THE
MALONE ANTEGRADE CONTINENCE ENEMA (MACE) PRINCIPLE IN CHILDREN: IS IT
IMPORTANT IF THE CONDUIT IS IMPLANTED IN THE LEFT OR THE RIGHT COLON?
(
Download pdf )
KARINE F. MEYER, MAURICIO MACEDO, HUMBERTO S. FILHO, THAIS R. PINTO, LEONAN T. GALVAO, QUIRINO C. MENESES
Section of Pediatric Surgery (KFM, TRP, QCM), Hospital do Servidor Publico Estadual, Section of Pediatric Surgery (MM), Hospital Estadual Infantil Darcy Vargas (MM), Section of Pediatric Surgery (HSF), Santa Casa, Sao Paulo, SP, Brazil
ABSTRACT
Objective:
The aim of the study was to determine which was the optimal side for the
conduit to be placed (right or left colon) for antegrade continence enema
implantation.
Materials and Methods: Between July 1999
and March 2006, 31 patients underwent the construction of a catheterizable
conduit using the Malone principle (MACE) In 22 cases the conduit was
re-implanted in the right colon and in 9 cases in the left colon. There
were 20 male patients and 11 female patients, with a mean age of 10.23
years. The follow-up period varied from 3 from 83 months (average 25 months).
Right and left implantation of the conduit in the colon were compared
with regards to the presence of complications, volume of the solution
utilized, frequency of colonic lavage, time needed for performing the
enema, and degree of satisfaction.
Results: One patient with the conduit in
the right colon, using the appendix, lost the mechanism after two month
follow-up. Thirty patients remain clean and are all capable of performing
self-catheterization. No statistically significant differences were found
between the groups regarding the variables studied: complications (p =
1.000), solution volume (p = 0.996), time required (p = 0.790) and patient’s
rating (p = 0.670). The lavage frequency required for patients with the
conduit in the right colon may be lower.
Conclusion: The MACE principle was considered
effective for treating fecal retention and leaks, independent of the implantation
site. The success of this surgery appears to be directly related to the
patient’s motivation and not to the technique utilized.
Key
words: fecal incontinence; enema; surgery
Int Braz J Urol. 2008; 34: 206-13
INTRODUCTION
Different
diseases can cause intestinal dysfunction and continuous feces soiling.
And for the treatment to be adequately performed, it is of utmost importance
that a cause be found and eventually treated. Independent of its origin,
intestinal incontinence, especially when it has become chronic, could
carry significant emotional and social problems. Therefore, the management
of children with continuous fecal soiling is essential to improve quality
of life (1).
Retrograde enema was the treatment of choice
until recently when there was a major step forward made by Malone et al.
in 1990 (2) with the description of the continent cecal access for antegrade
enema. The technical procedure utilized the Mitrofanoff (3) principle
for the creation of a continent conduit with the appendix, which is easily
catheterizable from a stoma.
In cases where the appendix has previously
been removed or is required for urological use, the need to construct
a new conduit occurs. This has been achieved by utilizing a cecal flap
(4), a sigmoid flap (5) or a segment of the small intestine or colon that
has been reconfigured (6) by means of the Yang-Monti principle (7,8).
After the reimplantation of these conduits
in the left colon began, doubts emerged regarding the optimal place for
reimplanting them: the right colon or the left colon. Calado et al. (5)
believed that the left colon was the more physiologically appropriate
location, with a decrease in the risk of water absorption as well as a
decrease in the time required for enema administration and washout, thereby
increasing patient satisfaction and compliance. The enema performed in
right colon often is long and tedious for handicapped patients, as the
volume of washout from the cecum to the rectum is large, especially in
neuropathic bowels prone to dolichosigmoid (5).
The aim of the study was to determine which
was the optimal side for the conduit to be placed (right or left colon)
for antegrade continence enema implantation.
