LAPAROSCOPIC
PARTIAL NEPHRECTOMY: A PROCEDURE IN EVOLUTION
(
Download pdf )
KENNETH OGAN, JEFFREY A. CADEDDU
The Clinical Center for Minimally Invasive Urologic Cancer Treatment, Department of Urology, University of Texas Southwestern Medical Center at Dallas, Dallas, Texas, USA
ABSTRACT
Laparoscopic
partial nephrectomy (LPN) was initially described in an animal model,
and subsequently performed in a patient with pyelonephritis and stone
disease in 1992. In an effort to decrease operative morbidity and improve
laparoscopic hemostasis, numerous investigators have developed several
techniques to facilitate the procedure. This article will outline the
various techniques that are currently performed clinically, are in development,
and also discuss the possibilities being developed for the future.
The main techniques described and discussed
are: Pure Laparoscopic Nephrectomy (duplication of open surgery), Cable-tie
Tourniquet, Double-loop Renal Tourniquet, Endosnare, Hand-assisted Laparoscopic
Partial Nephrectomy, Ultrasonic Shears, Radiofrequency Coagulation, Hydro-jet,
Microwave and Holmium laser.
In conclusion, it must be emphasized that
for a procedure to be performed laparoscopically it must be demonstrate
that the laparoscopic approach has the same or better efficacy with decreased
morbidity when compared to open surgery. This is evident to laparoscopic
radical nephrectomy. Whether the same will hold true for laraposcopic
partial nephrectomy (LPN) has yet to be determined. Thus far, the reported
techniques have demonstrated success in animal models and in small clinical
series. As a result, LPN is certainly an efficacious procedure applicable
in many cases. Nevertheless, LPN will not replace open partial nephrectomy
for many tumors.
Key words:
kidney; laparoscopy; partial nephrectomy; kidney neoplasms
Braz J Urol, 28: 184-191, 2002
INTRODUCTION
Laparoscopic
nephrectomy for the treatment of renal tumors has gained widespread acceptance
since its introduction by Clayman et al. in 1990 (1). At the same time,
the indications for open nephron-sparing surgery have expanded, as the
long-term results are similar to radical nephrectomy. However, laparoscopic
partial nephrectomy has not enjoyed similar popularity because of the
problems associated with parenchymal hemostasis and the risk of urinary
leakage incurred during this procedure (2).
Laparoscopic partial nephrectomy (LPN) was
initially described in an animal model, and subsequently performed in
a patient with pyelonephritis and stone disease in 1992 (3,4). Subsequently,
McDougall et al. initially reported a high complication rate (50%) and
open conversion rate (33%) (5). In an effort to decrease operative morbidity
and improve laparoscopic hemostasis, numerous investigators have developed
several techniques to facilitate the procedure. This article will outline
the various techniques that are currently performed clinically, are in
development, and also discuss the possibilities being developed for the
future.
TECHNIQUES
Pure Laparoscopic
Nephrectomy (Duplication of Open Surgery)
As evident from the numerous laparoscopic
techniques reviewed, there is no consensus concerning the optimal method
for obtaining hemostasis laparoscopically. This is in opposition to the
open procedure where renal hilar clamping, in situ hypothermia, and suturing
of transected vessels and the collecting system is the standard protocol.
These principles have been avoided in the laparoscopic procedure because
of the difficulty in performing these maneuvers laparoscopically. Gill
et al. (6) duplicated the open surgical principles in a series of 36 patients
who underwent LPN. In this report the kidney was approached either retro-
or transperitoneally and fully mobilized to gain access to the renal hilum.
The renal artery and vein were clamped and ice-slush hypothermia was utilized
as necessary. The renal mass was then resected along with a rim of normal
parenchyma using a monopolar hook electrode. Intracorporeal free-hand
suturing was used for repairing the collecting system and for obtaining
hemostasis. Parenchymal defects were reconstructed using surgical bolsters
and mattress sutures. Mean operative time was 2.9 +/- 1.1 hours, warm
ischemia was 20.5 +/- 6.5 minutes, and blood loss was 237 +/- 291 ml.
