LAPAROSCOPIC
ASSISTED RADICAL CYSTOPROSTATECTOMY WITH Y-SHAPED ORTHOTOPIC ILEAL NEOBLADDER
CONSTRUCTED WITH NON-ABSORBABLE TITANIUM STAPLES THROUGH A 5 CM PFANNENSTEIL
INCISION
(
Download pdf )
SIDNEY C. ABREU, FREDERICO I. MESSIAS, RENATO S. ARGOLLO, GLAUCO A. GUEDES, MARDHEN B. ARAUJO, GILVAN N. FONSECA
Urological Hospital of Brasília (SCA, FIM, RSA, GAG) and Sections of Urology, Federal University of Ceara (MBA) and Federal University of Goias (GNF), Brazil
ABSTRACT
Introduction:
We performed a laparoscopic radical cystoprostatectomy followed by constructing
a Y-shaped reservoir extra-corporeally with titanium staples through a
5-cm muscle-splitting Pfannenstiel incision.
Surgical technique: Upon completion of the
extirpative part of the operation, the surgical specimen was entrapped
and removed intact through a 5-cm Pfannenstiel incision. Through the extraction
incision, the distal ileum was identified and a 40 cm segment isolated.
With the aid of the laparoscope, the ureters were brought outside the
abdominal cavity and freshened and spatulated for approximately 1.5-cm.
Bilateral double J ureteral stents were then inserted up to the renal
pelvis and the ureters were directly anastomosed to the open ends of the
limbs of the neobladder. Following this, the isolated intestinal segment
was arranged in a Y shape with two central segments of 14 cm and two limbs
of 6 cm. The two central segments were brought together and detubularized,
with two sequential firings of 80 x 3.5 mm and 60 x 3.5 mm non-absorbable
mechanical stapler (Multifire GIA - US Surgical) inserted through an opening
made at the lowest point of the neobladder on its anti-mesenteric border.
The neobladder was reinserted inside the abdominal cavity and anastomosed
to the urethra with intracorporeal laparoscopic free-hand suturing.
Conclusion: Although this procedure is feasible
and the preliminary results encouraging, continued surveillance is necessary
to determine the lithiasis-inducing potential of these titanium staples
within the urinary tract.
Key
words: bladder neoplasms; laparoscopy; cystectomy; urinary reservoirs;
neobladder, surgical stapling
Int Braz J Urol. 2005; 31: 362-9
INTRODUCTION
Initially
restricted to a few centers of excellence, the worldwide experience with
laparoscopic radical cystectomy is clearly on the increase (1). Nowadays,
the extirpative portion of the procedure does not represent a limiting
factor and pure laparoscopic techniques are employed to expeditiously
perform radical cystectomy and pelvic lymphadenectomy (2,3). Nonetheless,
there is a trend to perform the reconstructive procedures necessary to
create the urinary diversion extracorporeally, using conventional open
surgical technique in an attempt to reduce the overall surgical time (1).
Recently, the Italian group from Piedmont has described an “easy,
fast and reliable” technique to create an orthotopic Y-shaped ileal
neobladder open surgically using non-absorbable titanium staples (4).
Based on these promising results, we sought to perform a laparoscopic
radical cystoprostatectomy followed by the construction of a Y-shaped
reservoir extracorporeally through a 5 cm muscle-splitting Pfannenstiel
incision. Therefore maximizing the benefits of a minimally invasive approach
including, decreased postoperative pain, shorter hospital stay, quicker
recovery, better cosmesis without a significant increase in the operative
time.
Herein, we describe the surgical technique
and present our preliminary results with laparoscopic assisted radical
cystoprostatectomy with Y-shaped orthotopic ileal neobladder using non-absorbable
titanium staples.
