TWELVE
CORE PROSTATE BIOPSY VERSUS SIX SYSTEMATIC SEXTANT BIOPSIES
(
Download pdf )
PAULO E. FUGANTI, M. TOBIAS-MACHADO, MARCELO A. PINTO, LUCILLA H. SIMARDI, ERIC R. WROCLAWSKI
ABC Medical School, Santo André, São Paulo, Brazil
ABSTRACT
Objectives:
We have studied patients submitted to twelve core prostate biopsy (Bx12C)
to evaluate its sensitivity in the diagnosis of prostate cancer (PCa)
as well as the addition of pathologic information when compared to those
obtained by sextant prostate biopsy (Bx6C) guided by transrectal ultrasound.
Materials and Methods: Seventy-eight men
underwent Bx12C. Transrectal ultrasound evaluated prostate volume and
guided the biopsies to the 12 following areas: right and left apex, right
and left mid prostate, right and left base, right and left transition
zone, 1 and 2 right mid-lateral and 1 and 2 left mid-lateral. The efficiency
of the Bx12C was compared to the 6 cores of the Bx6C in the same patients.
Results: Mean PSA was 17.3 ng/ml and 60
patients (77%) had abnormal digital rectal examination. The Bx12C diagnosed
28 prostate cancers (35%), adding 2 (8%) tumors (p = 0.81) and 2 (50%)
cases of prostatic intraepithelial neoplasia (PIN) to the Bx6C. The Bx12C
added 2 tumors to the 4 diagnosed by the Bx6C in the 6 patients with prostate
cancer whose prostates weighed more than 40 grams. On the other hand,
the Bx12C did not add any neoplasia (p = 0.039) in the 22 patients with
prostate cancer whose prostates weighed less than 40 grams. In PCa cases,
the additional cores increased the percentage of positive cores in 4 cases,
diagnosed bilateral PCa in 1 case, increased Gleason’s score in 1
case and added 2 cases of perineural infiltration.
Conclusions: The Bx12C does not increase
prostate cancer detection when compared to the Bx6C among patients with
high serum PSA and palpable nodule. In the patients subgroup with prostates
> 40 g, Bx12C increased the number of PCa diagnosed.
Key words:
prostate; prostatic neoplasms; diagnosis; biopsy; needle
Braz J Urol, 28: 207-213, 2002
INTRODUCTION
Traditionally,
the PCa diagnosis has been done through a transrectal ultrasound guided
prostate biopsy with 6 standardized cores (1) associated to the biopsy
of suspicious regions, such as palpable or ultrasound hypoecogenic nodules.
Some recent studies have suggested that the standard sextant biopsy (Bx6C)
lacks sensibility (2-4). Besides, prospective studies have demonstrated
that the addition of lateral cores to the Bx6C significantly increases
PCa detection (2,3).
Besides PCa diagnosis, the histopathologic
data obtained in the biopsy, such as the Gleason’s score, the presence
of grades 4 and 5, the percentage of positive cores, and presence of perineural
infiltration, are of prognostic value (5,6). The Gleason’s score
is included in category I of pathologic factors (6), considering its important
prognostic value. The tumor volume can be estimated by the number of positive
cores and by the higher percentage of tumor among the positive cores.
From the tumors with at least 1 positive core in more than 80% of their
extension, 73% are pT3, contrasting with the 18% of pT3 if the extension
is < 40% (5). The perineural via is one of the capsular infiltration
routes. Patients with perineural infiltration in the biopsy are among
the 50% of pT3 cases, versus the 25% of pT3 without this infiltration
(5). However, despite the important information revealed by the biopsy,
there are many discrepancies regarding the surgical specimen. This difference
is probably the result of an insufficient tumor sample which does not
represent the real neoplasia magnitude. It is likely that the information
obtained in the biopsy with more cores better reflects the real tumor
behavior.
We have studied patients submitted to 12-core
prostate biopsy (Bx12C) to evaluate the Bx12C sensibility in the PCa dianosis.
We have also analyzed the addition of histopathologic prognostic parameters
in patients with PCa submitted to the Bx12C when compared to the Bx6C.