MATERIALS AND METHODS
Between
July 1999 and March 2006, 31 patients with intestinal dysfunction and
continuous feces soiling underwent the construction of a catheterizable
conduit using the MACE principle (2).
The criteria for indicating surgical treatment
were fecal incontinence not responsive to more conservative measures (dietary
modifications and medical treatment); patients who remained clean by performing
enemas via the rectal route; the patients and their parents should be
motivated to perform the antegrade enema.
There were 20 male patients and 11 female
patients, with a mean age of 10.2 years (range: 4 to 17 years). Fourteen
children had imperforate anus, twelve had myelomeningocele, three had
medullar trauma, one had spina bifida, and one had complex perineal trauma
(Table-1).
For the 22 patients with the mechanism re-implanted
in the right colon (Table-2), the conduit utilized was the cecal appendix,
which was kept in its original position and subjected to an anti-reflux
procedure consisting of suturing the walls of the cecum around the appendix.
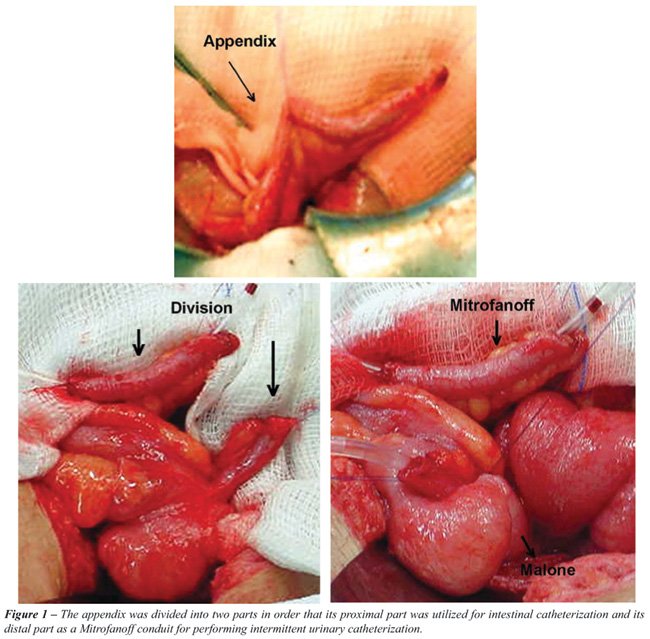
In 16 patients, this conduit was brought to the exterior at the umbilicus
and in six, at the right iliac fossa. In five of these children, the appendix
was divided into two parts (Figure-1), with concomitant division of its
irrigation, in order that its proximal part was utilized for intestinal
catheterization and its distal part as a Mitrofanoff conduit (3) for performing
intermittent urinary catheterization.
In the nine patients with reimplantation
of the mechanism in the left colon (Table-2), the conduit was constructed
by utilizing a segment of the sigmoid with its base against the mesenteric
margin (5). This was tubularized around a urethral probe and was subjected
to an anti-reflux procedure involving the walls of the sigmoid. It was
brought to the exterior at the left iliac fossa.
During the same operation, 16 patients simultaneously
also underwent other procedures:
• 10 patients: bladder enlargement,
construction of a conduit for urinary continence catheterization (Mitrofanoff
(3)) and plastic surgery on the bladder neck;
• 2 patients: construction of a conduit
for urinary continence catheterization (Mitrofanoff (3));
• 1 patient: sigmoidoplasty to reduce
its caliber;
• 1 patient: plastic surgery on the
bladder neck;
• 1 patient: reconstruction of the
intestinal transit;
• 1 patient: correction of an incisional
hernia.
Following the surgery, all the patients
were given training, in order to learn how to operate the mechanism. The
volume utilized for the enema was adjusted individually, so that it would
be sufficient for cleaning the colon, without rectal leaks during the
day. The solution used depended on the patient’s preference (tap
water for 14 patients, glycerinated solution for 13 patients and saline
solution for 4 patients).