SURGICAL TECHNIQUE
Laparoscopic
radical cystoprostatectomy was performed using a 5-port transperitoneal
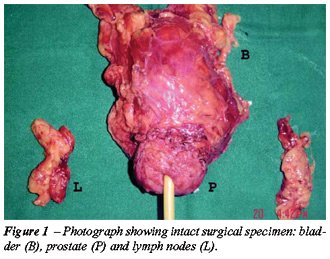
approach, which has been described in detail elsewhere (1-3). Upon completion
of this extirpative part of the operation, the surgical specimen was entrapped
in a Lapsac and removed intact through a 5-cm muscle-splitting Pfannenstiel
incision (Figure-1). Through the extraction incision, the distal ileum
was identified and brought outside the abdominal cavity. Using conventional
open surgical techniques, a 40 cm ileal segment was isolated 15 to 20
cm proximal to the ileocecal valve and a side-to-side entero-entero anastomosis
was performed to re-establish bowel continuity. Through the laparoscope,
the ureters, which were previously anchored to the anterior abdominal
wall with a stay stitch, were identified and also brought outside the
abdominal cavity. Laparoscopic viewing was used to ensure the ureters
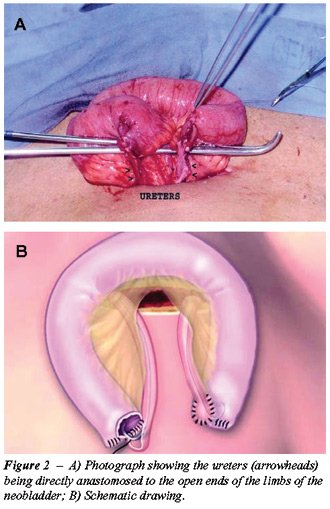
were not twisted or rotated. Subsequently, the ureters were freshened
and spatulated for approximately 1.5-cm. Bilateral, 6F double J ureteral
stents were then inserted up to the renal pelvis and the ureters were
directly anastomosed to the open ends of the limbs of the neobladder using
running sutures of 4-0 PDS (Figure-2). Following this, the isolated intestinal
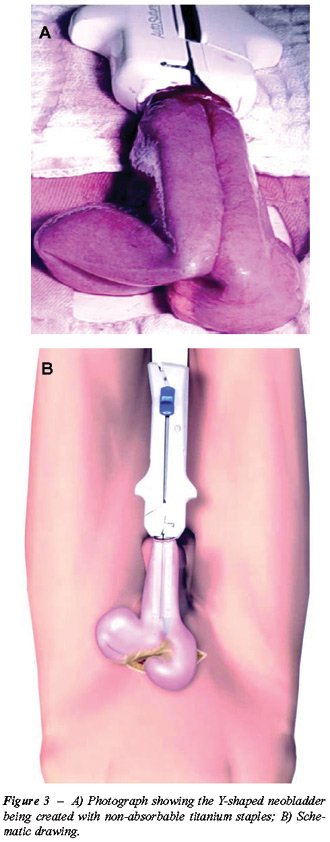
segment was arranged in a Y shape with 2 central segments of 14 cm and
two limbs of 6 cm. The 2 central segments were brought together and detubularized
with 2 sequential firings of a 80 x 3.5 mm and 60 x 3.5 mm non-absorbable
mechanical stapler (Multifire GIA - US Surgical) inserted through an opening
made at the lowest point of the neobladder on its anti-mesenteric border
(Figure-3). The recently created neobladder was reinserted inside the
abdominal cavity and the 5-cm Pfannenstiel incision was closed. Pneumoperitoneum
was re-established and the Y-neobladder was anastomosed to the urethra
with four interrupted 2-0 monocryl sutures over a 22F Foley catheter,
using intracorporeal laparoscopic free-hand suturing. The 2 limbs of the
neobladder were then fixed to the psoas muscles. A suction drain was left
in the deep pelvis.
PATIENTS
AND RESULTS
Two
male patients diagnosed with muscle invasive transitional cell carcinoma
of the bladder consented and were scheduled to a laparoscopic assisted
radical cystoprostatectomy with orthotopic Y-shaped ileal neobladder.
Metastatic workouts with chest x-rays and abdominal CTs were negative
in both patients. There were no signs of enlarged pelvic nodes. Demographic,
intraoperative and postoperative data are presented in Table-1.
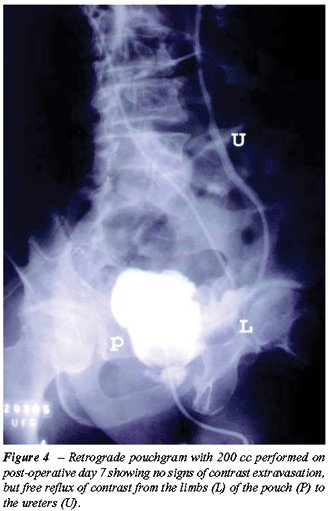
A retrograde cystogram was performed with
200 cc of contrast on postoperative day 3 and postoperative day 7 in the
first and second cases respectively, showing no signs of contrast media
extravasation (Figure-4). In both cases, bladder catheter was removed
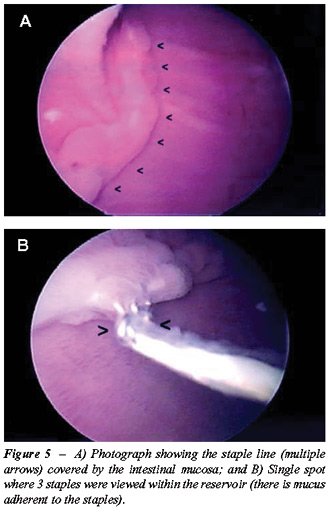
on postoperative day 21. In both cases, cystoscopic viewing in the second
postoperative month did not reveal any stones at the staple lines, which
were almost entirely covered by the intestinal mucosa, except by a single
spot where 3 staples could be visualized in the first case (Figure-5).
