Cross-cultural
Adaptation of the Dysfunctional Voiding Score Symptom (DVSS) Questionnaire
for Brazilian Children
(
Download pdf )
doi: 10.1590/S1677-55382010000400009
Pediatric Urology
Adriano A. Calado, Eleazar M. Araujo, Ubirajara Barroso Jr., Jose M. Bastos Netto, Miguel Zerati Filho, Antonio Macedo Jr., Darius Bagli, Walid Farhat
Division of Pediatric Urology (AAC, EMA), Pernambuco State University, Recife, Pernambuco, Brazil, Division of Pediatric Urology (UBJ), Federal University of Bahia, Salvador, Brazil, Division of Pediatric Urology (JMBN), Federal University of Juiz de Fora, Minas Gerais, Brazil, Division of Pediatric Urology (MZF), Urology and Nephrology Institute, Sao Jose do Rio Preto, SP, Brazil, Division of Pediatric Urology (AMJ), Federal University of Sao Paulo, Sao Paulo, Brazil and Division of Pediatric Urology (DB, WF), Hospital for Sick Children, Toronto, Canada
ABSTRACT
Purpose:
To translate and culturally adapt the Dysfunctional Voiding Symptom Score
(DVSS), questionnaire into Brazilian Portuguese.
Materials and Methods: The 10-item Dysfunctional
Voiding Symptom Score (DVSS) was translated into Brazilian Portuguese
according to a standard methodology: translation, synthesis, back-translation,
Expert Committee, and pre-testing. After the translation process the final
version was pre-tested and patient responses were analyzed to identify
necessary modifications. Reliability was evaluated using the test-retest
method, and internal consistency was assessed using Cronbach’s alpha.
Results: The Cronbach’s alpha coefficient
was calculated in the test and retest phases. Internal consistency was
found to be satisfactory, as confirmed by a Cronbach’s alpha coefficient
of 0.76 for the test and 0.77 for the retest. A high degree of stability
was found in the test/retest, with an intraclass correlation coefficient
(ICC) of 0.960 (p < 0.001; 95% CI: 0.943-0.972).
Conclusions: The cross-cultural adaptation
process of the Dysfunctional Voiding Symptom Score questionnaire to be
used on Brazilian children was successfully completed following internationally
accepted methodologies.
Key
words: urinary bladder; urinary incontinence; questionnaires;
urinary tract infection
Int Braz J Urol. 2010; 36: 458-63
INTRODUCTION
Dysfunctional
voiding (DV) is a common clinical problem seen in approximately 40% of
patients presenting to the pediatric urologist (1). Females are predominantly
affected with a female-to-male ratio of 5:1 (1,2). It is characterized
by numerous symptoms, including recurrent urinary tract infections, urinary
incontinence, constipation and encopresis. It is learned behavior that
suppresses bladder contractions by inappropriately contracting the pelvic
floor muscles (external urinary sphincter) during urination. This eventually
becomes an involuntary process, resulting in functional obstruction of
the urinary stream during voiding (detrusor/external urinary sphincter
incoordination) (3).
The Standardization Committee of the International
Children’s Continence Society (4) defined dysfunctional voiding
as “over activity of the urethral sphincter during the voiding contraction
of the detrusor in neurologically normal children”. There exists
great variability in the clinical presentation of voiding dysfunction
in children. This variability translates into different approaches for
defining the problem and even treatment modalities. Although behavioral
modification remains the cornerstone of treatment, pharmacological and
biofeedback techniques have been used (5).
The various treatment outcome data published
for pediatric dysfunctional voiding are difficult to compare secondary
to the lack of a universally accepted reproducible means of reporting
symptoms and improvement. Urologists are familiar with symptom scorings.
The International Prostate Symptom Score has been widely accepted and
is currently the most popular way of grading benign prostatic hyperplasia
symptoms in men.
Farhat et al. (6) described validated symptom
scoring for wetting and functional disorders in children called the dysfunctional
voiding symptom score (DVSS). The DVSS includes 10 quantitative and qualitative
urological variables assessed by age-appropriate questions for children,
and has been used as an objective instrument to grade voiding dysfunction
in children (Appendix-1).
Since this instrument was originally written
in English and no similar validated questionnaire about this theme existed
in Brazil, a cultural adaptation was necessary.
The cross-cultural adaptation process had
to follow international guides to maintain the equivalence between the
original and target versions (7,8).
The aim of the present study was to translate
and culturally adapt the questionnaire entitled Dysfunctional Voiding
Symptom Score into Brazilian-Portuguese language.