Complications included transfusion [1], atelectasis [1], and atrial fibrillation
with a transient rise in serum creatinine [1]. Any patient developed urine
leak. The authors acknowledged the point that facility with laparoscopic
suturing is essential for this technique. No doubt the laparoscopic surgeon
must be adept at laparoscopic suturing to successfully perform the technique
of Gill et al (6). In fact, Winfield & Kozlowski (7) have stressed
that duplicating open partial nephrectomy techniques is very difficult
and will limit widespread application of LPN. As a result, several investigators
have developed alternative novel techniques to facilitate LPN.
Cable-tie
Tourniquet
Cable-tie compression to facilitate partial
nephrectomy and minimize bleeding was first attempted by Clayman et al.
in 1993 (8). Recent modifications by Cadeddu et al. (9) have resulted
in the development of a successful technique.
The initial case reported by Cadeddu &
Corwin involved a man with a 3 cm left upper pole renal mass (10). The
procedure was performed transperitoneally with 4 ports. The perinephric
fat overlying the tumor was sent for pathological evaluation and the entire
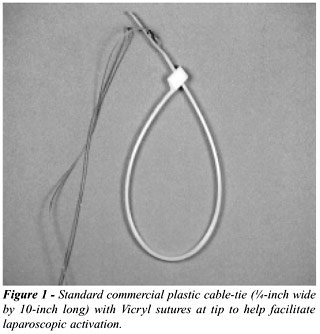
upper pole was exposed circumferentially. A 1/4 - inch wide, 10 - inch
long standard commercial plastic cable-tie (Figure-1) was gas sterilized,
engaged in a loop and laparoscopically positioned around the upper pole
above the hilum and below the tumor. The cable tie was then slowly tightened
(ratcheted) until the upper pole above the cable tie became ischemic.
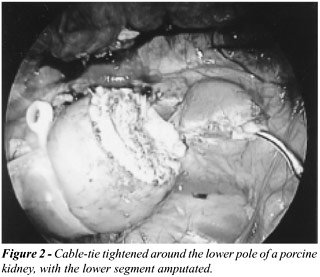
The tumor along with a margin of normal renal parenchyma was then rapidly
excised using laparoscopic scissors (Figure-2, in porcine model). Bleeding
was kept to a minimum ooze by the cable tie and no violation of the collecting
system was noted. The argon beam coagulator along with 2 layers of fibrin
glue and oxidized cellulose were then utilized to seal the parenchymal
surface. The cable tie was then cut with ultrasonic shears and removed.
The tumor specimen was extracted in a sack and the procedure was completed
in the standard fashion.
The warm ischemic time to the upper pole
above the cable tie was 12 minutes. The total operative time was 3.5 hours
and blood loss was less than 100 cc. The patient was discharged to home
on postoperative day 3 and returned to normal activity 3 weeks later.
The final histopathological analysis confirmed renal cell carcinoma with
negative margins.
Performed in an additional 2 patients, this
technique provides a reliable means of preventing the hemorrhage associated
with LPN while avoiding hilar occlusion. The cable-tie is easy to manipulate
laparoscopically and is extremely low in cost. The ischemic time is not
only short, but is confined to the parenchyma that is to be resected only.
Thus, the remaining kidney remains perfused during the procedure avoiding
potential acute tubular necrosis associated with warm ischemia. Another
benefit is that this method provides an intact pathological specimen for
examination. The obvious disadvantage is that a margin of normal parenchyma
between the tumor and hilum is necessary thereby restricting the technique
to polar lesions.
Double-loop
Renal Tourniquet
Similar to a cable-tie, Gill et al. (11)
developed a novel double loop renal parenchymal tourniquet to aid with
hemostasis during open and LPN. This device also provides for laparoscopic
circumferential pressure around the kidney during partial nephrectomy
and is limited to polar lesions. The apparatus consists of 2 U-shaped
tapes that are introduced into the abdomen via a 17F-introducer sheath.