MATERIALS AND METHODS
From
March to October 2000, 78 men were submitted to prostate biopsies. The
indication for the procedure was: PSA > 4 ng/ml and/or suspicious digital
rectal examination (DRE) (nodule, hardened prostate). Patients were included
in the study through a written consent and a protocol previously approved
by Research Ethics Committee of our Institution. The transrectal ultra-sonography
(TRUS) was performed with a transrectal transducer “endfire”
6.5 Mhz (Mitsubishi, Japan). The TRUS guided the biopsies and evaluated
the prostate volume (volume = 0.52 x antero-posterior diameter x sagital
diameter x transverse diameter) and the presence of nodules. The patient
was placed in lateral decubitus with inflected legs. A needle with automatic
biopsy pistol angulated 30o of the prostatic surface was used. It was
directed to the following 12 regions: right and left apex (RA and LA,
respectively), right and left mid-prostate (RM and LM, respectively),
right and left base (RB and LB, respectively) (longitudinal cut), righ
and left transition zone (RTZ and LTZ, respectively), right mid-lateral
(RML1 and RML2 – 2 cores), and left mid-lateral (LML1 and LML2 –
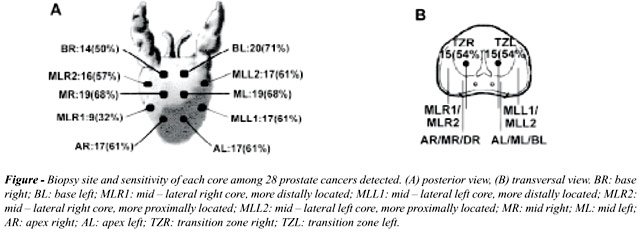
2 cores) (transversal cut), Figure.
Specimens were fixed in 10% buffered formaldehyde. Later, the material
was processed and stored in paraffin. Five-µm serial cuts were performed.
The number of positive cores for neoplasia and perineural infiltration
were verified.
The efficiency of the Bx6C and the Bx12C
was compared in the same patients. Data were analyzed through the computer
softwares Excel 97, Epi-info 5.0 and Statistica 5.0. The Student’s
t test was used to analyze parametric variables, the Mann-Whitney-U test
to analyze non-parametric variables and the Fisher and chi-square tests
were used to compare proportions.
RESULTS
Patients
with PCa were significantly older (general mean age = 69 years; patients
with PCa = 72 years and patients without PCa = 57 years; p = 0.01), with
higher PSA (general mean PSA = 17.3 ng/ml; with PCa = 24.9 ng/ml; without
PCa = 12.9 ng/ml; p = 0.001) and with smaller prostates when compared
to those patients without PCa (general mean prostate volume = 35.4 g;
with PCa = 29.3 g; without PCa = 38.8 g; p = 0.002). Regarding biopsy
indication, 8 patients (10%) presented PSA < 4 ng/ml with abnormal
DRE, 46 patients (60%) presented PSA > 10 ng/ml and abnormal DRE, and
24 patients (30%) presented PSA between 4 and 10 ng/ml, being 8 (10%)
with normal DRE and 16 (20%) with abnormal DRE. In the 18 patients with
normal DRE, the mean PSA was 15.6 ng/ml (6 - 55.2 ng/ml), being 8 (10%)
with PSA < 10 ng/ml.
The Figure shows the location of the biopsies
and the number of diagnosed PCa per each core of Bx12C. The Bx12C has
diagnosed PCa in 28 patients (35%), 2 (8%) more than the Bx6C (p = 0.81),
being 1 patient with PSA = 10.5 ng/ml, DRE unilaterally hardened, with
2 positive cores (RTZ and LTZ) and the other patient with PSA = 20.4 ng/ml,
DRE unilaterally hardened, with 1 positive core (LTZ). Any of the lateral
cores (RML1, RML2, LML1, LML2) exclusively diagnosed PCa. The perineural
infiltration was evident in 6 patients in the Bx12C.
The prostate volume of the patients with
PCa with exclusive diagnosis by the Bx12C was significantly higher than
the diagnosed by the Bx6C (58.5 g versus 27 g, p = 0.01). The Bx12C significantly
diagnosed more tumors in the prostates with more than 40 g (p = 0.039),
increasing the diagnostic sensibility in this subgroup in 50% when compared
to the Bx6C (Table-1). The Bx12C was not more efficient than the Bx6C
in the patients with lower PSA. When comparing the different biopsy strategies,
there was no significant PCa diagnostic difference between the different
models (Table-2).
Regarding the pathologic information, we
have observed that in 5 (19%) of the 26 patients with PCa diagnosed by
the Bx6C, the additional cores of the Bx12C added at least one histopathologic
information. From the 6 cases with only prostatic intraepitelial neoplasia
(PIN), 2 (33%) were only diagnosed by the Bx12C (Table-3).