MATERIALS AND METHODS
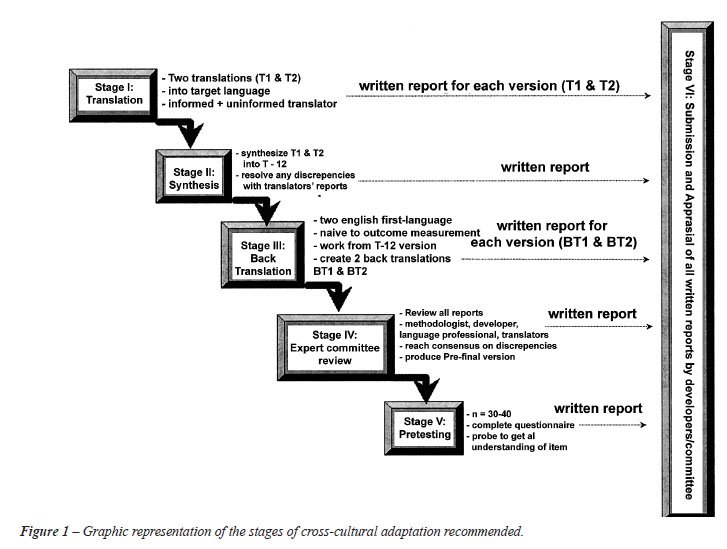
Permission to translate the DVSS into Brazilian Portuguese was obtained from one of the DVSS’s authors, Dr. Walid Farhat. The translation of this phase was carried out according to methods recommended in the literature (Figure-1). The translation of the instrument into Brazilian Portuguese was done independently by two Brazilians translators, who knew the study’s objectives. The two Portuguese versions generated one version after authors’ consensus (DVSS 1) and then, it was submitted to back-translation, done by two other translators, natives of the USA and England, who lived in Brazil, had full mastery of Portuguese and knowledge about Brazilian culture. The translators were neither informed about the study objectives, nor about the concepts involved and the goal of the instrument. The result of this phase was the DVSS version 2.
Subsequently, it that was submitted to a
committee of experts, composed of 5 pediatric urology specialists, with
English as their first language. They compared each item of the original
instrument and the translated version in relation to semantic/idiomatic
equivalences in order to assure the correct translation. Also, they had
to assure the cultural equivalence, which is related to the context and
the life experiences in Brazilian population, and conceptual equivalence,
which is the verification of the original instrument concept maintenance
in the translated version. The questionnaire items were considered as
a good agreement by the Committee only when the agreement percentage was
approximately 90%.
For the qualitative analysis, a discussion
about the judges’ suggestions was performed. The goal was to consolidate
all the versions of the instrument and indicate which characteristics
should be considered in the pre-final version. A consensus was reached
achieving semantic, idiomatic, experiential, and conceptual equivalence.
After all suggestions made by the judges, the pre-final version was developed
for field testing.
A pre-test was carried out to verify the
cultural adequacy of the instrument, and the answer “I didn’t
understand the question” was added to all of the items. Data collection
was conducted with 40 children who answered the instrument. Pre-test data
analysis showed that none of the items was above the 15th percentile of
incomprehension, which attested to the instrument’s adequacy with
no need for changes to its content or a new pre-test.
After the conclusion of the pre-test, the final Brazilian-Portuguese version
was obtained. The primary developer of the DVSS (Dr. Walid Farhat) was
informed at all stages of the translation process and approved the final
version of the questionnaire and from now on will be referred to as the
DVSS Brazilian version.
All patients who participated in this study
were asked to provide written informed consent prior to enrollment. The
full protocol received the approval of the Local Ethics and Research Committee.
The questionnaire data were recorded in
commercial statistical software (Excel/2003 for Microsoft Windows). Descriptive
statistics were used to describe the sample, to verify the content validity
of the adapted instrument, and to determine the pretest results the following
analyses were performed:
- Cronbach’s coefficient alpha: to verify reliability. Cronbach
alpha values > 0.70 were established as constituting evidence of satisfactory
internal consistency.
- Intraclass correlation coefficient (ICC): used to verify reliability
with reference to the stability of the instrument (test-retest). ICC values
= 0.90 were considered evidence of stability.
RESULTS
The
team of specialists which analyzed the translations pointed out that there
was a correspondence between the items translated, semantic equivalence
between the two translations and no translation difficulty. Adjustments
were made for the few verbal differences. Therefore, the counter-translation
compared to the original version did not did not require any changes in
grammatical structure, when the Portuguese version was translated back
into English.
In the pretest phase, the questionnaire
was answered by a sample of 40 parents of children with dysfunctional
voiding symptoms. This group was characterized by the fact that the majority
of subjects were female (80%, 32/40) with a mean age of 6.2 years. Following
application of the instrument, the patients were interviewed to evaluate
the difficulties found in filling out the questionnaire and to identify
any questions or words that were difficult to understand.