The mean follow-up duration was 25 months
(range: 3 to 83 months).
Right and left implantations of the conduit
in the colon were compared with regard to the presence of complications,
volume of the solution utilized, frequency of enema, time needed for performing
the enema, and degree of satisfaction (the patients were asked to give
a score on a scale from 1 to 10 to rate the improvement in their quality
of life following the construction of the mechanism for performing antegrade
enema).
The quantitative variables were represented
by mean, standard deviation, median, minimum and maximum, and the qualitative
variables by absolute frequency (n) and relative frequency (%). The non-parametric
Mann-Whitney test for independent samples was applied to make comparisons
between groups of patients with regard to the variables of solution volume,
time needed and patient’s rating. Associations between the presence
of complications and the side of implantation were evaluated by means
of Fisher's exact test. The significance level was set at 0.05 (a = 5%).
RESULTS
One
patient had loss of the mechanism after two months follow-up, following
presentation of an abscess in the pathway of the appendix that evolved
with fibrosis of the conduit. Thirty patients are currently using their
conduits: 21 implanted in the right colon and nine in the left colon.
All these patients are clean and capable of performing self-catheterization
(Table-3).
Complications
No statistically significant differences
were found between the groups (p = 1.000). Six patients (27.3%) with the
conduit re-implanted in the right colon and constructed using the appendix
presented complications:
• stenosis of the stoma in the skin
(four patients);
• loss of the mechanism after two
months follow-up, following presentation of an abscess in the pathway
of the appendix that evolved with fibrosis of the conduit (one patient);
• discharge of secretions (one patient).
Three patients (33.3%) with the conduit
re-implanted in the left colon and constructed using a sigmoid flap presented
complications:
• peristomal infection (two patients);
• difficulty in probing because of
angling of the conduit, which necessitated surgical reintervention (one
patient);
Volume
of the Solution Utilized
No statistically significant differences
were found between the (p = 0.996). The patients with the conduit re-implanted
on the right side used a mean enema volume of 13.34 mL/kg. The patients
with the conduit re-implanted on the left side used a mean enema volume
of 13.35 mL/kg.
Frequency
of Enema
The patients with the conduit on the left
side required daily enema. On the other hand, the enema frequency required
for patients with the conduit on the right side may be lower, given that
six of our patients (27%) performed intestinal cleaning only on alternate
days.
Time
Needed for Performing the Enema
No statistically significant differences
were found between the groups (p = 0.790). The mean time needed for performing
the enema was 51.4 minutes (range: 30 to 60 minutes) for the patients
with the conduit constructed using the appendix and re-implanted on the
right side, and 49.2 minutes (range: 15 to 90 minutes) for the patients
with the conduit constructed using the sigmoid and re-implanted on the
left side.
Degree
of Satisfaction
No statistically significant differences
were found between the groups (p = 0.670). The patients were asked to
give a score on a scale from 1 to 10 to rate the improvement in their
quality of life following the construction of the mechanism for performing
antegrade enema. The patients with the conduit in the right colon gave
a mean score of 8.9 and the patients with the conduit in the left colon
gave a mean score of 9.2.
COMMENTS
The
MACE procedure has been used in patients with fecal incontinence caused
by chronic retention of feces, independent of its etiology, when these
patients are resistant to the medical treatment (5,6,8-10). In our study,
imperforate anus and myelomeningocele were the principal diseases presented
by the patients.
The procedure, described by Malone et al.
(2) in 1990, consists of dissection and isolation of the cecal appendix,
suture of the appendix tip into the skin as an appendicostomy, and the
implantation of the bottom of the appendix into the cecum in an antireflux
tunnel. The appendicostomy is therefore fixed in the inferior right quadrant
or in the umbilical region, therefore permitting the introduction of a
catheter to perform enemas in an antegrade direction. The original procedure
was posteriorly modified, maintaining the appendix in its original position
and fixing the cecum in the abdominal wall, thus avoiding twisting of
the conduit and reducing the time needed to perform the surgery (11).
