DEEP-SEATED
SARCOMAS OF THE PENIS
(
Download pdf )
ALBERTO A. ANTUNES, LUCIANO J. NESRALLAH, PIERRE D. GONCALVES, YURI A. FERREIRA, JOAO C. CAMPAGNARI, MIGUEL SROUGI
Portuguese Beneficence Hospital of Sao Paulo and Syrian Lebanese Hospital, Sao Paulo, SP, Brazil
ABSTRACT
Mesenchymal
neoplasias represent 5% of tumors affecting the penis. Due to the rarity
of such tumors, there is no agreement concerning the best method for staging
and managing these patients.
Sarcomas of the penis can be classified
as deep-seated if they derive from the structures forming the spongy body
and the cavernous bodies. Superficial lesions are usually low-grade and
show a small tendency towards distant metastasis. In contrast, deep-seated
lesions usually show behavior that is more aggressive and have poorer
prognosis.
The authors report 3 cases of deep-seated
primary sarcomas of the penis and review the literature on this rare and
aggressive neoplasia.
Key
words: penis; sarcoma; neoplasm metastasis
Int Braz J Urol. 2005; 31: 245-50
INTRODUCTION
Cancer
of the penis is infrequent, with an incidence ranging from 0.6 to 1/100,000
patients in developed countries. Epidermoid carcinoma is the dominant
histological type; however, other tumors, including basal cell carcinoma
and melanoma, can be found as well (1). Malignant and benign mesenchymal
tumors represent 5% of tumors affecting this organ (2).
The sarcomas of the penis can be classified
as superficial or deep-seated according to the tissues from which they
derive (3). Superficial lesions rarely reach deep tissues, are usually
low-grade and show a small tendency to distant metastases. In contrast,
deep-seated lesions, which include those originating from the glans, those
involving the smooth muscle of the spongy and/or cavernous bodies, and
those representing advanced lesions that were initially superficial, usually
show more aggressive behavior and have poorer prognosis (4).
In the present study, the authors report
3 cases of primary deep-seated sarcomas of the penis and review the literature
on this rare and aggressive neoplasia.
CASES REPORT
Case
1
A 61-year old Caucasian man presented penile
pain and a tumor at the base of the penis for 60 days. Physical examination
of the penis revealed a constant state of semi-erection, which the patient
reported as having started 30 days earlier. On palpation, a tumor mass
with hardened consistency was observed in the pre-pubic region measuring
approximately 5 cm in diameter and extending to the right cavernous body
and perineal region.
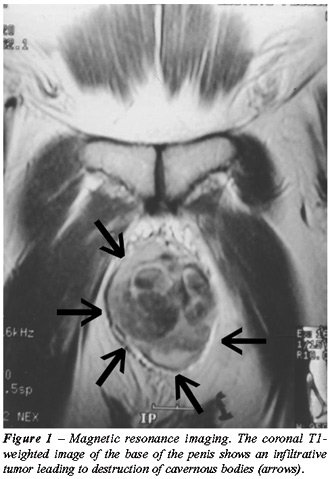
Laboratory tests, chest x-ray and abdominal
ultrasound (USG) were normal. Magnetic resonance imaging (MRI) of the
pelvis showed a solid infiltrative mass at the base of the penis and signs
suggestive of thrombosis in the cavernous bodies (Figure-1). There was
no evidence of enlarged lymph nodes.
The patient underwent emasculation (Figure-2)
and definitive suprapubic cystostomy with closure of the urethral stump
at the level of the membranous urethra due to the perineal extension of
the tumor. There were no postoperative complications and the patient was
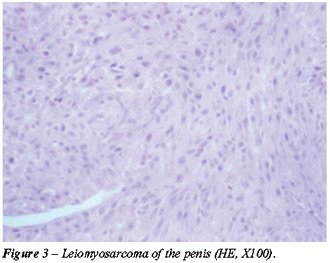
discharged from the hospital on the 4th postoperative day. Pathological
examination revealed leiomyosarcoma involving the cavernous bodies and
extending to the deep perineal planes (Figure-3). Surgical margins were
free from neoplasia.

