MYCELEAL
EMPHYSEMATOUS CYSTITIS COMPLICATING A RENAL TRANSPLANT KIDNEY
(
Download pdf )
ERICH K LANG, ERNEST RUDMAN, KARL ZHANG, DANIEL THORNER, AMER HANANO
Department Radiology and Urology, SUNY Downstate Medical School, Brooklyn, New York, NY, USA
Radiology Page
Vol. 37
(2): 268-269, March - April, 2011
doi: 10.1590/S1677-55382011000200014
This
44 year old Caucasian male presented acutely ill with chills, fever and
pain over the renal allograft. The symptoms had intensified over the past
3 days. At admission his temperature was 100.8 F, pulse-rate 110/min,
BP 185/110, Hb 10.2, Hct 28, WBC 16200 (66% polymorphs). BUN 140 mg/dL,
CR 3.8 mg/dL, blood sugar 121 mg%.
The patient had a history of poorly controlled
hypertension for eight years and received a renal transplant for endstage
renal disease some 10 months ago. The postoperative period was complicated
by several episodes of LUTIs which were treated with amoxicillin and ciprofloxacin.
Two months prior to this admission the patient had been treated for acute
rejection and was still on maintenance immunosuppressive therapy. Foley
catheterization yielded only 100 mL of purulent urine; analysis revealing
60 WBC/hpf, bacteria, mycelia and debris. Urine culture grew E Coli and
identified Aspergillus Niger.
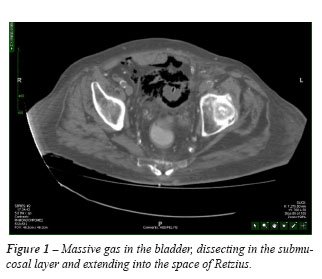
Enhanced computed tomograms revealed massive
gas in the bladder, dissecting in the submucosal layer and extending into
the space of Retzius. Debris is outlined by the gas. A shaggy mass engulfes
the tip of the Foley catheter. The mass and shaggy debris are caused by
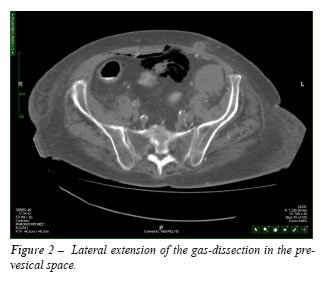
a myceliatomas (Figure-1). A CT section at a slightly higher level demonstrated
lateral extension of the gas-dissection in the pre-vesical space. It also
shows the site of implantation of the transplant ureter, which is edematous
(Figure-2). A coronal reconstruction shows the massively edematous ureter,
with some gas dissecting into the ureter (Figure-3). There is however,
still some parenchymal phase enhancement of the transplant kidney, suggesting
viability.

Open surgical drainage of the space of Retzius
was immediately undertaken. Aggressive antibiotic therapy with ciprofloxacin
and amphotericin B, parenteral, as well by infusion into the bladder was
pursued for 3 weeks. The necrotic transplant ureter was resected. The
transplant kidney was drained by percutaneous nephrostomy, ultimately
a uretero-pyelostomy, using the still intact native ureter was performed
to reestablish drainage to the bladder.
Only a few cases of emphysematous cystitis
in renal transplant recipients have been reported (1,2). The presence
of a gas-forming infection in a patient under maintenance immunosuppression
further increases the risk of emphysematous cystitis (mortality up to
20%) and calls for prompt diagnosis and aggressive surgical and medical
management (1).
REFERENCES
- Sampathkumar K, Murali TR, Sooraj YS, Mahaldar AR: Emphysematous prostatitis in renal transplant. Indian J Urol. 2007; 23: 476-8.
- Fujita S, Watanabe J, Reed AI, Hemming AW, Solis D, Netzel TC, et al.: Case of emphysematous pyelonephritis in a renal allograft. Clin Transplant. 2005; 19: 559-62.
_______________________
Correspondence
address:
Dr. Erich K. Lang
Departments of Urology and Radiology
SUNY, Downstate Health Science Center
455 Lenox Road
Brooklyn, NY, 11203, USA
E-mail: erich.lang@downstate.edu