A
NEW EXTRA-ABDOMINAL CHANNEL ALTERNATIVE TO THE MITROFANOFF PRINCIPLE:
EXPERIMENTAL AND PRELIMINARY CLINICAL EXPERIENCE
(
Download pdf )
ANTONIO MACEDO JR., TIAGO ROSITO, JESUS A. S. PIRES, RIBERTO LIGUORI, VALDEMAR ORTIZ
Department of Urology, Federal University of Sao Paulo, Unifesp, Sao Paulo, SP, Brazil
ABSTRACT
Introduction:
The appendix is the gold-standard channel for the Mitrofanoff principle
in pediatric urology, but the search for alternatives is justified considering
it may not be available or preferably used for colonic stomas (Malone
antegrade continence enema). The aim of this study is to report on technical
feasibility of a new approach for creating catheterizable channels in
a rabbit model and to present our preliminary clinical experience.
Material and Methods: We configured a tube
from two rectangular skin flaps 1x4 cm opposite each other in the middle
line of the lower inferior abdomen. The channel was anastomosed to the
bladder dome with embedding sutures to create a valvular mechanism. The
experimental study consisted of 12 rabbits, divided in 4 groups according
to the sacrifice schedule at 2, 4, 8 and 12 weeks. At 30th postoperative
day, an urodynamic evaluation was performed to record continence of the
stoma. A histological analysis of the specimens stained with hematoxylin-eosin,
Masson trichrome and Picrosirius red was also done in group 2 (sacrifice
at 4 weeks postoperatively). We used this method in 3 patients with congenital
non-neurogenic bladder disease presenting with massive residual volumes
without compliance deficits.
Result: The technique proved feasible in
all animals, 9 of 12 could be easily catheterized and underwent urodynamic
study. No stoma leakage was observed in 7 animals at high bladder pressures
(> 50 cm H20) and only 2 animals had some leakage at 40
cm H20. Urodynamics performed through the stoma showed urethral
leakage at 20 cm H20, therefore demonstrating the efficacy
of the valvular mechanism. Histological analysis confirmed good integration
between the tube and the bladder. Mean follow-up of the clinical series
(3 patients) was 7.2 months. Two patients remained continent up to 4 hours,
whereas 1 patient had some leakage after 2 hours.
Conclusion: We were able to confirm feasibility
of a new extra-abdominal channel based on the Mitrofanoff principle and
successfully reproduced the method in a clinical setting. Follow-up was
short and long term results are required before any conclusive judgment
can be made.
Key
words: bladder; children; urinary diversion; Mitrofanoff principle;
surgery
Int Braz J Urol. 2009; 35: 205-16
INTRODUCTION
The
introduction of clean intermittent catheterization (CIC) at the 70s improved
considerably the quality of life in patients with neurogenic bladder and
other end-stage bladder disease (1). The appendicovesicostomy gave patients
more comfort and autonomy, especially for those confined to a wheel-chair
or boys with urethral sensitivity (2). The appendix is the gold-standard
channel for urinary reservoirs but simultaneous need for a MACE (Malone
antegrade continence enema) procedure and urinary reconstruction forced
urologists to find alternatives to the appendix as the outlet tube. The
Yang-Monti, double Monti and Casale tubes are good options but they still
have complications and are constructed from intestinal segments, which
could be avoided when there is no need for bladder augmentation but only
a Mitrofanoff channel in the native bladder (3).
A second point of concern in urinary and
colonic continent stomas is the high incidence of stoma stricture, which
might be related to variables like the technique itself, frequency of
catheterization and presence of feces, although this latter condition
has not yet been proved (4,5). To date, a revision rate of 10-50% due
to stoma stricture has been reported in the literature.
The aim of this study was to report on technical
feasibility of a new approach for creating catheterizable channels in
a rabbit model and to present preliminary clinical results. The technique
was named RPM because they are the initials of three authors who developed
the concept (Rosito, Pires and Macedo). One possible advantage of this
method is in cases where it is necessary to create an abdominal channel
for catheterizing the native bladder without need of opening the peritoneum
to obtain the appendix or make a Yang-Monti tube thus reducing considerably
the morbidity of the treatment.
MATERIALS AND METHODS
We
selected the rabbit for this experimental model because of its practical
features, including ease of manipulation and familiarity of our group
with this model in previous experimental studies. The experimental protocol
was reviewed and approved by the Local Animal Research Committee. A total
of 12 New Zealand White Rabbits, approximately eight weeks old and a weight
of 2.5-3.0 kg were acclimated at the Experimental Research Animal Surgery
Department for one week before the procedures.