Mouriquand et al. (6) proposed the use of
an isolated intestinal segment of ileum reconfigured using the Yang-Monti
(7,8) technique with the implantation of the conduit in the left colon.
They reported that this placement of the conduit in the left colon combined
with regular performance of enema resulted in the accumulation of feces
only in the left colon, reduced time required to perform the enema, and
increased child compliance.
Complications involving this procedure are
not rare, and the most important ones involve the stoma (12). In the present
study, when the conduit utilized was the appendix, stenosis of the skin
was the principal complication, and this was corrected by means of dilatation
or new maturation of the stoma in the skin. When the conduit utilized
was a sigmoid flap, the peristomal infection rate increased, which was
expected because of the manipulation involved in opening and suturing
colonic loops.
The volumes utilized for performing enemas
through conduits implanted on the right and left sides were similar, which
has led us to the hypothesis that the volume needed for cleaning the colon
is independent from the size of the colon, which is distally situated
from the implantation site of the conduit.
If the feces only accumulate in the left
colon as stated by Mouriquand et al. (6), one can imagine that even if
the conduit is re-implanted in the right colon, it would clear no significant
amount of additional feces from the right colon. Thus, the enema volume
required for a right-sided conduit could be similar to the volume required
for a left-sided conduit.
The enema solution chosen most often by
our patients was plain tap water, followed by glycerinated solution and
physiological solution. With these solutions, no metabolic disturbances
were observed, whereas many have been reported when the solution utilized
was phosphated.
There were no differences regarding the
time required for performing the enema. The patients took a mean time
of 50 minutes (range: 15 to 90 minutes), independent of the conduit reimplantation
site.
The patients with the conduit on the left
side required daily colon cleaning. On the other hand, the lavage frequency
required for patients with the conduit on the right side may be lower,
given that six of our patients (27%) performed intestinal cleaning only
on alternate days.
The authors consider that if the appendix
is already available, the MACE procedure can be performed with little
mobilization of the organ and the results could be as good as, if not
better, than if the conduit was re-implanted directly in the left colon.
This has the additional advantage that there is no need to use intestinal
segments to perform the catheterization conduit. The appendix should be
utilized even when urinary continence derivation is simultaneously necessary,
since the proximal appendix can be utilized for intestinal catheterization
and the distal appendix can be utilized as a Mitrofanoff conduit (3) for
performing intermittent urinary catheterization, as was done in five of
our cases, with good results.
The success of this surgery appears to be
directly related to the patient’s motivation and not to the technique
utilized. Thirty patients in this study are currently using their conduits:
21 implanted in the right colon and nine in the left colon. All these
patients are clean and are capable of performing self-catheterization.
To obtain this high rate of adherence to treatment, all the patients must
have been aware that, after the mechanism for antegrade enemas had been
constructed, a certain time was needed for adjusting the volume of liquid
to be utilized and the frequency of the enemas, until the continence they
required was obtained. Through such awareness, abandonment of the use
of the conduit was avoided.
When the patients were asked to give a rating
from 1 to 10 regarding the improvement in their quality of life following
the surgical procedure, the result was a score of 8.9 for the conduits
implanted on the right side and 9.2 for the conduits implanted on the
left side, thus showing a high satisfaction rate, independent of the implantation
site in the colon.
Fecal continence promotes independence among
children, and it improves their self-esteem and quality of life. The method
utilizing the MACE principle is relatively safe and if we have correctly
interpreted the results of this limited series, the surgical technique
should be the simplest one to perform. Moreover, our patients demonstrated
a high degree of satisfaction with the procedure independent of which
side it was implanted in.