One month following surgery, patient presented
respiratory stress and the radiological examination revealed the presence
of bilateral pulmonary nodules and metastases characteristics. Chemotherapy
was then started with adriamycin, ifosfamide and dimethy-l-triazeno-imidazol-carboxamide
(DTIC). Upon completion of chemotherapy, the patient presented a reduction
in pulmonary lesions but he died in the eighth postoperative month.
Case
2
A 56-year old man complained of a painful
perineal tumor for 2 months. Physical examination revealed a fixed perineal
mass measuring approximately 6.0 cm in diameter.
Pelvic computerized tomography revealed
a solid nodule measuring 6.5 cm with involvement of cavernous bodies.
Laboratory tests were normal, as were radiological examinations of the
chest and abdomen.
Emasculation was performed with closure
of the urethral stump followed by definitive cystostomy. The patient evolved
with no intercurrences and was discharged from the hospital on the 5th
postoperative day.
The pathological examination revealed leiomyosarcoma
of cavernous bodies with involvement of surgical margins. The patient
was then referred to adjuvant radiotherapy, however he complained of respiratory
stress and control exams evidenced pulmonary nodules suggestive of metastases
at the end of the treatment. Systemic chemotherapy was indicated, but
the patient died in the 9th postoperative month.
Case
3
A 72-year old man presented perineal discomfort
with increasing severity for approximately 6 months, especially during
sexual intercourse. He reported the appearance of a tumor in the penis
30 days earlier. Physical examination revealed a hardened mass measuring
approximately 8.0 x 8.0 cm located at the base of the penis, infiltrating
to the cavernous bodies and extending to the perineum.
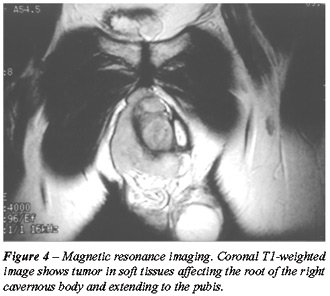
Laboratory tests were normal and pelvic
ultrasound showed no abnormalities. Abdominal and pelvic computerized
tomography showed a solid lesion in cavernous bodies measuring 5.9 cm
in diameter. MRI allowed a more accurate assessment of the local extension
to the perineum (Figure-4). There was no evidence of enlarged lymph nodes
in the chest x-ray.
The patient underwent emasculation where
an extensive involvement was observed in the perineum and right ischiorectal
fossa. Again, suprapubic definitive cystostomy was performed. There were
no postoperative complications and the patient was discharged from hospital
on the 5th postoperative day.
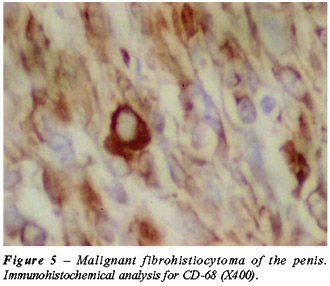
The pathological study together with an
immunohistochemical analysis revealed a fibrohistiocytic sarcomatous tumor
(Figure-5) with imprecise limits located 0.8 cm from the surgical margins.
The patient received adjuvant radiotherapy; however, pulmonary metastasis
was diagnosed in the 3rd postoperative month. The patient received chemotherapy,
which was unsuccessful, and died on the 6th postoperative day.
COMMENTS
It
is estimated that less than 5% of soft tissue sarcomas originate from
the urogenital tract, and they represent only 1 to 2% of neoplasias in
this system (5). In the present study, we present 3 cases of deep-seated
sarcomas of the penis in patients aged between 56 and 72 years old that
were diagnosed based on clinical presentation and pelvic imaging studies.
The cases reflect the lesion’s aggressive characteristics leading
to death after a mean period of 7.6 months despite aggressive surgical
treatment and adjuvant therapy.
Despite being rare, some characteristics
relative to the pattern of recurrence and metastatic dissemination for
sarcomas of the penis have been well established. Local recurrence seems
to be a frequent phenomenon, and total amputation of the penis should
be considered even for superficial lesions (6). On the other hand, regional
metastases appear to occur less frequently, and if there is no apparent
lymph nodal disease, lymphatic dissection is not recommended (7). The
most frequent sites of distant metastases are the lungs, liver and brain
(8).