DISCUSSION
The
sextant transrectal prostatic biopsy (Bx6C) is the traditional method
used in the PCa dianosis. Until the end of the 80’s, the biopsies
were directed to the nodules of the digital rectal examination and, later,
also to the ultrasound hypoecogenic nodules. In 1989, Hodge et al. (1)
directed the biopsies to 6 standard quadrants and also to hypoecogenic
areas (Bx6C). This standard identified PCa in 62% of 136 patients. In
1995, Stamey (7), after analyzing the histologic cuts of radical prostatectomies,
observed that the higher tumor volume was in the peripheral zone more
lateral to the Bx6C plane. Based on this, Eskew et al. (2) were the first
to perform biopsies with more lateral cores. They performed biopsies in
5 regions, adding 3 planes to the Bx6C, being 2 lateral and 1 median,
obtaining at least 13 cores per patient. In this study (2), the additional
regions added 35% of PCa diagnosis. After that, many studies started to
analyze the value of the lateral cores (4,8-10). Norberg et al. (8) included
lateral and transitional zone cores, observing that the Bx6C did not diagnosed
15% of the 276 PCa. Chang et al. (9) also added lateral cores to the Bx6C,
where the Bx6C and the additional cores diagnosed 76% and 80% of the 121
PCa, respectively. To compare the effect of the increase in the number
of cores without amplifying the biopsy regions, Ravery et al. (11) performed
biopsies in intermediate regions to the Bx6C. They concluded that the
10-core biopsy sensibility does not surpass the Bx6C when the regions
of the biopsy are not different. This way, the biopsy of additional regions
promotes better prostate samples. Computer programs with prostatic biopsies
simulations (4) have demonstrated that the Bx6C reaches only 65% to 72%
of the PCa. On the other hand, Naughton et al. (10) have prospectively
analyzed 244 patients submitted to 6 or 12-core prostate biopsies, observing
a similar diagnostic sensibility in the 2 groups (26% and 27%, respectively).
However, such study deserves two critics: it was designed to detect a
difference of more than 10% between the 2 groups, being smaller differences
not demonstrated with this number of patients, and the number of diagnosed
PCa by the 6 standard cores in the 12-core group was significantly smaller
that the PCa obtained in the 6-core group. The improvement in biopsy protocols
suggests, therefore, that the addition of lateral cores adds tumors to
the Bx6C in up to 35% of the cases.
In our study, even though the percentage
of detected tumors (35%) is in accordance with the other series (2,3,10),
the gain of 8% in Bx12C sensibility in relation to the Bx6C was small
when compared to the other studies. Besides, any lateral fragment (RML1,
LML1, RML2 and LML2) added neoplasia diagnosis, differently from most
studies, where lateral cores to the Bx6C are the ones which add more tumor
diagnosis (2,3,8). In our view, this difference is related to the amount
of tumor per prostate volume and the growing pattern of the peripheral
zone tumors: the bigger expansion of peripheral zone PCa occurs laterally,
in transverse direction over the posterior capsule surface and, in smaller
proportion, in the cefalocaudal direction (7). The higher the growth and
the tumoral mass, the smaller the diagnostic complementation added to
the Bx12C lateral cores. While analyzing the PCa staging in the studies
of Eskew et al. (2) and Ravery et al. (3), we observe that at least half
of them is T1c (79% and 50%, respectively), contrasting with our sampling,
where 78% of the PCaP are higher than cT1c. The same occurred with the
mean PSA in these studies (7.3 to 16.3 ng/ml) (2,3,9), where the values
were below ours (24.9 ng/ml). Such information suggests that our sampling
is composed of larger neoplasias. It is also known that the addition of
lateral cores to the Bx6C has higher efficacy in the PCa diagnosis in
subgroups with PSA < 10 ng/ml (2,3), which corresponds to only 21%
of our cases of PCa,. It is possible that the inexpressive increase in
the Bx12C diagnostic sensibility of the present study has been a result
of the larger tumor size of our patients.