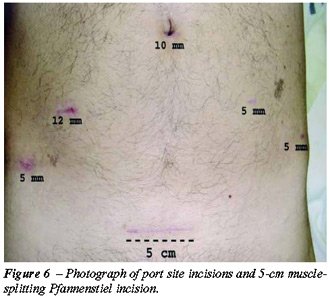
We used a smaller 5-cm Pfannenstiel incision (Figure-6) to perform the
bowel work, the Y-shaped orthotopic ileal neobladder and the ureteral
re-implantation, thus further improving cosmesis and perhaps further decreasing
surgical morbidity. Pathology revealed a T2G3 transitional cell carcinoma
(TCC) of the bladder with negative surgical margins in the first case
and a T3aG3 TCC of the bladder in the second case. Lymph nodes were negative
in both cases.
COMMENTS
Over
the past decade, a few studies have reported that the use of non-absorbable
titanium staples inside the urinary tract may be safe and secure (4-9).
The corrosive resistant nature, low toxicity and excellent tissue and
fluid biocompatibility of titanium may explain why such non-absorbable
staples are well tolerated here. In fact, in 1993, Kerbl and colleagues
from Washington University have reported the initial encouraging laboratory
and clinical data with laparoscopic stapled (titanium staples) bladder
closure (4). However, this article was criticized by reviewers at that
time, who used comments such as: “…just because it is new,
rapid and easy to use does not mean that it should be used in a cavalier
fashion;” and “… sutures are less expensive than staples
and less likely to result in stone formation.” However, in 2000
this same group discussed its follow up research conducted over a more
than 10-year period, and attesting to the safety of using non-absorbable
titanium staples to secure the bladder cuff during laparoscopic nephroureterectomy
(5), and demonstrating that no stones have ever been observed at the titanium
staple line even when the staples were not entirely covered by the vesical
mucosa.
In 2004, an Italian group from Piedmont
reported an acceptable 6% rate of stones formation when fifty Y-shaped
orthotopic ileal neobladders were created in open surgical procedures
with non-absorbable titanium staples in a mean follow up of 20 months
(total follow up range: from 8 to 47 months) (7). Encouraged by the Fontana
and colleagues study, we recently performed and documented the first orthotopic
ileal neobladder constructed totally intracorporeally using non-absorbable
titanium staples exclusively (8). Although the procedure was possible,
it took a long time (approximately 10 hours) and it required a considerable
amount of disposables (8 stapler loads) to complete it. In an attempt
to overcome these difficulties, we sought to incorporate Fontana’s
idea of creating an ileal neobladder with non-absorbable titanium staples
with the technique discussed by Basillote and colleagues of laparoscopic
assisted radical cystectomy (2). Basillote et al. have demonstrated that
when radical cystectomy is performed laparoscopically and the neobladder
is performed open surgically with conventional techniques through a Pfannenstiel
incision, the patient has the benefits of a minimally invasive approach,
including decreased post-operative pain and quicker recovery, without
a significant increase in operative time (2). Therefore, we performed
2 cases of laparoscopic assisted radical cystoprostatectomy wherein the
Y-shaped orthotopic ileal neobladder was created extracorporeally using
non-absorbable titanium staples.
Although longer follow-up is required to
fully evaluate the safety of this approach, we believe that our initial
results are encouraging. It is also worth noting the mean overall surgical
time of 5.7 hours, mean blood loss of 375 cc and mean total hospital stay
of 5 days. Moreover, over a very short period ranging from 3-7 days post-operatively,
we were able to demonstrate that there were no signs of contrast extravasation
during retrograde pouchgram performed with 200 cc of contrast. Furthermore,
cystoscopy performed in the second post-operative month did not reveal
any stones at the staple line, and only a few staples were visualized
within the neobladder while the remainder of the staple line was recovered
by the intestinal mucosa.