The rabbits were anesthetized intramuscularly
with ketamine hydrochloride (30 mg/kg) and xylazine (5 mg/kg), and local
anesthetic (xylocaine) was used to perform a penile block. All animals
were operated on under sterile conditions and under optical magnification
(2.5X). We made two rectangular flaps (1x4 cm) both opposite each other
in the middle line of the lower inferior abdomen (Figure-1A). The vascular
structure of both flaps was kept intact by inferior superficial epigastric
vessels and superficial iliac circumflex.
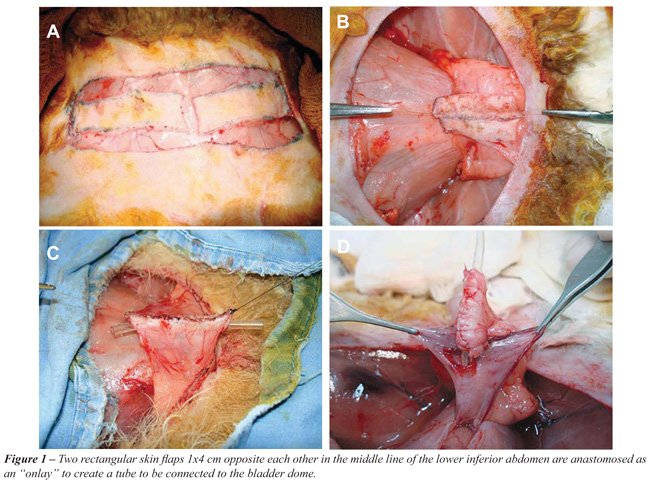
The cranial and lateral surface of the flaps
was sectioned, giving it enough mobility to allow a 90-degree rotation.
The horizontal superior border was moved to the vertical position close
to each other. A 5.0 polyglicolic acid running suture was performed configuring
a skin plate (Figure-1B). The next step consisted of an anastomosis of
the lateral margins of the flaps using a 10F plastic tube as a mold in
order to create a tube (Figure-1C).
A small abdominal incision to reach the
bladder was performed and a 0.5 cm section of the anterior wall at the
dome level of the bladder was performed (Figure-1D). The proximal end
of the tube was anastomosed to the bladder by means of 6-8 5.0 polyglicolic
acid sutures (Figures 2A and B). The continence mechanism of the channel
was done by embedding it over 3, 4.0 poliglycolic acid sutures at the
seromuscular wall of the bladder. The abdominal wall was closed in layers
and the stoma consisted of the distal end of the tube, which was adapted
to the wound margins without circular anastomosis (Figure-2C). The animals
were kept in a warm room with ventilatory support until they were well
awake. The channel mold was left intact for 7 days. The experimental study
consisted of 12 rabbits, divided in 4 groups according to the sacrifice
schedule at 2, 4, 8 and 12 weeks (groups 1 to 4 respectively).

We evaluated patency of the stoma and performed
urodynamic analysis at sacrifice (group 1) or 30th postoperative day when
animals were sedated with midazolam 0.02 mg/kg IM and a 10F plastic tube
insertion was attempted (Figure-2D). At this moment, an urodynamic evaluation
was completed using a Dynamed set, (Sao Paulo, Brazil). We catheterized
the bladder initially through the urethra using a 4F catheter for filling
the bladder and a second one via the stoma for recording bladder pressure.
A rectal catheter with a balloon was used to record abdominal pressure.
We changed the filling/recording function of catheters for subsequently
evaluating continence through the urethra and stoma. In order to better
define detrusor leak-point pressure (DLPP) through the stoma we performed
manual compression of the urethra to avoid overflow through the urethra
and created a “stress” study for the channel continence mechanism.
Detailed results are shown in Table-1 and were compared statistically
using a Chi-square analysis. Animals of group 2 were sacrificed and surgical
specimens removed, fixed in formalin and sent for histological evaluation
stained with hematoxylin-eosin, Masson trichrome and Picrosirius red.