One of the loops is used to stabilize the kidney, while the other loop
is “double-looped” around the kidney and cinched tight to afford
hemostasis. The parenchymal resection is accomplished by standard techniques.
With the excellent hemostasis attained by the hemostatic loop compression,
the minimal residual bleeding is controlled with the argon beam, electrocoagulation,
or suture ligatures.
This technique has been employed in 5 open
and 1 LPN to date (12). The renal tourniquet not only provided adequate
hemostasis, but it also allowed for facile laparoscopic positioning of
the kidney within the double looped sling. Though promising, this device
is not available, as it requires fabrication and industry cooperation
to manufacture.
Endosnare
Similar to the tourniquet techniques, Clayman
et al. (13) have developed a unique electrosurgical snare electrode in
combination with an electrosurgical generator for LPN. To date this has
been successfully evaluated in the porcine model only. In their study
the snare was compared to two different established ultrasound dissectors.
A total of 12 pigs were randomized to undergo lower pole LPN with either
the Cavitron Ultrasonic Surgical Aspirator (CUSA), the harmonic scalpel
(HS), or the electrosurgical snare electrode (ESE). The electrosnare loop
was placed around the lower pole of the right kidney and cinched tightly.
With the generator set on forced autocoagulation at 60W and endocut of
120W, the wire was pulled through the kidney until the lower pole was
completely excised.
When compared to the two ultrasound dissectors,
the electrosurgical dissector was found to be significantly faster and
associated with less intraoperative bleeding. However, the argon beam
electrocoagulator was necessary in certain cases to control persistent
oozing from the cut parenchymal surface. Retrograde pyelograms performed
at six weeks in the endosnare group revealed no evidence of extravasation.
Also, histological analysis of the resected specimens demonstrated better
preservation of the cellular architecture than with the electrosurgical
dissector. Successful clinical application has yet to be reported. The
St. Louis group recently modified the snare (14) and anticipates clinical
evaluation soon.
Hand-assisted
Laparoscopic Partial Nephrectomy
The endosnare, renal tourniquet, and cable-tie
mimic manual compression of the kidney parenchyma used during open partial
nephrectomy. Only hand-assisted LPN recapitulates this open surgical technique
as the surgeon’s hand is in the operative field. Originally, hand-assisted
laparoscopy was touted as a technique to help those learning the skills
of laparoscopy. Recently, however, skilled laparoscopists have used hand-assisted
laparoscopy in order to perform more complex procedures that would not
be possible with purely laparoscopic techniques.
Shickman et al. (15) describe the use of
the hand-assist device to facilitate LPN in 11 patients. The dissection
of the renal hilum and manual compression of the renal parenchyma was
performed via the hand-assist port. The incision of the renal parenchyma
was performed with the harmonic scalpel to minimize bleeding. Residual
bleeding was controlled with the argon beam electrocoagulator in combination
with numerous hemostatic agents. All cases were completed laparoscopically
without need for open conversion or blood transfusion.
The question is whether the abdominal incision
necessary for using the hand-assist device decreases the benefits afforded
by a purely laparoscopic approach. Wolf et al. compared 21 patients who
underwent either a purely laparoscopic versus a hand-assisted nephrectomy
(16). They found that the hand-assisted group had a shorter operating
room time and decreased major complications, with similar pain scores,
hospital stay, and convalescence. Thus, they concluded that for laparoscopic
nephrectomy, hand assistance improves operative speed and safety while
not sacrificing the benefits of a minimally invasive technique. However,
the hand incision is cosmetically unappealing as most specimens are only
2-3 cm in diameter.