We differed from the technique described
by Basillote et al., who used a 15-cm Pfannenstiel incision to perform
bowel work, Studer orthotopic ileal neobladder, ureteral re-implantation
and the urethral-ileal anastomosis (2). As reported, we used a smaller
5-cm Pfannenstiel incision to perform the bowel work, Y-shaped orthotopic
ileal neobladder and ureteral re-implantation, thus further improving
cosmesis and perhaps further decreasing surgical morbidity. In our approach,
the urethral-ileal anastomosis is performed using free-hand laparoscopic
suturing after the recently fashioned neobladder is pushed back into the
abdominal cavity, the extraction incision is closed and pneumoperitoneum
is re-established.
Moreover, our approach to the bilateral
ureteral re-implantation was different from that originally described
by Fontana et al. In their report, the ureters were spatulated anteriorly
and were anastomosed to the dorsal aspect of the two limbs of the Y with
5-0 sutures using the direct (end-to-side) Nesbit technique. Subsequently,
the previously placed ureteral stents were brought out through the distal
portions of each chimney and then through the anterior abdominal wall.
In our procedure, the ureters were freshened and spatulated for approximately
1.5-cm, and then directly anastomosed (end-to-end) to the already open
ends of the 2 limbs with 4-0 sutures over previously placed double J ureteral
stents, resulting in a wide patent anastomosis. We thus avoided the presence
of external ureteral stents and did not have to close the open ends of
the limbs or create 2 new openings in the chimneys in order to implant
the ureters, thus saving some time and perhaps decreasing the chances
of developing a urinary fistula in the reservoir.
CONCLUSION
Laparoscopic assisted radical cystoprostatectomy with Y-shaped orthotopic ileal neobladder constructed using non-absorbable titanium staples through a 5-cm Pfannenstiel incision is feasible and our preliminary results are encouraging. Continued surveillance will be necessary to determine the lithiasis-inducing potential of these titanium staples within the urinary tract.
REFERENCES
- Moinzadeh A, Gill IS: Laparoscopic radical cystectomy with urinary diversion. Curr Opin Urol. 2004; 14: 83-7.
- Basillote JB, Abdelshehid C, Ahlering TE, Shanberg AM: Laparoscopic assisted radical cystectomy with ileal neobladder: a comparison with the open approach. J Urol. 2004; 172: 489-93.
- Abreu SC, Gill I: Laparoscopic radical cystectomy. In: Cadeddu J, (ed.), Laparoscopic Urologic Oncology. Totowa, New Jersey. Humana Press Inc. 2003; p. 297-304.
- Kerbl K, Chandhoke P, McDougall E, Figenshau RS, Stone AM, Clayman RV: Laparoscopic stapled bladder closure: laboratory and clinical experience. J Urol. 1993; 149: 1437-9; discussion 1439-40.
- Shalhav AL, Dunn MD, Portis AJ, Elbahnasy AM, McDougall EM, Clayman RV: Laparoscopic nephroureterectomy for upper tract transitional cell cancer: the Washington University experience. J Urol. 2000; 163: 1100-4.
- Grubb RL 3rd, Sundaram CP, Yan Y, Chen C, McDougall EM, Clayman RV: Use of titanium staples during upper tract laparoscopic reconstructive surgery: initial experience. J Urol. 2002; 168: 1366-9.
- Fontana D, Bellina M, Fasolis G, Frea B, Scarpa RM, Mari M, et al.: Y-neobladder: an easy, fast, and reliable procedure. Urology. 2004; 63: 699-703.
- Abreu, SC, Fonseca G, Gadelha JB: Laparoscopic radical cystectomy with intracorporeally constructed Y-shaped ileal neobladder using non-absorbable titanium staples exclusively. Urology. (in press), 2005.
- Abreu SC, Fonseca G, Gadelha JB: Re: Y-neobladder an Easy, Fast and Reliable Procedure. J Urol (in press), 2005.
_____________________
Received: March 3, 2005
Accepted after revision: June 10, 2005
_______________________
Correspondence address:
Dr. Sidney C. Abreu
Hospital Urológico de Brasília
SEP Sul, Q. 714/914
Ed. Sta. Maria, térreo
Phone: + 55 61 346-7004
E-mail: sidneyabreu@hotmail.com
EDITORIAL COMMENT
The
authors are to be congratulated for achieving the advanced laparoscopic
procedure of radical cystoprostatectomy. This procedure has started to
gain interest worldwide, with more institutions performing the procedure.