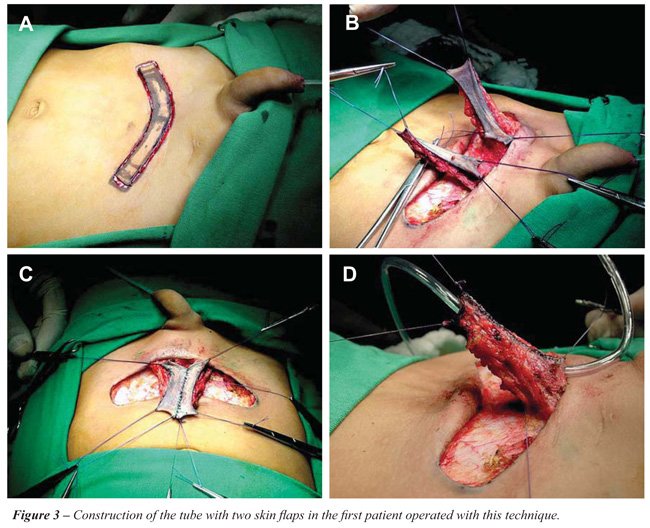
After initial experience with the experimental
model, we designed a clinical protocol and informed parents about potential
advantages of the technique, mainly to avoid opening the peritoneal space
and possible complications were also mentioned. The protocol was also
approved by local Ethics Committee. We then introduced the method in clinical
practice. We operated on three children presenting with non-neurogenic
congenital bladder abnormalities presenting with massive residual volumes
without storage deficiency. One patient had presumably primary bladder
neck obstruction (Figures 3 and 4), one had posterior urethral valve and
a third boy had prune-belly syndrome (Figure-5). Age at surgery and additional
surgical procedures are described in Table-2. A stoma catheter (12F silicone
Tube) was left indwelling for three weeks when a nurse-urotherapist trained
patients how to perform CIC. Patients were followed as outpatients every
month for at least 5 months for continence, urinary tract infection occurrence
and stoma complications.


RESULTS
Experimental:
There were minor complications related to the operative procedure in 2
cases: wound infection and partial wound dehiscence. At the sacrifice
schedule for group 1 and 30th postoperative day for other groups, animals
were examined as regards the ease of catheterization, which was possible
in 9 of 12 animals. The three failed cases included one animal with acute
stricture of the stoma due to intense inflammatory response and the two
others that developed wound dehiscence due to local infection.
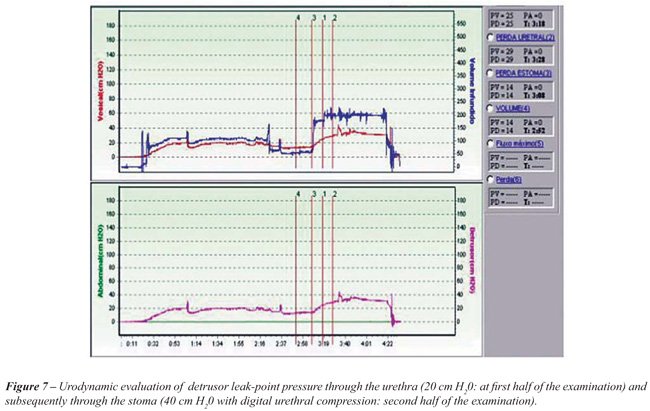
Urodynamic evaluation was performed through
both urethral and abdominal access at the same time. The detailed data
are presented in Table-1. In summary, we found no leakage through the
stoma in 7 of 9 animals reaching a detrusor pressure ranging from 60 to
110 cm H20. The two other animals had leakage at 40 cm H20.
Maximal cystometric capacity ranged from 70 to 100 mL. In order to better
evaluate the resistance pressure of the valve mechanism we had to perform
manual compression of the urethra because urodynamics performed through
a stoma catheter showed leakage at 15-20 cm H20 through the
urethra and no leakage at all through the stoma. These figures proved
efficacy of the valvular mechanism of the tube when compared mean DLPP
(or pressure at maximal capacity when no leakage occurred) in both situations
(p < 0.05). An illustration of the urodynamic curve is shown in Figure-6.