The best treatment method for sarcomas is
complete resection of the tumor. One study showed that no patient with
retroperitoneal sarcoma had survived beyond 5 years when the sarcomas
had not been not completely resected, while the 5-year survival rate for
patients who underwent complete resection was 48% (9). When investigating
43 patients with urogenital sarcoma, Russo et al. (10) reported that complete
tumor resection was possible in 72% of the cases, and 58% had disease-free
margins. Survival rates after 3 and 5 years were 55% and 40% respectively.
Another factor that contributes to the poor prognosis in these patients
is the fact that no effective response to adjuvant therapy has been obtained
up to this moment. Radiotherapy has been used for final control in local
disease for unresectable tumors and for patients with positive margins,
with chemotherapy being reserved for cases of disseminated disease. In
the series by Russo et al. (10), no patient with disseminated disease
was fully responsive to the use of several chemotherapy regimens.
Some previously described prognostic factors
can help to predict the biological behavior of sarcomas of the penis (10).
These factors are lesion size (larger or smaller than 5 cm), extension
of invasion (superficial vs. deep-seated), complete resection of the lesion,
presence or absence of metastatic disease and expression of the retinoblastoma
gene (11).
Two of the 3 cases described in this study
were diagnosed as leiomyosarcoma. In 1994, 14 cases of deep-seated leiomyosarcomas
of the penis were reviewed (12). The lesions were primarily treated with
local excision (3), amputation (8), external radiotherapy (2) and chemotherapy
(1), and patients were followed during a period from 1 to 72 months (mean
16 months). Eight patients died during follow-up. Among the patients treated
by radical surgery (amputation), 3 developed disseminated disease and
4 died from the disease. All patients treated with chemotherapy or radiotherapy
had local recurrence, with 2 of them presenting disseminated disease.
More recently, Fetsch et al. (13) reported
14 cases of leiomyosarcoma of the penis from a single center. Ages ranged
from 43 to 62 years old (mean 51). The penile shaft was the most frequently
affected site. The size of the lesions ranged between 0.5 and 6 cm. Nine
tumors were superficial, 2 had undetermined location, and 3 were deep-seated.
Immunohistochemical analysis was available for 9 patients (64%), and immunoreactivity
for desmin was present in all such cases. Mean follow-up was 12 years
and 11 months, and, of 9 patients (64%) with available information, 3
had multiple local recurrences, 2 of which were subsequently treated by
wide local excision and partial penectomy. The third patient refused treatment
and developed distant metastasis 10 months after the fourth recurrence.
The main prognostic factors were the lesion’s depth and size.
The third case was diagnosed as a fibrohistiocytic
sarcoma. Despite being the sarcoma that is more frequently described in
the elderly, this histological type rarely involves the urogenital tract
(14). Only 2 cases of malignant fibrohistiocytoma have been described
up to the present time (15,16). These tumors usually display an aggressive
behavior tending to lymphatic dissemination (15,17). Regional lymphadenectomy
apparently does not benefit those patients with sarcomas of the penis
without evidence of lymphatic dissemination, however it is highly recommended
for patients with this type of tumor. In the presence of metastases, chemotherapy
seems to present some benefits (18).
Other types of penile sarcoma have been
described in the literature. According to records from the Armed Forces
Institute of Pathology, Kaposi’s sarcoma is the most common histological
type, surpassing the cases of leiomyosarcoma by a 2:1 ratio. In contrast
to the latter, the Kaposi’s sarcomas are strongly reactive to CD34
and CD31 and do not show desmin expression. Finally, sarcomatoid carcinomas
must always be remembered when a penile sarcoma is diagnosed. The immunohistochemical
analysis for keratin pattern and extension can distinguish between both
tumors (13).
Though radical surgery with negative margins
is the treatment that provides the best results, our patients quickly
evolved to disseminated disease, with the lungs being the most frequent
site for metastasis. When a perineal urethrostomy is impossible, and if
the patient’s clinical conditions allow, performing a continent
urinary shunt might make social living more acceptable for these patients,
since they would not have to use a cystostomy bag (19).