The Cronbach’s alpha coefficient was
calculated in the test and retest phases. Internal consistency was found
to be satisfactory, as confirmed by a Cronbach’s alpha coefficient
of 0.76 for the test and 0.77 for the retest. A high degree of stability
was found in the test/retest, with an intraclass correlation coefficient
(ICC) of 0.960 (p < 0.001; 95% CI: 0.943-0.972). Table-1 presents the
final version of the Brazilian DVSS.

COMMENTS
This
study provides the first adaptation into the Brazilian context of a specific
instrument for the voiding dysfunction in children. To date, there is
no consensus in the literature regarding the best strategy to perform
transcultural adaptations. The process chosen was based on the script
proposed by Guilemin et al. (8). In addition, this method has been already
successfully applied in Brazil by other researchers.
At the present time, there are a great number
of questionnaires developed on a certain culture. The process of translation
and cultural adaptation has been considered essential for comparisons
between studies from different countries, languages, and cultures. A good
linguistically accurate translation is not sufficient because items must
also be adapted culturally to preserve the conceptual meaning of the questionnaire.
The translations should be mainly evaluated
in terms of conceptual equivalence so that necessary grammatical changes
can be conceptually similar to another culture. With regard to the cross-cultural
adaptation, cultural factors such as habits and activities of a population
should be considered because an activity which is not common in a certain
population can make the instrument’s adaptation invalid. In the
present study, no obstacles were found either in the Brazilian Portuguese
language or regarding the cultural aspects which could render unviable
the applicability of the translation and the cross-cultural adaptation
of the analyzed instrument.
The cross-cultural adaptation process of
the Dysfunctional Voiding Symptom Score to Brazilian-Portuguese language
followed standardized guides: translation, synthesis, back-translation,
Expert Committee, and pre-testing (7,8).
The evaluation of the reliability showed
satisfactory internal consistency as indicated by a Cronbach’s alpha
coefficient of 0.76 for the test and 0.77 for the retest.
The changes made on the adapted version
were authorized by the author of the original instrument after previous
consultation.
After all the stages had been achieved,
the entire process of the cross-cultural adaptation was considered completed.
However, this study did not include the
assessment of measurement equivalence. Therefore, further studies should
perform this task comparing the psychometric properties of the Portuguese
version of the DVSS to those of the original instrument.
CONCLUSION
The cross-cultural adaptation process of the Dysfunctional Voiding Symptom Score questionnaire to be used on Brazilian children was successfully completed following internationally accepted methodologies.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Feldman AS, Bauer SB: Diagnosis and management of dysfunctional voiding. Curr Opin Pediatr. 2006; 18: 139-47.
- Swithinbank LV, Carr JC, Abrams PH: Longitudinal study of urinary symptoms in children. Longitudinal study of urinary symptoms and incontinence in local schoolchildren. Scand J Urol Nephrol Suppl. 1994; 163: 67-73.
- Hoebeke P, Van Laecke E, Van Camp C, Raes A, Van De Walle J: One thousand video-urodynamic studies in children with non-neurogenic bladder sphincter dysfunction. BJU Int. 2001; 87: 575-80.
- Nevéus T, von Gontard A, Hoebeke P, Hjälmås K, Bauer S, Bower W, et al.: The standardization of terminology of lower urinary tract function in children and adolescents: report from the Standardisation Committee of the International Children’s Continence Society. J Urol. 2006; 176: 314-24.
- Lordêlo P, Soares PV, Maciel I, Macedo A Jr, Barroso U Jr: Prospective study of transcutaneous parasacral electrical stimulation for overactive bladder in children: long-term results. J Urol. 2009; 182: 2900-4.
- Farhat W, Bägli DJ, Capolicchio G, O’Reilly S, Merguerian PA, Khoury A, et al.: The dysfunctional voiding scoring system: quantitative standardization of dysfunctional voiding symptoms in children. J Urol. 2000; 164: 1011-5.
- Beaton DE, Bombardier C, Guillemin F, Ferraz MB: Guidelines for the process of cross-cultural adaptation of self-report measures. Spine (Phila Pa 1976). 2000; 25: 3186-91.
- Guillemin F, Bombardier C, Beaton D: Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. J Clin Epidemiol. 1993; 46: 1417-32.
____________________
Accepted
after revision:
December 20, 2009
_______________________
Correspondence
address:
Dr. Adriano A. Calado
Pernambuco State University
Pediatric Urology Section
Rua Arnóbio Marques, 310, Santo Amaro
Recife, PE, 50100-130, Brazil
E-mail: caladourologia@yahoo.com.br