As up to 25% of the prostates with cancer
present tumors in the TZ (12), there has been an effort to systematically
obtain cores from the TZ. Terris et al. (13) have demonstrated less than
5% of additional PCa diagnosis when compared to the Bx6C. In our casuistics,
the TZ cores added a 8% sensibility, which is a value very close to the
10% obtained by Kojima et al. (14). Differently from most studies, the
gain of diagnostic sensibility in our study was exclusively thanks to
the TZ cores. This inversion can be explained by the natural history of
primary neoplasias in the TZ. The extra-prostatic growth and expansion
of the TZ tumors is different from PZ, once the first are generally limited
by the compressed fibromuscular tissue of the benign prostatic hyperplasia
(BPH) (7). The PZ and prostatic capsule are rarely affected, even in large
TZ tumors (12) and high PSA. This way, the tumors located exclusively
in the TZ of our study would benefit from the Bx12C, because they would
not be included in the PZ cores even if more advanced, as supposed by
our sampling. Therefore, TZ cores would be important in high PSA casuistics.
The relationship between the prostatic volume
and PCa detection was initially studied by Uzzo et al. (15), who observed
a higher PCa detection with Bx6C in prostates < 50 g. Karakievicz et
al. (16) evaluated the Bx6C ability to diagnose PCa in prostates of different
volumes and obtained a 39.6% of PCa in prostatic volumes < 20 g and
10.1% of PCa in those between 80 and 90 g. In our study, we have also
obtained a higher detection of PCa in small prostates. Besides, the Bx12C
diagnosed additional PCa in prostatic volumes significantly higher. These
findings are in accordance with Ravery et al. (3), who has obtained better
PCa detection with the use of additional cores in prostates > 50 g.
Even though Chen et al. (17) have observed two times the number of small
volume tumors (< 0.5 ml) in prostates > 50 g when compared to the
small ones, Eskew et al. (18) have not observed any difference in tumor
volume or Gleanson’s score in tumors diagnosed by the Bx6C and their
5-region biopsy protocol. Thus, we believe that when we perform biopsies
in more regions, the larger prostates are better evaluated, with higher
chances of diagnosing an additional neoplasia with clinical relevance.
The PIN presence (high grade) in the absence
of tumor is associated with prostate adenocarcinoma diagnosis in more
than 30% of the re-biopsies (19). In our study, from the 50 patients without
PCa, 6 (12%) presented PIN. The Bx6C diagnosed 4 cases and the Bx12C added
2 more (50%). This way, the increase in the number of cores in prostate
biopsies has also an impact in the re-biopsy indication, because it allows
a better PIN diagnosis.
The additional cores have been used for
staging purposes (13). The percentage of positive cores in the biopsy
is a predictor of extra-capsular extension, seminal vesicle infiltration
and tumor volume (20), being included in prognostic factors category II
(6). Rubin et al. (5) analyzed the presence of perineural infiltration
and the percentage of core compromising in prostate biopsies of 632 patients
submitted to radical prostatectomy. They observed that the high percentage
of cancer in one core is intimately associated with the perineural infiltration,
being both associated with the pT3 stage in univariate analysis. By applying
multivariate analysis, only the percentage of core compromising in the
biopsy remained a predictor of pT3 stage. However, when these authors
(5) added pT2+ (pT2 with compromised margin) to pT3 stage, as the same
adverse pathology stage, the perineural infiltration remained a predictor
even in the multivariate analysis. This way, the perineural infiltration
and the tumor volume estimation in prostate biopsies are associated with
more advanced stages. In our study, the percentage of cores with PCa,
a estimation of tumor volume, increased the additional cores in 4 cases,
worsening its prognostic impression. The perineural infiltration, considered
a prognostic factor category III (6), was observed in 6 of our cases.
Two of them were evident only by the additional cores of the Bx12C. Besides
this information, one patient who presented a unilateral tumor in the
Bx6C presented, in fact, a bilateral one in the Bx12C. We believe that
the real value of this additional information which is obtained by the
more extensive biopsy should be re-evaluated with a larger group of patients
and in a long-term follow-up.
CONCLUSIONS
The increase in the number of prostate biopsy cores of patients with high PSA and palpable nodule did not increase the PCa diagnostic sensibility. In patients with prostates > 40 g, the increase in the number of cores substantially increased the PCa diagnosis. A higher number of cores in previously determined sites added prognostic information which better define the real tumor biological behavior.
REFERENCES
- Hodge KK, McNeal JE, Terris MK, Stamey TA: Random systematic versus directed ultrasound guided transrectal core biopsies of the prostate. J Urol, 142: 71-75, 1989.