Ultrasonic Shears
When first introduced, the potential of
ultrasonic shears to facilitate LPN was exciting. The instrument, which
consists of a titanium blade that vibrates at a rate o 55,000 Hz, simultaneously
cuts and coagulates tissue. Jackman et al. (17) studied the ability of
the Harmonic scalpel (LaparoSonic Coagulating Shears; Ethicon Endo-Surgery,
Cincinnati, OH) to perform LPN in the porcine model. Thirty peripheral
wedge biopsies, upper or lower-pole partial nephrectomies, or heminephrectomies
were performed. The quality of hemostasis was assessed with a constructed
“hemostasis score”. While the harmonic scalpel was found to
be adequate for peripheral wedge biopsies, supplemental coagulation was
needed in 25% of animals having a polar resection, and uncontrollable
bleeding was encountered with heminephrectomy. Therefore, the size of
the resection did predict the ability to maintain hemostasis, and the
authors recommended that the harmonic scalpel was inadequate for controlling
bleeding during a large parenchymal resection.
Harmon et al. (18) recently described their
experience with a series of 15 patients undergoing LPN primarily with
the ultrasound shears for renal parenchymal resection and hemostasis.
Once the resection was completed, a piece of oxidized cellulose was welded
with the argon beam electrocoagulator to the resection margin to prevent
against future bleeding. They reported no major complications, and concluded
that this technique was reliable. Conversely, Janetschek et al. (19) incurred
excessive bleeding in one patient where they used the ultrasonic shears
and thereby did not recommend its routine use.
Radiofrequency
Coagulation
Radiofrequency energy along with other tissue
destructive techniques (i.e.: cryosurgery) has been used for the minimally
invasive in-situ management of small renal tumors. The major shortcoming
of these techniques is the lack of a surgical specimen for pathological
diagnosis. Therefore, rather than just ablate in-situ, Corwin et al (9)
utilized radiofrequency energy to coagulate a renal mass and a margin
of normal renal parenchyma prior to laparoscopic resection. The radiofrequency
energy minimized the problems with hemostasis, while the LPN still provided
a specimen for pathological analysis.
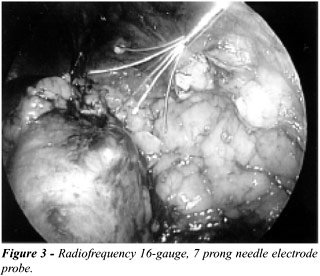
Gettman et al. (20) recently reported on
their series of 10 patients that underwent radiofrequency coagulation-assisted
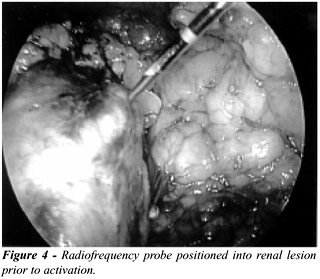
LPN. Under direct vision, a radiofrequency needle electrode (Figure-3)
was percutaneously positioned into the laparoscopically exposed renal
mass (Figure-4). The tines of the radiofrequency probe were deployed at
least 1 cm beyond the tumor to coagulate the tumor and a margin of normal
parenchyma. Using either laparoscopic scissors or ultrasound shears, the
renal lesion was then excised along with a 0.5 - 1.0 cm margin of normal
parenchyma. As there was only minimal bleeding during excision, the cut
surface was treated with additional hemostatic agents only as necessary.
The mean resection size was 2.1 cm (1-3.2 cm) while the mean operative
time was 170 minutes with an estimated blood loss of 125 cc. There were
no intraoperative or immediate perioperative complications. Importantly,
radiofrequency coagulation did not preclude accurate histological analysis
of the specimen.
Hydro-jet
An innovative and promising technique is
the use of the Hydro-Jet, which utilizes an ultra-coherent stream of water
that functions like a sharp knife. The Hydro-jet generator and dissection
probe has been mainly utilized in liver, corneal, and neurological surgery
(21-23). It has been successfully applied during laparoscopic liver resections
and cholecystectomies (24). The novel advantage of this technology is
the selective cutting of parenchyma while sparing large blood vessels
and bile ducts.