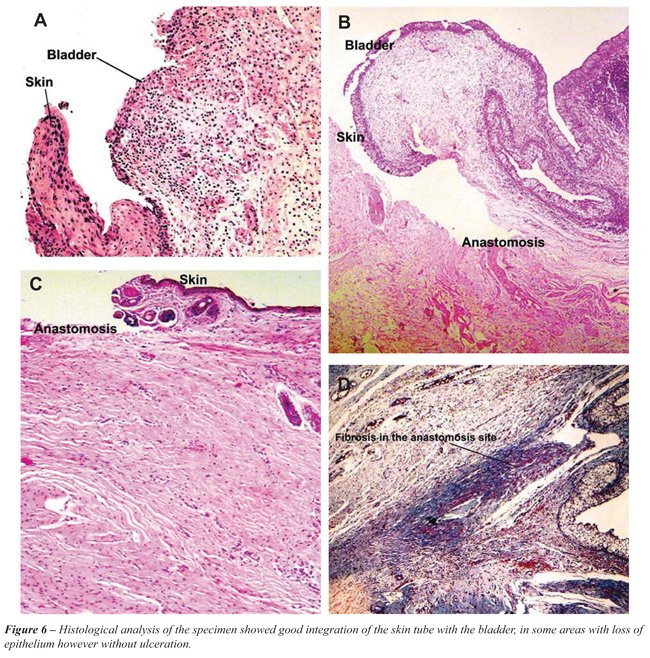
The histological analysis of the specimen
showed good integration of the skin tube with the bladder, in some areas
with loss of epithelium however without ulceration (Figure-7).
Clinical: To date, our clinical experience
of 3 patients presents good results with a mean follow-up of 7.2 months.
Two patients manage to catheterize their bladders through their stoma
4-5 times a day without urinary leakage at 4 hour intervals. One patient
(case 1) complained of painful catheterization and urinary loss after
2 hours interval between CIC after 5 months of uneventful outcome. In
two cases, the RPM channel was performed with association of other procedures:
a Cohen reflux repair and a Monfort abdominoplasty with orchiopexy.
COMMENTS
Continent
urinary diversion requires an outlet that maintains continence but allows
easy catheterization for voiding. Although none of the available options
is ideal, the appendiceal flap-valve channel first described by Mitrofanoff
appears the most reliable (1). Mitrofanoff principle is a well-established
procedure in pediatric urology and main complications reported in the
literature with this method are stoma stricture (8-39%), leakage (5-22%)
and less frequently appendix necrosis and prolapse (3). In cases where
the appendix is unavailable, ileum has been shown to be a suitable alternative.
Although some studies have reported higher stoma complication rates with
ileal catheterizable conduits, other studies have shown favorable results
(2,3).
The Yang-Monti tubes, as well as their modifications,
are the best alternative today specially for obese patients, however complications
are even higher than the classical appendicovesicostomy and they require
open access to the abdomen. This may not be a problem when bladder augmentation
is also performed, but when the main problem is abdominal access for CIC
the search for a better option is still justifiable.
The ureter has also been used to construct
a Mitrofanoff channel. However, in the studies of Van Savage et al. (4)
there was a higher risk of complications due to the need for associated
ureteral reconstruction (reimplantation or transureteroureterostomy) as
well as a greater risk of stoma stenosis.
The technique here presented based on two
lower abdominal skin flaps (RPM) could also be regarded as a valuable
alternative for continent urinary diversion, mainly because it is an extra
peritoneal approach precluding intestinal opening and anastomosis, which
theoretically could reduce clinical morbidity. A second potential advantage
is the lower risk for stoma stricture, since the two flap anastomosis
produce an “onlay” tube without circular anastomosis. If this
hypothesis proves to be correct with long term follow-up this technique
may gain acceptance especially because Thomas et al. (5) recently reported
that up to 50% of stoma strictures are treated surgically.
The inspiration for a two flap anastomosis
to obtain a tube and not simply tubularizing one flap originated from
the background of hypospadias repair that suggests that onlay repair is
superior to one circular suture in terms of stricture rate. On the other
hand, we also learned that these strictures may eventually occur with
time and at the present moment we can not predict future of the tube described
as a channel. During the peer-review process of this paper, one of the
consultants mentioned a video available at the “you tube: http://www.youtube.com/watch?v=56wNX4WKSro”
with a similar but different concept of creating a neo-urachus by tubularizing
a vertical flap of skin to communicate the bladder with the umbilicus.
To our knowledge this procedure has not yet been reported in the literature
and therefore we cannot comment on results or ethical aspects. It also
differs from our technique as a circular anastomosis is used and theoretically
more prone to stenosis or other complications.
