection at virtual cystoscopy. Radiology. 2001; 218: 95-100.
- Allan JD, Tolley DA: Virtual endoscopy in urology. Curr Opin Urol. 2001; 11: 189-92.
- Bernhardt TM, Rapp-Bernhardt U: Virtual cystoscopy of the bladder based on CT and MRI data. Abdom Imaging. 2001, 26: 325-32.
- Takebayashi S, Hosaka M, Takase K, Kubota Y, Kishida T, Matsubara S: CT-nephroscopic images of renal pelvic carcinoma. J Urol. 1999, 162: 315-8.
- Takebayashi S, Hosaka M, Kubota Y, Nogushi K, Fukuda M, Ishibashi Y, et al.: CT-ureteroscopy for diagnosing ureteral tumors. J Urol. 2000; 163: 42-6.
- Bennington JL, Beckwith JB: Tumors of the Renal Pelvis and Ureter. In: Atlas of Tumor Pathology. Tumors of the kidney, Renal Pelvis and Ureter: Washington DC, AFIP, 1975, p. 24.
____________________
Received: April 24, 2002
Accepted after revision: July 29, 2002
_______________________
Correspondence address:
Dr. Adilson Prando
Av. Andrade Neves, 707
Campinas, SP, 13013-161, Brazil
Fax: + 55 19 3231-6629
E-mail: aprando@mpc.com.br