Shekarriz et al. first describe its use
in laparoscopic partial nephrectomies in the porcine model (25). Ten partial
nephrectomies were performed in 5 pigs using a Muritz 1000 (Euromed Medizintechnik,
A. Pein, Schwerin, Germany) Hydo-Jet generator. The kidney was laparoscopically
exposed and hilar vessels were identified and dissected free using the
Hydro-Jet. Once exposed, vessel loops were placed around the renal vessels
and the kidney was cooled with cold water. At a setting of 30 atm, the
Hydro-jet was then used to incise the renal capsule and cut through the
renal parenchyma. The Hydro-jet preferentially cut the parenchyma leaving
the intrarenal vessels and collecting system intact. Large vessels were
then clipped and divided under direct vision. Minimal residual bleeding
was easily controlled with electrocoagulation. Hydro-jet LPN was successful
in all of the animals with no conversions to open surgery. The mean dissection
time and warm ischemia time was approximately 45 minutes and 17 minutes,
respectively. These promising results have yet to be duplicated clinically.
Nevertheless, despite the capital expense associated with this device,
this technique, in principle, is promising.
Microwave
Most recently there has been a report by
Yoshimura et al. (26) on a small series of patients who underwent LPN
with a microwave tissue coagulator. This energy form has been used previously
during partial hepatectomy to control hemorrhage (27) and has been applied
in open partial nephrectomy for renal cell carcinoma (28). Microwave cautery
has been shown to coagulate vessels up to 3 to 5mm. in diameter (29).
Yoshimara et al. employed the microwave
coagulator in six patients with peripheral exophytic renal masses ranging
form 11 to 25 mm in size (26). Once the renal lesion was exposed and visually
identified, its boundaries were confirmed with laparoscopic ultrasound.
The resection edge was then circumferentially marked with electrocautery
and microwave tissue coagulation was performed with a Microtaze OT-110M
(Azwell Inc., Osaka, Japan) microwave generator and a needle type monopolar
applicator. The renal parenchyma was punctured with the microwave probe
along the resection line at 5 to 8 mm intervals. Depending on the size
of the lesion, there were 5 to 23 coagulations performed at 70 to 75W
for 40 to 45 seconds per session, followed by 15 seconds of dissociation.
The tumor was subsequently resected with endoscissors along the coagulated
zone without need for renal pedicle occlusion.
Mean operative time was 186 minutes (range
131 to 239) and blood loss was minimal in all cases (less than 50 ml.).
There were no major complications and time to full convalescence ranged
from 7 to 25 days (median 9). Five of the six patients had negative surgical
margins. The one patient with a positive frozen section underwent further
laparoscopic resection. As with other techniques, the authors note that
this procedure should only be used in small lesions (3 cm) in favorable
locations.
Holmium
Laser
The holmium laser has become an integral
tool in the urologist’s armamentarium for the treatment of urolithiasis
(laser lithotripsy), urethral and ureteral strictures (incision), and
benign prostatic hyperplasia (transurethral laser prostatectomy). The
holmium: YAG laser is a pulsed laser with the ability to cut and ablate
tissue on contact and also coagulate bleeding by defocusing the laser.
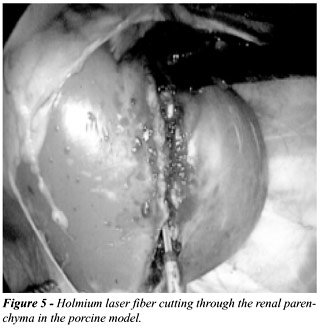
Recently, Lotan et al. (submitted for publication) investigated the use
of the holmium/YAG laser for LPN in six pigs. Without hilar occlusion,
at 0.2 joules and 60 pulses per second, a circumferential capsulotomy
was created from anteromedial to lateral. Activation of the laser along
this line of incision (Figure-5) was continued through the renal parenchyma
until the lower pole was completely excised. Defocusing the laser and
using fibrin glue at the resected margin controlled residual bleeding.
The procedure was performed successfully
in all animals with minimum bleeding (< 50 ml). Operative time was
short due to no hilar dissection and minimum renal mobilization. The only
shortcoming of the technique noted by the authors was compromised visualization
secondary to the splattering of blood on the camera during the resection.
This was partially avoided by keeping the camera at a distance from the
line of resection. Initial clinical evaluation of this technique has begun.