We acknowledge that there other limitations
of our study. The presence of hair in abdominal skin, mainly in males,
could be a possible factor for producing stones. On the other hand, different
from the urethra, urine will not be in permanent contact with the luminal
surface of the tube, so we can not predict its evolution. We agree that
the tube, if continent, might have a drop of urine deposited along the
channel but mainly it is presumably only a conduit for CIC, and the role
of skin inside the tube is not predictable. Some new methods of hair deepitelization
with laser before surgery may also in the future prevent this complication,
although there are not objective data currently available, to our knowledge,
to support this procedure or its use only in selected cases after complications
due to hair inside the channel.
We also acknowledge that vascular support
of our channel, which is different from the appendix or Monti procedure
originates from superficial vessels in the skin (epigastric and circumflex
branches) so that caution should be observed in reoperations, although
it would not limit any major abdominal operation when incision is performed
above the stoma.
Our experimental data, in which an indwelling
catheter in the channel could be left for only 7 days resulted in easy
catheterization in 75% of cases (9 of 12). Histological evaluation confirmed
good integration between the skin channel and bladder. Urodynamic evaluation
confirmed efficacy of the valvular mechanism. The embedding sutures of
the bladder over the channel created at least a 40 cm H20 pressure
resistance whereas urethral resistance recorded in the study was 20 cm
H20. Our group recently published an experimental ex-vivo model
confirming efficacy of embedding sutures in creating resistance also in
intestinal reservoirs and intestinal segments (6). We also applied this
method for creating channel resistance in our concept of bladder augmentation
or substitution over the past ten years (7). Our clinical series confirmed
easy CIC in the three patients and continence with a mean follow-up of
7.2 months. Only one patient complained of pain during catheterization
after 8 months with no abnormalities.
A third intuitive advantage of the method
is the absence of wound skin anastomosis to the tube, since the tube is
only adapted to the wound. We hypothesized a possible impairment of stoma
stenosis with our method. Overall, published stoma stenosis rates vary
from 3% to 61% (8-10). Liard et al. (11) have the longest follow-up of
20 years and had stoma stenosis rates of up to 61%, compared with Horowitz
et al. (12) who only had a 3% stoma stenosis rate, however, with only
a short follow-up. Use of the cutaneous anastomosis technique with the
incorporation of U-, V- or VZ-flap may also reduce stoma stenosis (13,14),
however our method precludes any of these procedures and aesthetic aspect
is also very favorable as seen in Figures 4D and 5D.
In conclusion, we report our experimental
and preliminary experience with a new approach for extra-abdominal channel
construction based on the Mitrofanoff principle. The main advantages of
our approach are the easy of the technique, applying well-known principles
of onlay skin flap anastomosis like in hypospadia repair, minimal invasive
access (extra-peritoneal) to the bladder and no need of skin flap anastomosis
to the channel (possible impairment of stoma strictures). Long term results
are definitely required before any conclusive judgment but preliminary
results are very favorable and technical feasibility of the method could
be proved in the experimental study.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Mitrofanoff P: Trans-appendicular continent cystostomy in the management of the neurogenic bladder. Chir Pediatr. 1980; 21: 297-305.
- Cain MP, Casale AJ, King SJ, Rink RC: Appendicovesicostomy and newer alternatives for the Mitrofanoff procedure: results in the last 100 patients at Riley Children’s Hospital. J Urol. 1999; 162: 1749-52.
- Narayanaswamy B, Wilcox DT, Cuckow PM, Duffy PG, Ransley PG: The Yang-Monti ileovesicostomy: a problematic channel? BJU Int. 2001; 87: 861-5.
- Van Savage JG, Khoury AE, McLorie GA, Churchill BM: Outcome analysis of Mitrofanoff principle applications using appendix and ureter to umbilical and lower quadrant stomal sites. J Urol. 1996; 156: 1794-7.
- Thomas JC, Dietrich MS, Trusler L, DeMarco RT, Pope JC 4th, Brock JW 3rd, et al.: Continent catheterizable channels and the timing of their complications. J Urol. 2006; 176: 1816-20; discussion 1820.
- Vilela ML, Furtado GS, Koh I, Poli-Figueiredo LF, Ortiz V, Srougi M, et al.: What is important for continent catheterizable stomas: angulations or extension? Int Braz J Urol. 2007; 33: 254-61; discussion 261-3.
- Macedo A Jr, Srougi M: A continent catheterizable ileum-based reservoir. BJU Int. 2000; 85: 160-2.
- Süzer O, Vates TS, Freedman AL, Smith CA, Gonzalez R: Results of the Mitrofanoff procedure in urinary tract reconstruction in children. Br J Urol. 1997; 79: 279-82.