As with any new oncologic procedure, one must look at the outcomes in
order to assess efficacy of the procedure. The margin status must be reported
together with surveillance follow-up imaging studies. In the open cystectomy
literature, 5 year survival is 87-89% for organ confined node negative
disease compared to 50-62% for locally extravesical non-metastatic disease
(1).
The
limits of an extended pelvic lymph node dissection have been another area
of discussion. An extended lymph node dissection should include the distal
para-aortic and paracaval lymph nodes as well as the pre-sacral nodes,
known anatomic sites of lymph node drainage from the bladder. An extended
dissection may provide a survival advantage in patients with node-positive
and node-negative tumors without significantly increasing the morbidity
or mortality of the surgery (2). Recently, a multi-institutional study
reviewed their series of where positive lymph nodes were most commonly
found (3). This mapping study demonstrated positive lymph nodes were found
most commonly in the obturator spaces and adjacent to the iliac vessels.
Interestingly, 16% of lymph node metastases also included nodes above
the aortic bifurcation, whereas 8% of lymph node metastases involved the
presacral region.
Performing
the ureteral reimplantation into the neobladder extracorporeally is a
reasonable method to decrease operative time; however, one must be conscious
of avoiding excessive tension when the ureters are pulled up through the
incision, as this can lead to early strictures.
The
use of non-absorbable titanium staples to create the neobladder is a balance
between time saving maneuvers and decreasing the morbidity of the procedure.
While stones have been reported at a rate of only 6% where titanium staples
were used to construct the neobladder, one wonders if this is comparable
with the baseline stone formation rate where mucus is a nidus of stone
formation.
Clearly,
laparoscopic radical cystectomy will continue to play a role in urologic
oncology. It is currently at the infancy of institutions’ experience,
and differs from the experience of laparoscopic radical prostatectomy
in that fewer cases are performed due to the incidence of muscle invasive
transitional cell carcinoma compared to prostate cancer, as well as the
average age and health status of the patients. Longer follow-up outcome
data however is needed in order to insure optimal results.
REFERENCES
1. Stein JP, Lieskovsky G, Cote R, Groshen S, Feng AC, Boyd S et al.:
Radical cystectomy in the treatment of invasive bladder cancer: long term
results in 1,054 patients. J Clin Oncol. 2001; 19: 666-75.
2. Stein JP, Skinner DG: The role of lymphadenectomy in high-grade invasive
bladder cancer. Urol Clin North Am. 2005; 32: 187-97.
3. Leissner J, Ghoneim MA, Abol-Enein H, Thuroff JW, Franzaring L, Fisch
M, et al.: Extended radical lymphadenectomy in patients with urothelial
bladder cancer: results of a prospective multicenter study. J Urol. 2004;
171: 139-44.
Dr. Benjamin R. Lee
Laparoscopy Section, Department of Urology
Long Island Jewish Medical Center
New Hyde Park, New York, USA
EDITORIAL COMMENT
The
authors should be commended for presenting a hybrid procedure combining
a novel open technique, the Y-shaped orthotopic ileal neobladder, and
a minimally invasive laparoscopic approach. As with any hybrid procedure,
the urologist will need broad surgical skills. Urologists using this approach
must possess advanced laparoscopic skills, as they must perform a laparoscopic
cystoprostatectomy and complete the urethrovesical anastomosis laparoscopically.
Similarly, the creation of the Y-shaped neobladder requires experience
with urinary diversion, and specifically care must be taken to avoid twisting
or rotating the ureter or blood supply to the neobladder during the procedure
through the 5 cm incision.
It is evident that careful patient selection
will be critical when using this technique. Patients having prior abdominal
procedures, or with aggressive disease may be better suited to an alternative
approach. Similarly, morbidly obese patients may prove challenging, specifically
when managing the open neobladder creation through the smaller Pfannenstiel
incision. Although convalescence data and long-term follow-up are lacking,
this procedure should prove effective and beneficial. The authors diligently
state the need for long-term follow-up of the neobladder for stone disease,
although most experts would agree this would not be problematic.
In 2005, cystoprostatectomy and neobladder
creation remains an open operation in most centers, despite the fact that
many bladder cancer patients would benefit from the improved convalescence
and cosmesis of the minimally invasive approach. Moreover, a more rapid
recovery would be beneficial for bladder cancer patients requiring adjuvant
chemotherapy. This report adds nicely to the growing body of literature
supporting minimally invasive cystoprostatectomy and urinary diversion.
Dr. Stephen Y. Nakada
Professor and Chairman of Urology
University of Wisconsin
Madison, Wisconsin, USA