CONCLUSION
Even
in this “golden era” of laparoscopy in urology, some of the
most accomplished laparoscopists have avoided performing routine laparoscopic
partial nephrectomies. The reason is evident if one looks at the numerous
techniques that have been illustrated above. Any procedure for which there
are so many different techniques surely has not found one that works optimally.
Even in the short time it has taken to prepare this article two new techniques
have been published in the literature.
For a procedure to be performed laparoscopically
it must demonstrate that the laparoscopic approach has the same or better
efficacy with decreased morbidity when compared to open surgery. This
is evident for laparoscopic radical nephrectomy (30). Whether the same
will hold true for LPN has yet to be determined. Thus far, the reported
techniques have demonstrated success in animal models and in small clinical
series. As a result, LPN is certainly an efficacious procedure applicable
in many cases. Nevertheless, LPN will not replace open partial nephrectomy
for many tumors.
REFERENCES
- Fergany AF, Hafez KS, Novick AC: Long-term results of nephron sparing surgery for localized renal cell carcinoma: 10-year follow-up. J Urol, 163: 442-445, 2000.
- . Clayman RV, Kavoussi LR, Soper NJ, Dierks SM, Meretyk S, Darcy MD, Roemer FD, Pingleton ED, Thomson PG, Long SR: Laparoscopic nephrectomy: initial case report. J Urol, 146: 278-282, 1991.
- Winfield HN, Donovan JF, Godet AS, Clayman RV: Laparoscopic partial nephrectomy: initial case report for benign disease. J Endourol, 7: 521-526, 1993.
- Winfield HN, Donovan JF, Lund GO, Kreder KJ, Stanley KE, Brown BP, Loening SA, Clayman RV: Laparoscopic partial nephrectomy: initial experience and comparison to the open surgical approach. J Urol, 153: 1409-1414, 1995.
- McDougall EM, Elbahnasy AM, Clayman RV: Laparoscopic wedge resection and partial nephrectomy - the Washington University experience and review of the literature. J Soc Laparoendosc Surg, 2: 15-23, 1998.
- Desai MM., Gill IS, Murphy DP, Kaouk JH, Meraney AM, Schweizer DK, Sung GT, Novick AC: Pure laparoscopic partial nephrectomy for renal tumors: duplicating open surgical principles. J Urol, 165, (Suppl. 5): 157 (Abst 87), 2001.
- Kozlowski PM, Winfield HN: Laparoscopic partial nephrectomy and wedge resection. J Endourol, 14: 865-870; discussion 870-871, 2000.
- McDougall EM, Clayman RV, Chandhoke PS, Kerbl K, Stone AM, Wick MR, Hicks M, Figenshau RS: Laparoscopic partial nephrectomy in the pig model. J Urol, 149: 1633-1636, 1993.
- Cadeddu JA, Corwin TS, Traxer O, Collick C, Saboorian HH, Pearle MS: Hemostatic laparoscopic partial nephrectomy: cable-tie compression. Urology, 57: 562-566, 2001.
- Cadeddu JA, Corwin TS: Cable tie compression to facilitate laparoscopic partial nephrectomy. J Urol, 165: 177-178, 2001.
- Gill IS, Munch LC, Clayman RV, McRoberts JW, Nickless B, Roemer FD: A new renal tourniquet for open and laparoscopic partial nephrectomy. J Urol, 154: 1113-1116, 1995.
- Gill IS, Munch LC, Clayman RV, McRoberts JW, Nickless B, Roemer FD: A new renal tourniquet for open and laparoscopic partial nephrectomy. J Urol, 154: 1113-1116, 1995.
- Elashry OM, Wolf JS Jr, Rayala HJ, McDougall EM, Clayman RV: Recent advances in laparoscopic partial nephrectomy: comparative study of electrosurgical snare electrode and ultrasound dissection. J Endourol, 11: 15-22, 1997.
- Collyer W, Landman J, Olweny E, Andreoni C, Kibel A, Andiole GL, Clayman RV, Bostwick DG: Use of a novel electrosurgical snare to perform laparoscopic partial neprectomy in a porcine model. J Urol, 165, (Suppl. 5): 157 (Abst 644), 2001.