- McAndrew HF, Malone PS: Continent catheterizable conduits: which stoma, which conduit and which reservoir? BJU Int. 2002; 89: 86-9.
- Cain MP, Rink RC, Yerkes EB, Kaefer M, Casale AJ: Long-term follow-up and outcome of continent catheterizable vesicocstomy using the Rink modification. J Urol. 2002; 168: 2583-5.
- Liard A, Séguier-Lipszyc E, Mathiot A, Mitrofanoff P: The Mitrofanoff procedure: 20 years later. J Urol. 2001; 165: 2394-8.
- Horowitz M, Kuhr CS, Mitchell ME: The Mitrofanoff catheterizable channel: patient acceptance. J Urol. 1995; 153: 771-2.
- Kaefer M, Retik AB: The Mitrofanoff principle in continent urinary reconstruction. Urol Clin North Am. 1997; 24: 795-811.
- Clark T, Pope JC 4th, Adams C, Wells N, Brock JW 3rd: Factors that influence outcomes of the Mitrofanoff and Malone antegrade continence enema reconstructive procedures in children. J Urol. 2002; 168: 1537-40; discussion 1540.
____________________
Accepted after revision:
January 20, 2009
_______________________
Correspondence address:
Dr. Antonio Macedo Jr.
Rua Maestro Cardim, 560/215
São Paulo, SP, 01323-000, Brazil
Fax: + 55 11 3287-0639
E-mail: macedo.dcir@epm.br
EDITORIAL COMMENT
The
article by Macedo et al. in this issue of the International Braz J Urol
provides us with an interesting addition to the surgical armamentarium
for fashioning continent catheterizable abdominal channels, further expanding
the options that followed Mitrofanoff’s groundbreaking contribution.
This work provides exciting data on animal experiments that translated
into therapeutic interventions in a small, selected and somewhat heterogeneous
group of children followed-up for a relatively short period of time. Acknowledged
as a preliminary experience, the data needs to mature prior to declaring
it equivalent or superior to current techniques. The widespread acceptance
of appendicovesicostomy and bowel-fashioned conduits will now face the
challenge of options such as the RPM (Rosito, Pires and Macedo) technique,
Perovic’s genital skin flap (1) or the continent vesico-cutaneous
channel by Rackley et al. (video quoted in the Discussion section of the
article); all attractive as they appear potentially easier to perform
but characterized by a different risk/benefit profile. By virtue of avoiding
the use of bowel, problems such as internal hernias, anastomotic leaks,
mucous production and intra-peritoneal adhesions may be avoided. The trade-off
will likely be a different set of complications particularly related to
the use of skin flaps for intermittent access to bladder drainage. For
example, also borrowing from the experience with hypospadias repair, there
are specific potential problems that may be of clinical relevance, such
as those related to the development of hair follicles within the conduit
following puberty. Ultimately, comparative analyses will be needed in
order to determine if important long-term outcomes such as stomal stenosis,
strictures, leakage and difficulty catheterizing favor one technique over
the other. Only time will tell if skin proves to be a suitable alternative
to bowel tissue.
The authors are to be congratulated on following
a noteworthy pathway for innovative surgical research, by first pursuing
feasibility in an animal model prior to proceeding with surgical interventions
in children under approval by their Ethics Committee. Overall I find the
concept appealing but remain cautiously skeptical. As indicated by the
authors, the suggestion that skin based flaps are less morbid, simpler
to construct or superior to the alternatives may turn out to be true,
but there is paucity of data to categorically support or disprove this
assumption. Being the developers of the procedure, they are in prime position
to establish prospective clinical research protocols to help us answer
many of these questions. As with many other things in medicine, with experience
we may discover that patient selection is likely to play an important
role. For example, skin-based conduits may not be best for children who
undergo concomitant augmentation cystoplasty or with multiple prior surgical
interventions with incisions in areas that may compromise the blood supply
of the flaps.
I sincerely look forward to a favorable
response from the surgical community and hope that after experience with
the RPM technique grows we can enjoy the expansion of our surgical options
based on the foundations set by this elegant study.
REFERENCE
1. Perovic S: Continent urinary diversion using preputial penile or clitoral skin flap. J Urol. 1996; 155: 1402-6.
Dr.
Armando J. Lorenzo
Pediatric Urology
Hospital for Sick Children
Toronto, ON, Canada
E-mail: ajlmd@aol.com