The authors conclude that sarcomas of penis
are rare tumors and usually have poor prognosis when they involve deep-seated
lesions. The analysis of prognostic factors can help to identify those
patients at higher risk for disease progression. The complete tumor resection
with negative surgical margins whenever possible seems to offer the best
chances of healing. No effective treatment for disseminated disease has
been developed up to the present time.
REFERENCES
- Dehner LP, Smith BH: Soft tissue tumors of the penis. A clinicopathologic study of 46 cases. Cancer. 1970; 25: 1431-47.
- Lucia MS, Miller GJ: Histopathology of malignant lesions of the penis. Urol Clin North Am. 1992; 19: 227-46.
- Pratt RM, Ross RT: Leiomyosarcoma of the penis. A report of a case. Br J Surg. 1969; 56: 870-2.
- Trojani M, Contesso G, Coindre JM, Rouesse J, Bui NB, de Mascarel A, et al.: Soft-tissue sarcomas of adults; study of pathological prognostic variables and definition of a histopathological grading system. Int J Cancer. 1984; 33: 37-42.
- Herr HR: Sarcomas of the Urinary Tract. In: de Kernion JB, Paulson DF (eds.), Genitourinary Cancer Management. Philadelphia, Lea & Febiger. 1987; pp. 259-70.
- Webber RJ, Alsaffar N, Bissett D, Langlois NE: Angiosarcoma of the penis. Urology. 1998; 51: 130-1.
- Lynch Jr. DF, Pettaway CA: Tumors of the Penis. In: Walsh PC, Retik AB, Vaughan Jr. ED, Wein AJ (eds.), Campbell’s Urology, 8th ed. Philadelphia, WB Saunders. 2002; pp. 2945-81.
- Antoneli CB, Novaes PE, Alves AC, Cardoso H, Lopes A: Rhabdomyosarcoma of the penis in a 15-month-old boy. J Urol. 1998; 160: 2200-1.
- Zhang G, Chen KK, Manivel C, Fraley EE: Sarcomas of the retroperitoneum and genitourinary tract. J Urol. 1989; 141: 1107-10.
- Russo P, Brady MS, Conlon K, Hajdu SI, Fair WR, Herr HW et al.: Adult urological sarcoma. J Urol. 1992; 147: 1032-6; discussion 1036-7.
- Cance WG, Brennan MF, Dudas ME, Huang CM, Cordon-Cardo C: Altered expression of the retinoblastoma gene product in human sarcomas. N Engl J Med. 1990; 323: 1457-62.
- Pow-Sang MR, Orihuela E: Leiomyosarcoma of the penis. J Urol. 1994; 151: 1643-5.
- Fetsch JF, Davis Jr CJ, Miettinen M, Sesterhenn IA: Leiomyosarcoma of the penis: a clinicopathologic study of 14 cases with review of the literature and discussion of the differential diagnosis. Am J Surg Pathol. 2004; 28: 115-25.
- Enzinger FM, Weiss SW: Soft Tissue Tumors. St Louis, Mosby. 1983; pp. 116-98.
- Parsons MA, Fox M: Malignant fibrous histiocytoma of the penis. Eur Urol. 1988; 14: 75-6.
- Fletcher CD, Lowe D: Inflammatory fibrous histiocytoma of the penis. Histopathology. 1984; 8: 1079-84.
- Sclama AO, Berger BW, Cherry JM, Young JD Jr: Malignant fibrous histiocytoma of the spermatic cord: the role of retroperitoneal lymphadenectomy in management. J Urol. 1983; 130: 577-9.
- Williamson JC, Johnson JD, Lamm DL, Tio F: Malignant fibrous histiocytoma of the spermatic cord. J Urol. 1980; 123: 785-8.
- Lemelle JL, Simo AK, Schmitt M: Comparative study of the Yang-Monti channel and appendix for continent diversion in the Mitrofanoff and Malone principles. J Urol. 2004; 172: 1907-10.
_______________________
Received: January 17, 2005
Accepted after revision: May 3, 2005
_______________________
Correspondence address:
Dr. Alberto Azoubel Antunes
Rua Três de Maio, 17/31
São Paulo, SP, 04044-020, Brazil
Phone: + 55 11 5573-5385
E-mail: betoazoubel@yahoo.com.br