- Eskew LA, Bare RL, McCullough DL: Systematic 5 region prostate biopsy is superior to sextant method for diagnosing carcinoma of the prostate. J Urol, 157: 199-203, 1997.
- Ravery V, Goldblatt L, Royer B, Blanc E, Toublanc M, Boccon-Gibod: Extensive biopsy protocol improves the detection rate of prostate cancer. J Urol, 164: 393-396, 2000.
- Chen MC, Troncoso P, Tang K, Babayan RJ, Johnston D: Comparison of prostate biopsy schemes by computer simulation. Urology, 53: 951-960, 1999.
- Rubin MA, Bassily N, Sanda M, Montie J, Strawderman MS, Wojno K: Relationship and significance of greatest percentage of tumor and perineural invasion on needle biopsy in prostatic adenocarcinoma. Am J Surg Pathol, 24: 183-189, 2000.
- Bostwick DG, Grignon D, Hammond MEH, Amin M, Coben M, Crawford D et al.: Prognostic factors in prostate cancer. Arch Pathol Lab Med, 124: 995-1000, 2000.
- Stamey TA: Making the most out of six systematic sextant biposies. Urology, 45: 2-12, 1995.
- Norberg M, Egevad L, Holmberg L, Sparén P, Norlén BJ, Busch C: The sextant protocol for ultrasound-guided core biopsies of the prostate underestimates the presence of cancer. Urology, 50: 562-566, 1997.
- Chang JJ, Shinohara K, Bhargava V, Presti JC: Prospective evaluation of lateral biopsies of the peripheral zone for prostate cancer detection. J Urol, 160: 2111-2114, 1998.
- Naughton CK, Miller DC, Mager DE, Ornstein DK, Catalona WJ: A prospective randomized trial comparing 6 versus 12 prostate biopsy cores: impact on cancer detection. J Urol, 164: 388-392, 2000.
- Ravery V, Billebaud T, Toublanc M, Boccon-Gibod L, Hermieu JF, Moulinier F et al.: Diagnostic value of ten systematic TRUS-guided prostate biopsies. Eur Urol, 35: 298-303, 1999.
- McNeal JE, Redwine EA, Freiha FS, Stamey TA: Zonal distribution of prostatic adenocarcinoma: correlation with histologic pattern and direction of spread. Am J Surg Pathol, 12 : 897-906, 1988.
- Terris MK, Pham TQ, Issa MM, Kabalin JN: Routine transition zone and seminal vesicle biopsies in all patients undergoing transrectal ultrasound guided prostate biopsies are not indicated. J Urol, 157: 204-206, 1997.
- Kojima Y, Nonomura N, Nose T, Inoue T, Tsuda K, Narumi Y et al.: Transition zone biopsy in the detection of prostate cancer. Eur Urol, 37: 675-679, 2000.
- Uzzo RG, Wei JT, Waldbaum RS, Perlmutter AP, Byrne JC, Vaughan ED: The influence of prostate size on cancer detection. Urology, 46: 831-836, 1995.
- Karakiewicz PI, Bazinet M, Aprikian AG, Trudel C, Aronson S, Nachabe M et al: Outcome of sextant biopsy according to gland volume. Urology, 49: 55-59, 1997.
- Chen MC, Troncoso P, Johnston DA, Tang K, Babayan RJ: Prostate cancer detection: Relationship to prostate size. Urology, 53: 764-768, 1999.
- Eskew LA, Woodruff RD, Bare RL, McCullough DL: Prostate cancer diagnosed by the 5 region biopsy method is significant disease. J Urol, 160: 794-796, 1998.
- Davidson D, Bostwick DG, Qian J, Wollan PC, Oesterling JE, Rudders RA et al.: Prostatic intraepithelial neoplasia is a risk factor for adenocarcinoma: predictive accuracy in needle biopsies. J Urol, 154: 1295-1299, 1995.
- Peller PA, Young DC, Marmaduke DP, Marsh WL, Badalament RA: Sextant prostate biopsies: a histopathologic correlation with radical prostatectomy specimens. Cancer, 75: 530-538, 1995.
_________________________
Received: December 4 , 2001
Accepted after revision: March 28, 2002
_______________________
Correspondence address:
Dr. Paulo E. Fuganti
Rua Jaguaribe, 102 / 13
São Paulo, SP, 01224-000, Brazil
Fax: + + (55) (11) 223-0886
E-mail: paulo_fuganti@uol.com.br