- Stifelman MD, Sosa RE, Nakada SY, Shichman SJ: Hand-assisted laparoscopic partial nephrectomy. J Endourol, 15: 161-164, 2001.
- Wolf JS Jr, Moon TD, Nakada SY: Hand assisted laparoscopic nephrectomy: comparison to standard laparoscopic nephrectomy. J Urol, 160: 22-27, 1998.
- Jackman SV, Cadeddu JA, Chen RN, Micali S, Bishoff JT, Lee BR, Moore RG, Kavoussi LR: Utility of the harmonic scalpel for laparoscopic partial nephrectomy. J Endourol, 12: 441-444, 1998.
- Harmon WJ, Kavoussi LR, Bishoff JT: Laparoscopic nephron-sparing surgery for solid renal masses using the ultrasonic shears. Urology, 56: 754-759, 2000.
- Janetschek G, Daffner P, Peschel R, Bartsch G: Laparoscopic nephron sparing surgery for small renal cell carcinoma. J Urol, 159: 1152-1155, 1998.
- Gettman MT, Bishoff JT, Su LM, Chan D, Kavoussi LR, Jarrett TW, Cadeddu JA: Hemostatic laparoscopic partial nephrectomy: initial experience with the radiofrequency coagulation-assisted technique (1). Urology, 58: 8-11, 2001.
- Papachristou DN and Barters R: Resection of the liver with a water jet. Br J Surg, 69: 93-94, 1982.
- Terzis AJ, Nowak G, Rentzsch O, Arnold H, Diebold J, Baretton G: A new system for cutting brain tissue preserving vessels: water jet cutting. Br J Neurosurg, 3: 361-366, 1989.
- Lipshitz I, Bass R, Loewenstein A: Cutting the cornea with a waterjet keratome. J Refract Surg, 12: 184-186, 1996.
- Rau HG, Meyer G, Jauch KW, Cohnert TU, Buttler E, Schildberg FW: Liver resection with the water jet: conventional and laparoscopic surgery. Chirurg, 67: 546-551, 1996.
- Shekarriz H, Shekarriz B, Upadhyay J, Burk C, Wood DP Jr, Bruch HP: Hydro-jet assisted laparoscopic partial nephrectomy: initial experience in a porcine model. J Urol, 163: 1005-1008, 2000.
- Yoshimura K, Okubo K, Ichioka K, Terada N, Matsuta Y, Arai Y: Laparoscopic partial nephrectomy with a microwave tissue coagulator for small renal tumor. J Urol, 165(6 Pt 1): 1893-1896, 2001.
- Tabuse K, Katsumi M, Kobayashi Y, Noguchi H, Egawa H, Aoyama O, Kim H, Nagai Y, Yamaue H, Mori K: Microwave surgery: hepatectomy using a microwave tissue coagulator. World J Surg, 9: 136-143, 1985.
- Naito S, Nakashima M, Kimoto Y, Nakamura M, Kotoh S, Tanaka M, Kumazawa J: Application of microwave tissue coagulator in partial nephrectomy for renal cell carcinoma. J Urol, 159: 960-962, 1998.
- Muraki J, Cord J, Addonizio JC, Eshghi M, Schwalb DM, Armenakas N, Nagamatsu GR: Application of microwave tissue coagulation in partial nephrectomy. Urology, 37: 282-287, 1991.
- Dunn MD, Portis AJ, Shalhav AL, Elbahnasy AM, Heidorn C, McDougall EM, Clayman RV: Laparoscopic versus open radical nephrectomy: a 9-year experience. J Urol, 164: 1153-1159, 2000.
_________________________
Received: September 4, 2001
Accepted: September 30, 2001
_______________________
Correspondence address:
Dr. Jeffrey A. Cadeddu
The University of Texas
Department of Urology
Southwestern Medical Center
5323 Harry Hines Blvd.
Dallas, Texas 75390-9110, USA
Fax: + + (1) (214) 648-8786