The success of the Malone procedure seems
to depend mainly on selection of the patients. The patients and their
parents should be motivated to perform the antegrade enema as a routine
task and should be conscious that there is an adaptation period before
the expected continence is obtained. Fecal continence promotes the children’s
independence, improves self-esteem, and improves the quality of life.
The construction of colonic conduit for
antegrade enema is not the cure for fecal incontinence but could be an
optimal therapeutic option for the patients with chronic and irreversible
constipation with soiling. The surgical technique should be the simplest
one to perform and our patients demonstrated a high degree of satisfaction
with it, independent of which side it was implanted in.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Landman GB, Rappaport L, Fenton T, Levine MD: Locus of control and self-esteem in children with encopresis. J Dev Behav Pediatr. 1986; 7: 111-3.
- Malone PS, Ransley PG, Kiely EM: Preliminary report: the antegrade continence enema. Lancet. 1990; 336: 1217-8.
- Mitrofanoff P: Cystostomie continente transappendiculaire. dans le traitement des vessies neurologiques. Chir Pediatr. 1980; 21: 297-305.
- Kiely EM, Ade-Ajayi N, Wheeler RA. Cecal flap conduit for antegrade continence enema. Br J Surg. 1994: 81: 1215.
- Calado AA, Macedo A Jr, Barroso U Jr, Netto JM, Liguori R, Hachul M, et al.: The Macedo-Malone antegrade continence enema procedure: early experience. J Urol. 2005; 173: 1340-4.
- Mouriquand P, Mure PY, Feyaerts A, Morel-Journel N, Jules JA, Basset Debrousse T: The left Monti-Malone. BJU Int. 2000; 85 (suppl 4): 65.
- Yang WH: Yang needle tunneling technique in creating antireflux and continent mechanisms. J Urol. 1993; 150: 830-4.
- Monti PR, Lara RC, Dutra MA, de Carvalho JR: New techniques for construction of efferent conduits based on the Mitrofanoff principle. Urology. 1997; 49: 112-5.
- Dick AC, McCallion WA, Brown S, Boston VE: Antegrade colonic enemas. Br J Surg. 1996; 83: 642-3.
- Hill J, Stott S, MacLennan I: Antegrade enemas for the treatment of severe idiopathic constipation. Br J Surg. 1994; 81: 1490-1.
- Koyle MA, Kaji DM, Duque M, Wild J, Galansky SH: The Malone antegrade continence enema for neurogenic and structural fecal incontinence and constipation. J Urol. 1995; 154: 759-61.
- Castellan MA, Gosalbez R, Labbie A, Ibrahim E, Disandro M: Outcomes of continent catheterizable stomas for urinary and fecal incontinence: comparison among different tissue options. BJU Int. 2005; 95: 1053-7.
____________________
Accepted after revision:
April 4, 2007
_______________________
Correspondence address:
Dr. Karine Furtado Meyer
Rua Rio Grande, 551/162
São Paulo, SP, 04018-001, Brazil
Fax: + 55 11 5084-5342
E-mail: karine_meyer@uol.com.br
EDITORIAL COMMENT
The
authors have performed a review of their surgical experience with a left-
and right-sided Malone antegrade continence enema (MACE) procedure. Their
data shows no significant difference in evacuation time, continence, or
satisfaction between the two groups.
Interestingly, a significant number of patients
with a right MACE were able to irrigate only on alternate days and remain
continent as opposed to those with a left MACE. In our institution, a
right-sided MACE is nearly always our first choice when using the appendix
in its orthotopic location. A Monti-MACE can be implanted wherever it
is deemed appropriate from a vascular pedicle standpoint given the restraints
of the urinary reconstruction to be performed. A theoretical concern with
a left MACE in a myelomeningocele patient with a dilated colon would be
proximal constipation that may not be adequately treated by the enema
regimen.
Dr.
William Robert DeFoor
Division of Pediatric Urology
Cincinnati Children’s Hospital
Cincinnati, OH 45229
E-mail: bob.defoor@cchmc.org